Anesthesia Practice Management conferences rarely focus on billing, coding and compliance. The AIAPM focuses on all three because we believe how important these topics are to all attendees including Anesthesiologists, CRNAs, Practice Administrators and Billing Staff. Our goal is to help all anesthesia practices maximize their reimbursements and reduce their compliance risk.The Advanced Institute for Anesthesia Practice Management will be held at the Cosmopolitan of Las Vegas from April 17-19, 2015. Please join us along with the following experts in anesthesia billing, coding and compliance:Devona Slater, CHA, CHC, CMCPPresidentAuditing for Compliance & EducationMarvel J Hammer, RN, CPC, CCS-P, ACS-PM, CHCOMJH ConsultingKelly Dennis, MBA, ACS-AN, CAN-PC, CHCA, CPC, CPC-IPerfect Office Solutions, Inc.Vicki Myckowiak, Esq.Myckowiak Associates, PCJudy Blaszczyk, RN, CPC, ACS-PMAuditing for Compliance & EducationWe also have enlisted experts to enlighten us on the following valuable topics:The Latest in the Anesthesia Merger and Acquisition MarketOne Group's Journey Through the Acquisition ProcessThe Anesthesiologist's Role...
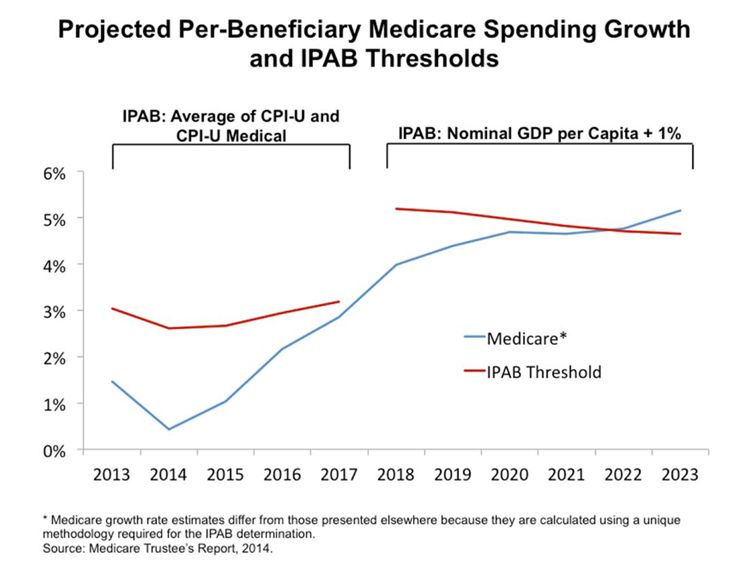 One especially alarming artifact of the Patient Protection and Affordable Care Act (ACA) is the Independent Payment Advisory Board (IPAB). The IPAB is a 15-member panel charged with making proposals to “reduce cost growth” and “improve quality of care for Medicare beneficiaries.” It is required to recommend cost-saving initiatives in any year in which per capita spending exceeds a threshold determined by the government. In addition, the Commission is authorized to make recommendations to “constrain the rate of growth in the private sector.”
Right now, the IPAB is also a phantom. Although the ACA called for the Commission to be in place and to make its first set of recommendations by January 2014, no members have ever been appointed and no nominations are even in the works.
Nevertheless, opposition to the IPAB is as strong today as when the draft that became the ACA first appeared. Senator John Cornyn (R-TX) reintroduced...
One especially alarming artifact of the Patient Protection and Affordable Care Act (ACA) is the Independent Payment Advisory Board (IPAB). The IPAB is a 15-member panel charged with making proposals to “reduce cost growth” and “improve quality of care for Medicare beneficiaries.” It is required to recommend cost-saving initiatives in any year in which per capita spending exceeds a threshold determined by the government. In addition, the Commission is authorized to make recommendations to “constrain the rate of growth in the private sector.”
Right now, the IPAB is also a phantom. Although the ACA called for the Commission to be in place and to make its first set of recommendations by January 2014, no members have ever been appointed and no nominations are even in the works.
Nevertheless, opposition to the IPAB is as strong today as when the draft that became the ACA first appeared. Senator John Cornyn (R-TX) reintroduced...  By:
Michael R. Hicks, MD, MBA, MHCM, FACHE Physician Executive, Dallas, TX
Joe Laden Louisville, KY
Background of the Authors:
National anesthesia management companies increase revenue for acquired groups....or do they? This article presents pros and cons for both viewpoints with discussion by two leaders in the field of anesthesia practice management, Michael R. Hicks, MD, MBA, MHCM, FACHE, a physician executive from Dallas, TX and Joe Laden, a practice manager based in Louisville, KY.
