 Higher acuity cases such as joint replacement and spinal fusions have moved into the ambulatory surgery center setting over the past few years as minimally invasive techniques allow surgeons to perform traditionally inpatient procedures in an outpatient setting.
The anesthesiologist plays a crucial role in making these cases successful. If patients have a great experience, appropriate pain expectations and continue to make progress after they return home, they’re likely to recommend the center to others and revisit the next time they need a procedure.
“When a patient says they didn’t have a good experience and felt sick, we just can’t cut that person loose. We have to check up on them and I think ASCs do a great job of looking at the patient surveys and following up,” says Charles Tullius, MD, an anesthesiologist in Savannah, Ga. “If the patient has one knee done at the center, they’ll return when they...
Higher acuity cases such as joint replacement and spinal fusions have moved into the ambulatory surgery center setting over the past few years as minimally invasive techniques allow surgeons to perform traditionally inpatient procedures in an outpatient setting.
The anesthesiologist plays a crucial role in making these cases successful. If patients have a great experience, appropriate pain expectations and continue to make progress after they return home, they’re likely to recommend the center to others and revisit the next time they need a procedure.
“When a patient says they didn’t have a good experience and felt sick, we just can’t cut that person loose. We have to check up on them and I think ASCs do a great job of looking at the patient surveys and following up,” says Charles Tullius, MD, an anesthesiologist in Savannah, Ga. “If the patient has one knee done at the center, they’ll return when they...
Leaders in medicine and health policy are focusing on a new component of care: appropriateness. Only those medical services and interventions that are likely to help and not harm the patient and that represent value (cost/quality) are appropriate. The real issue is, of course, knowing which services are appropriate.
The Choosing Wisely® campaign, an initiative of the American Board of Internal Medicine Foundation, aims to promote conversations between physicians and patients by helping patients choose care that is:
Supported by evidence
Not duplicative of other tests or procedures already received
Free from harm
Truly necessary
In response to this challenge, more than 40 national organizations including the American Society of Anesthesiologists have stepped up to the ABIM Foundation’s invitation and identified one or more sets of five tests or procedures commonly used in their field the appropriateness of which should be questioned and discussed with patients. The resulting lists of “Five Things...
Securing the Future for Anesthesia PracticesAs the health care world continues to evolve, offering new technological advances and business models, along with changing laws and regulations, it’s imperative to keep informed. Anesthesiologists, Practice Administrators, CRNAs and others in the anesthesia marketplace now have a great new option when looking to attend a conference on anesthesia practice management: The Advanced Institute for Anesthesia Practice Management.The Advanced Institute for Anesthesia Practice Management is an exciting new conference with new sponsors and a fabulous new venue. Previously known as the Anesthesia Billing & Practice Management Seminar, this new name reflects our commitment to position our conference as the premier educational opportunity for decision makers of anesthesia practices, including Anesthesiologists and Practice Administrators. The conference will take place at the hottest property on the Las Vegas Strip, The Cosmopolitan of Las Vegas, from April 11-13, 2014.The Advanced Institute for Anesthesia Practice Management offers the anesthesia...
No three-word phrase was heard more frequently than “Perioperative Surgical Home” (PSH) at the ASA Practice Management Conference held in Dallas on January 24-26, 2013.
The PSH is ASA’s response to the triple-aim challenge laid down by the Institute for Healthcare Improvement: (1) improving the experience of care, (2) improving the health of populations and (3) reducing per capita costs of health care. “The PSH,” according to ASA, “is an innovative model that will improve patient care and health care delivery, and reduce costs by implementing a seamless continuity of care from the moment surgery is planned, through recovery and discharge from a medical facility and beyond.”
The PSH model is based on the Patient-Centered Medical Home, the purpose of which is to address the fragmentation of chronic disease management by having a single primary care physician coordinate the patient’s care and engage a team of professionals and the patient in an...
 Just mention endoscopy at an anesthesia conference and see what happens. Few topics elicit such strong but disparate responses. For the anesthesiologist from the East endoscopy has been, and continues to be, his or her fastest growing and most profitable line of business. By contrast, the prevailing view of the physician in the West reflects a very high degree of skepticism. His experience is that the endoscopists don’t really want to work with his group. He interprets payer policy as forcing anesthesia through the same funnel of denial as other services and sees no meaningful light at the end of the tunnel, especially with regard to endoscopy. Such is the challenge to today’s anesthesia practice management: sorting out the realities of facility expectations, surgeon preferences, payer policies and economic realities and, most of all, rising above the prejudice of emotions. Cynicism and the weight of disappointment too often cloud our ability...