Mr. Laden
Over the past several years, anesthesiologists have been increasingly willing to sell their practices to acquiring firms. In a typical transaction, the anesthesiologist practice owners agree to reduce their incomes in return for the purchase of their stock in their practice. The stock payment is usually several times the annual salary reduction. The anesthesiologists benefit by receiving funds now rather than in the future, and this money is taxed at the capital gains rate...
By:
Michael R. Hicks, MD, MBA, MHCM, FACHE Physician Executive, Dallas, TX
Joe Laden Louisville, KY
Background of the Authors:
National anesthesia management companies increase revenue for acquired groups....or do they? This article presents pros and cons for both viewpoints with discussion by two leaders in the field of anesthesia practice management, Michael R. Hicks, MD, MBA, MHCM, FACHE, a physician executive from Dallas, TX and Joe Laden, a practice manager based in Louisville, KY.
Mr. Laden
Over the past several years, anesthesiologists have been increasingly willing to sell their practices to acquiring firms. In a typical transaction, the anesthesiologist practice owners agree to reduce their incomes in return for the purchase of their stock in their practice. The stock payment is usually several times the annual salary reduction. The anesthesiologists benefit by receiving funds now rather than in the future, and this money is taxed at the capital gains rate... 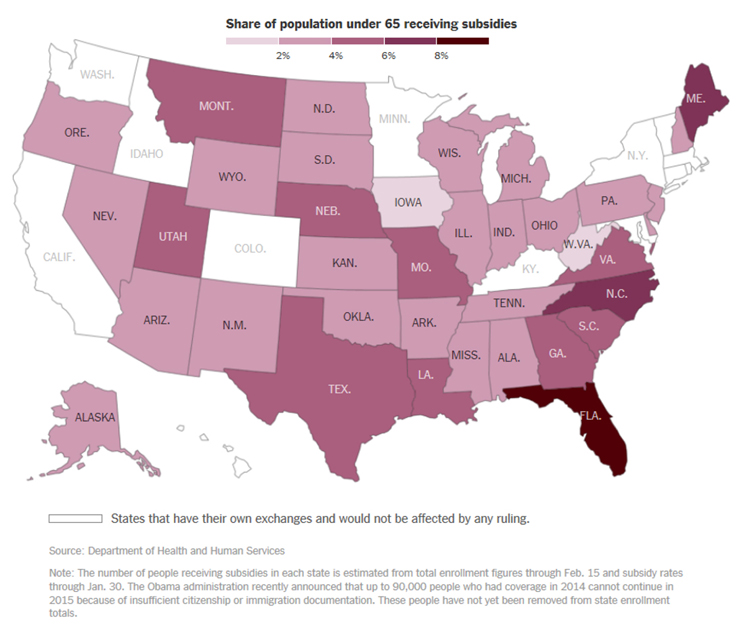 Health policy dominated the news media last week, with the Supreme Court hearing oral arguments in King v. Burwell, the case with the potential to eviscerate Obamacare, on Wednesday March 4. Demonstrators crowded the steps in front of the Court during the hearing; most urged that the Affordable Care Act (ACA) be left intact.
The interest in King v. Burwell is not surprising. If the Court decides in favor of the plaintiffs, between 7.5 and 8.2 million persons in 34 states that have not created their own health insurance exchanges stand to lose the coverage that they have been able to obtain because of the ACA subsidies. Eighty-seven percent of individuals who have signed up in the 34 states are eligible for subsidies, which average about $268 per month. Premiums are expected to increase by about 35-57 percent for those who remain in the federally run exchanges if and when many of...
Health policy dominated the news media last week, with the Supreme Court hearing oral arguments in King v. Burwell, the case with the potential to eviscerate Obamacare, on Wednesday March 4. Demonstrators crowded the steps in front of the Court during the hearing; most urged that the Affordable Care Act (ACA) be left intact.
The interest in King v. Burwell is not surprising. If the Court decides in favor of the plaintiffs, between 7.5 and 8.2 million persons in 34 states that have not created their own health insurance exchanges stand to lose the coverage that they have been able to obtain because of the ACA subsidies. Eighty-seven percent of individuals who have signed up in the 34 states are eligible for subsidies, which average about $268 per month. Premiums are expected to increase by about 35-57 percent for those who remain in the federally run exchanges if and when many of...  Dear Readers, We are entering the new year determined to enhance our engagement with you. Many of you have provided us with comments and questions on articles in past issues, opening the door to new topics and new contributors and at the very least to different perspectives.
If you have read previous issues of the Communiqué, you know that more and more of our content reflects reciprocal and often iterative learning. It is time to open up this process. We want to hear from you. Beginning with the Spring issue, we will add a “Letters to the Editor” section and we hope that you will write to us (editor.communique@anesthesiallc.com) with your observations on any item that has caught your interest. We will forward all correspondence to the author(s) of the article so that they may respond to your comments or queries, and we will do our best to supplement the authors’...
Dear Readers, We are entering the new year determined to enhance our engagement with you. Many of you have provided us with comments and questions on articles in past issues, opening the door to new topics and new contributors and at the very least to different perspectives.