Just mention endoscopy at an anesthesia conference and see what happens. Few topics elicit such strong but disparate responses. For the anesthesiologist from the East endoscopy has been, and continues to be, his or her fastest growing and most profitable line of business. By contrast, the prevailing view of the physician in the West reflects a very high degree of skepticism. His experience is that the endoscopists don’t really want to work with his group. He interprets payer policy as forcing anesthesia through the same funnel of denial as other services and sees no meaningful light at the end of the tunnel, especially with regard to endoscopy. Such is the challenge to today’s anesthesia practice management: sorting out the realities of facility expectations, surgeon preferences, payer policies and economic realities and, most of all, rising above the prejudice of emotions. Cynicism and the weight of disappointment too often cloud our ability...
After requesting comments from the public in August 2013 and receiving more than 130 letters, CMS is going forward with modification of its policy on disclosure of physician payment information.
Starting in late March of this year, CMS will evaluate requests for individual physician payment information (or requests for information that combined with other publicly available information could be used to determine total Medicare payments to a physician) on a case-by-case basis under the Freedom of Information Act. In addition, CMS will generate and make available aggregate data sets regarding Medicare physician services for public consumption.
The notice that CMS posted to its official blog on January 14th represents a reversal of policy going back to 1980. The original policy was based on an injunction issued by a federal district court in Florida that barred the government from disclosing identifiable annual Medicare payments to individual physicians. When the district court vacated its injunction...
 The 2014 Current Procedural Terminology® (CPT) edition will have a total of 335 changes, including 175 new codes, 107 revised codes and 47 deleted codes for specialties.
No Anesthesia CPT codes were deleted, revised, or added for 2014. Changes to the 2014 CPT codes may impact some ASA 2014 CROSSWALK® determinations or base units. Anesthesia providers should ensure that they understand the impact of potential revenue or compensation changes due to additions or revisions to the ASA 2014 CROSSWALK (Please refer to Appendix A – Summary of Additions and Revisions in the 2014 ASA CROSSWALK for a complete list of the additions or revisions).
Pain management providers should take note of the additions and deletions in the chemodenervation subsection of the nervous system section of CPT 2014.
Nearly one-quarter of this year’s CPT code changes resulted from an ongoing two-year effort to revise gastroenterology codes to capture...
The 2014 Current Procedural Terminology® (CPT) edition will have a total of 335 changes, including 175 new codes, 107 revised codes and 47 deleted codes for specialties.
No Anesthesia CPT codes were deleted, revised, or added for 2014. Changes to the 2014 CPT codes may impact some ASA 2014 CROSSWALK® determinations or base units. Anesthesia providers should ensure that they understand the impact of potential revenue or compensation changes due to additions or revisions to the ASA 2014 CROSSWALK (Please refer to Appendix A – Summary of Additions and Revisions in the 2014 ASA CROSSWALK for a complete list of the additions or revisions).
Pain management providers should take note of the additions and deletions in the chemodenervation subsection of the nervous system section of CPT 2014.
Nearly one-quarter of this year’s CPT code changes resulted from an ongoing two-year effort to revise gastroenterology codes to capture...
Hardly a week goes by without news of the loss of a computer containing thousands of patient records. It is all too easy for medical practices and health systems to suffer data breaches, and the financial consequences can be severe. When a breach of patient data is found and reported, healthcare providers and legal business associates can be liable for penalties of up to $1.5 million for violations of a single HIPAA provision.
The Department of Health and Human Services’ Office of Civil Rights (OCR) recently made it clear that an actual breach and disclosure of electronic Protected Health Information (ePHI) is not necessary—there may be liability for not having policies and procedures in place to address the breach notification provisions published in the HIPAA Omnibus Rule in January 2013. The Breach Notification Rule requires covered entities (healthcare providers, health plans, healthcare clearinghouses) to notify individuals and OCR (and in some cases...
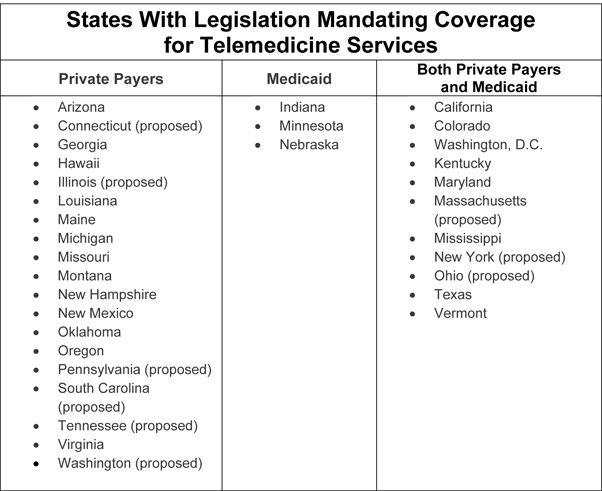 It is time for us to begin to familiarize ourselves with the role of telemedicine in anesthesiology. The concept is not entirely new; there have been several articles published on preadmission anesthesia or critical care consultations conducted through telemedicine. The results of a Canadian pilot study that appeared in Anesthesiology in 2004 showed “that preadmission anesthesia consultations using telemedicine technology can be successfully performed. Patients and consulting and attending anesthesiologists are very satisfied with telemedicine consultation.”
Tele-ICU systems are now able to monitor remotely about 10 percent of intensive care unit patients nationwide, as reported in the New York Times on April 14, 2013. We suspect that there may be more extensive applications right around the corner, and we hope to lay the groundwork for understanding these new applications as they arrive.
“Telemedicine” is commonly defined as the delivery of medical services and the sharing of medical knowledge between different locations using telecommunications systems. According...
It is time for us to begin to familiarize ourselves with the role of telemedicine in anesthesiology. The concept is not entirely new; there have been several articles published on preadmission anesthesia or critical care consultations conducted through telemedicine. The results of a Canadian pilot study that appeared in Anesthesiology in 2004 showed “that preadmission anesthesia consultations using telemedicine technology can be successfully performed. Patients and consulting and attending anesthesiologists are very satisfied with telemedicine consultation.”
Tele-ICU systems are now able to monitor remotely about 10 percent of intensive care unit patients nationwide, as reported in the New York Times on April 14, 2013. We suspect that there may be more extensive applications right around the corner, and we hope to lay the groundwork for understanding these new applications as they arrive.
“Telemedicine” is commonly defined as the delivery of medical services and the sharing of medical knowledge between different locations using telecommunications systems. According...
Anesthesiologists and other physicians who provided out-of-network services to Aetna patients for part or all of the period from 2003 to 2013 may be eligible for a share of the $120 million settlement agreement in the Aetna usual-and-customary (UCR) class action lawsuit.
This litigation arose out of the use by Aetna and other health plans of the Ingenix claims database and certain other reimbursement practices with respect to out-of-network services and supplies, allegedly resulting in artificially reduced payments. The settlement agreement received preliminary approval from the federal district court in Newark, New Jersey in August 2013. A final hearing to consider the “fairness, reasonableness and adequacy” of the agreement is scheduled for March 18, 2014.
Physicians have three choices with respect to the Aetna UCR litigation:
File a claim and share in the ultimate distribution of the Net Settlement Fund; or
Request exclusion from the Class by the deadline of February...
Just like the physical universe, the anesthesia practice universe continues to expand with increasing speed—or at least that is how it seems. The number and breadth of the challenges we face are larger than ever. To the familiar concerns such as disappointing payment rates, declining hospital income support and growing service demands, we can add the confusion and worries created by Obamacare and explosion of work occasioned by information technology. In most challenges, we know, there are also opportunities, some more accessible than others, of course.
ABC senior staff keep their eyes on practice management trends in order to help our clients (and our readers) understand and do well in the changing landscape. The most important challenges and opportunities that we see for 2014 include the following:
Rollout of the Affordable Care Act (ACA). Expect more business uncertainty. Fifteen of the 16 key provisions of the ACA will take effect in...
 Clinicians in the specialty of anesthesiology have much for which we should be proud. Advances in our specialty have made the anesthetic experience both safer and more convenient even as we have advanced the care of our patients both in terms of who can safely receive anesthesia and where it is delivered. In fact, the rest of medicine and health care generally views us as pioneers in the patient safety movement.
Anesthesiology blazed the patient safety trail utilizing a variety of approaches: prudent adoption of improved technology, advances in pharmacology, advanced monitoring techniques, adoption of clinical practice guidelines and standards and by adopting some basic system theory and team-based behavioral principles and models to name just a few. Today, patients with even significant underlying health issues have higher expectations of successful surgical experiences than was thought possible a generation ago. These advances, embraced by us and persistent in our application,...
Clinicians in the specialty of anesthesiology have much for which we should be proud. Advances in our specialty have made the anesthetic experience both safer and more convenient even as we have advanced the care of our patients both in terms of who can safely receive anesthesia and where it is delivered. In fact, the rest of medicine and health care generally views us as pioneers in the patient safety movement.
Anesthesiology blazed the patient safety trail utilizing a variety of approaches: prudent adoption of improved technology, advances in pharmacology, advanced monitoring techniques, adoption of clinical practice guidelines and standards and by adopting some basic system theory and team-based behavioral principles and models to name just a few. Today, patients with even significant underlying health issues have higher expectations of successful surgical experiences than was thought possible a generation ago. These advances, embraced by us and persistent in our application,... 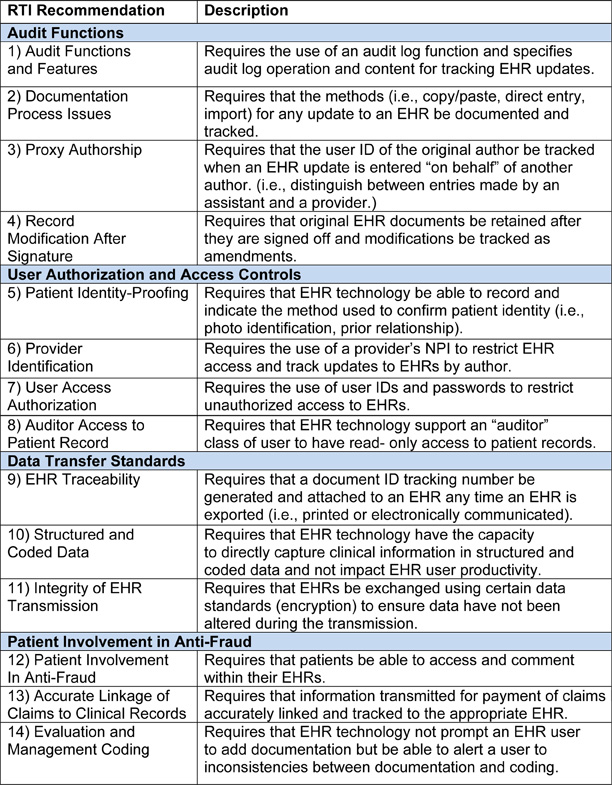 Electronic health records (EHRs) make it easier to document patient care with incorrect information, not just with desirable data. To put it bluntly, as does the Health and Human Services Office of the Inspector General (OIG) in its just-released report Not All Recommended Fraud Safeguards Have Been Implemented in Hospital EHR Technology, “Experts in health information technology caution that EHR technology can make it easier to commit fraud.”
The technology can also facilitate unintentional errors, particularly if the provider is not certain whether he or she is reporting a case in perfect compliance with Medicare requirements. Consider the copy-and-paste feature of many software applications (including Windows). This feature allows providers and other users to retrieve information from one place or one record and place it in another through a few mouse-clicks. If a pain physician knows that a carrier will only deem repeat facet joint injections medically necessary “when the patient...
Electronic health records (EHRs) make it easier to document patient care with incorrect information, not just with desirable data. To put it bluntly, as does the Health and Human Services Office of the Inspector General (OIG) in its just-released report Not All Recommended Fraud Safeguards Have Been Implemented in Hospital EHR Technology, “Experts in health information technology caution that EHR technology can make it easier to commit fraud.”
The technology can also facilitate unintentional errors, particularly if the provider is not certain whether he or she is reporting a case in perfect compliance with Medicare requirements. Consider the copy-and-paste feature of many software applications (including Windows). This feature allows providers and other users to retrieve information from one place or one record and place it in another through a few mouse-clicks. If a pain physician knows that a carrier will only deem repeat facet joint injections medically necessary “when the patient...  As we head into the final quarter of the year, the departmental and group stability that anesthesiologists seek remain elusive. Hospitals and health systems continue their drive toward consolidation. National management companies report more and more acquisitions of anesthesia practices. The Affordable Care Act’s Health Insurance Exchanges will have begun to enroll beneficiaries by the time this issue of the Communique is in your hands, with much of the uncertainty over the functioning unresolved. Indeed, after forty attempts by the House of Representatives to repeal the Affordable Care Act, much of the law will be in effect by January 1, 2014, unless there is a successful forty-first or forty-second attempt, which strikes us as unlikely. Defunding may yet kill the ACA, but for now we must proceed on the assumption that the law will be very much with us next year.
The new environment demands accountability as well as “value” and...
As we head into the final quarter of the year, the departmental and group stability that anesthesiologists seek remain elusive. Hospitals and health systems continue their drive toward consolidation. National management companies report more and more acquisitions of anesthesia practices. The Affordable Care Act’s Health Insurance Exchanges will have begun to enroll beneficiaries by the time this issue of the Communique is in your hands, with much of the uncertainty over the functioning unresolved. Indeed, after forty attempts by the House of Representatives to repeal the Affordable Care Act, much of the law will be in effect by January 1, 2014, unless there is a successful forty-first or forty-second attempt, which strikes us as unlikely. Defunding may yet kill the ACA, but for now we must proceed on the assumption that the law will be very much with us next year.
The new environment demands accountability as well as “value” and...  The Centers for Medicare and Medicaid Services (CMS) released the 1369-page final regulations containing the changes to the Physician Fee Schedule for 2014 (the “Final Rule”) on the Wednesday before Thanksgiving. Updates and provisions of interest to anesthesiologists include the 2014 conversion factor and changes to the Physician Quality Reporting System (PQRS) and Value-Based Payment Modifier requirements.
Conversion Factor
The national average anesthesia conversion factor (CF) is set at $17.2283 for 2014, down from $21.9243 this year. This includes a one-percent increase in the Medicare Economic Index for anesthesia services; many other specialties saw no increase or a negative impact.
The general Medicare conversion factor, which applies to pain medicine, critical care, evaluation and management and other “flat fee” services, will decrease by 20.1 percent, to $27.2006. In March 2013, CMS had projected a CF decrease of 24.4 percent for 2014.
The announcement of a decrease should not raise an alarm: ...
The Centers for Medicare and Medicaid Services (CMS) released the 1369-page final regulations containing the changes to the Physician Fee Schedule for 2014 (the “Final Rule”) on the Wednesday before Thanksgiving. Updates and provisions of interest to anesthesiologists include the 2014 conversion factor and changes to the Physician Quality Reporting System (PQRS) and Value-Based Payment Modifier requirements.
Conversion Factor
The national average anesthesia conversion factor (CF) is set at $17.2283 for 2014, down from $21.9243 this year. This includes a one-percent increase in the Medicare Economic Index for anesthesia services; many other specialties saw no increase or a negative impact.
The general Medicare conversion factor, which applies to pain medicine, critical care, evaluation and management and other “flat fee” services, will decrease by 20.1 percent, to $27.2006. In March 2013, CMS had projected a CF decrease of 24.4 percent for 2014.
The announcement of a decrease should not raise an alarm: ...  Many anesthesia practices across the country are hybrid entities, consisting of a subgroup of anesthesiologists and CRNAs who provide only surgical and obstetric anesthesia and another subset who spend part or all of their time in the management of chronic pain. The circumstances that have encouraged the development of such entities vary considerably, but it is a common phenomenon across the country in all types of settings.
In some cases, the different sets of providers appear to work quite harmoniously but these are the exceptions rather than the rule. Most struggle with a consistent set of challenges that derive directly from the fundamental differences between the two types of practices. Even a cursory review of any of these practices reveals just how different the criteria are for success in chronic pain as compared to O.R. or obstetric anesthesia. Simply put, the demands of a hospital-based anesthesia practice bear little or no...
Many anesthesia practices across the country are hybrid entities, consisting of a subgroup of anesthesiologists and CRNAs who provide only surgical and obstetric anesthesia and another subset who spend part or all of their time in the management of chronic pain. The circumstances that have encouraged the development of such entities vary considerably, but it is a common phenomenon across the country in all types of settings.
In some cases, the different sets of providers appear to work quite harmoniously but these are the exceptions rather than the rule. Most struggle with a consistent set of challenges that derive directly from the fundamental differences between the two types of practices. Even a cursory review of any of these practices reveals just how different the criteria are for success in chronic pain as compared to O.R. or obstetric anesthesia. Simply put, the demands of a hospital-based anesthesia practice bear little or no...
BREAKING NEWS: CMS released the final 2014 Physician Fee Schedule rule on Wednesday, November 27. The Medicare conversion factor will be reduced by 20.1 percent, not 24.4 percent as projected last March—unless Congress intervenes, as most observers expect will happen. Please see next week’s Alert for more information.
December 2, 2013
One of the longest-running Medicare whistleblower lawsuits, U.S. ex rel. El-Amin v. George Washington University (D.D.C. November 25, 2013), has apparently come to an end, without a trial. Late last month, the United States District Court granted the defendant’s motion for summary judgment, which means that even if the plaintiff’s factual allegations were true, the defendant would prevail as a matter of law.
Four nurse anesthetists then employed by the George Washington University (GWU) brought a qui tam or whistleblower lawsuit against GWU in 1995. They alleged that between 1989 and 1995, GWU had submitted thousands of claims to Medicare...
 At some point toward the beginning of their careers, physicians are required to take the Hippocratic Oath in which the physician covenants to heal the sick or to prescribe measures for the good of the patient. Unfortunately, in an environment in which overdoses on prescription medication are quickly rising to the top of the list of causes of death, zealous adherence to this portion of the Oath could leave pain management physicians exposed to liability. Furthermore, blind adherence to the Oath is not a legal defense to injury or death associated with the misuse or diversion of prescriptions. Luckily, there are steps that pain management physicians can follow early on to promote a beneficial relationship for the patient and to minimize legal risk to the physician. Still, even when preventative steps do not produce the intended results, there are measures that can be taken to legally terminate the relationship with the...
At some point toward the beginning of their careers, physicians are required to take the Hippocratic Oath in which the physician covenants to heal the sick or to prescribe measures for the good of the patient. Unfortunately, in an environment in which overdoses on prescription medication are quickly rising to the top of the list of causes of death, zealous adherence to this portion of the Oath could leave pain management physicians exposed to liability. Furthermore, blind adherence to the Oath is not a legal defense to injury or death associated with the misuse or diversion of prescriptions. Luckily, there are steps that pain management physicians can follow early on to promote a beneficial relationship for the patient and to minimize legal risk to the physician. Still, even when preventative steps do not produce the intended results, there are measures that can be taken to legally terminate the relationship with the... 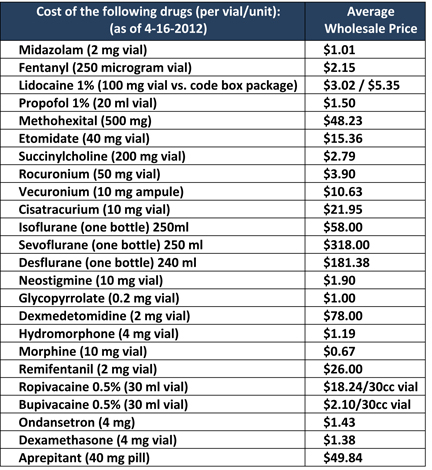 One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...  It’s a tough world out there for anesthesiologists. At least, that’s what many anesthesiologists think.
Many believe that hospital employment is the panacea: the new “safe” career option. And why not—that’s the song that hospitals are singing loud and clear, and it’s the one they’re encouraging you to sing, too, via “alignment.”
Are anesthesiologists being guided into a safe harbor from the storm of uncertainty, or are they being lured by the siren song of a creature lethal to physician success?
Siren Song
In Greek and Roman mythology, sirens lured mariners to their deaths. Lethal creatures that they were, they didn’t kill with knives, spears, or other observable weapons; they didn’t even give rise to a threat.
Instead, they used their enchanting voices in song to lure their victims’ ships aground on the rocky shore.
Today, there are a number of trends creating a storm in the sea of medical practice....
It’s a tough world out there for anesthesiologists. At least, that’s what many anesthesiologists think.
Many believe that hospital employment is the panacea: the new “safe” career option. And why not—that’s the song that hospitals are singing loud and clear, and it’s the one they’re encouraging you to sing, too, via “alignment.”
Are anesthesiologists being guided into a safe harbor from the storm of uncertainty, or are they being lured by the siren song of a creature lethal to physician success?
Siren Song
In Greek and Roman mythology, sirens lured mariners to their deaths. Lethal creatures that they were, they didn’t kill with knives, spears, or other observable weapons; they didn’t even give rise to a threat.
Instead, they used their enchanting voices in song to lure their victims’ ships aground on the rocky shore.
Today, there are a number of trends creating a storm in the sea of medical practice....