If you have read previous issues of the Communiqué, you know that more and more of our content reflects reciprocal and often iterative learning. It is time to open up this process. We want to hear from you. Beginning with the Spring issue, we will add a “Letters to the Editor” section and we hope that you will write to us (editor.communique@anesthesiallc.com) with your observations on any item that has caught your interest. We will forward all correspondence to the author(s) of the article so that they may respond to your comments or queries, and we will do our best to supplement the authors’...  Anesthesiologists’ role in perioperative medicine is rapidly expanding. It is now sufficiently visible that some surgeons are concerned about turf; see Brian Dunleavy’s article Perioperative Surgical Home Promotes Perioperativists in the February issue of General Surgery News online.
While much of the attention has focused on the services that anesthesiologists might provide in the pre-operative phase of surgical care, some anesthesiologists are providing care after discharge for a period of up to 30 days—and are being paid directly for some of that post-operative care. Medicare has recognized two transitional care management (TCM) codes (CPT™ codes 99495 and 99496) since January 1, 2013. Private payers may cover the service, but few, if any, have chosen to do so.
This year, the national unadjusted Medicare payment amounts for services provided in the facility setting are $111.91 (99495) and $161.25 (99496). For some anesthesiology practices, it makes financial as well as clinical sense to provide...
Anesthesiologists’ role in perioperative medicine is rapidly expanding. It is now sufficiently visible that some surgeons are concerned about turf; see Brian Dunleavy’s article Perioperative Surgical Home Promotes Perioperativists in the February issue of General Surgery News online.
While much of the attention has focused on the services that anesthesiologists might provide in the pre-operative phase of surgical care, some anesthesiologists are providing care after discharge for a period of up to 30 days—and are being paid directly for some of that post-operative care. Medicare has recognized two transitional care management (TCM) codes (CPT™ codes 99495 and 99496) since January 1, 2013. Private payers may cover the service, but few, if any, have chosen to do so.
This year, the national unadjusted Medicare payment amounts for services provided in the facility setting are $111.91 (99495) and $161.25 (99496). For some anesthesiology practices, it makes financial as well as clinical sense to provide...  By:
Richard P. Dutton, MD, MBA Chief Quality Officer, American Society of Anesthesiologists Executive Director, Anesthesia Quality Institute, Schaumburg, IL
Matthew T. Popovich, Ph.D. Director of Quality and Regulatory Affairs, American Society of Anesthesiologists, Washington, D.C.
The fact is, folks, that the Qualified Clinical Data Registry (QCDR)—and pay for performance reporting in general— is ridiculously complex. And the rules are changing every year. This article will lay out some of the basics, using simple lists and bullets, in the hope of making the options more intuitive. We wish to acknowledge also the editorial assistance of Karin Bierstein, herself an expert, who will correct any inadvertent misstatements we might make. Between the three of us we should be able to lift the fog a little bit.
Let’s begin with some Q&A:
Do I have to participate in performance reporting?
Leaving aside the local advantages of an effective...
By:
Richard P. Dutton, MD, MBA Chief Quality Officer, American Society of Anesthesiologists Executive Director, Anesthesia Quality Institute, Schaumburg, IL
Matthew T. Popovich, Ph.D. Director of Quality and Regulatory Affairs, American Society of Anesthesiologists, Washington, D.C.
The fact is, folks, that the Qualified Clinical Data Registry (QCDR)—and pay for performance reporting in general— is ridiculously complex. And the rules are changing every year. This article will lay out some of the basics, using simple lists and bullets, in the hope of making the options more intuitive. We wish to acknowledge also the editorial assistance of Karin Bierstein, herself an expert, who will correct any inadvertent misstatements we might make. Between the three of us we should be able to lift the fog a little bit.
Let’s begin with some Q&A:
Do I have to participate in performance reporting?
Leaving aside the local advantages of an effective...
The compliance deadline for ICD-10, as you have read many times, is October 1, 2015. After three delays since the deadline was originally set for 2011, there may be some doubt—not to say cynicism—about whether the October 1st date will slip too. It may—but the majority of viewers believe that the transition to ICD-10 codes will occur as scheduled.
On February 11, 2015, the U.S. House Energy and Commerce Subcommittee on Health held a hearing entitled "Examining ICD-10 Implementation.” The seven witnesses who testified were health industry professionals representing such major players as the American Health Information Management Association (AHIMA), Athena Health, America’s Health Insurance Plans (the commercial payers’ lobby) and 3M Health Information Systems. Six of the seven witnesses adamantly supported October 1st implementation. The seventh, William Jefferson Terry, MD, of the Mobile Urology Group and American Urology Association, made the usual arguments that ICD-10 coding will interfere with treating...
 If you have not spent much time thinking about the impact of the Exchange plans now being offered under Obamacare, you are not alone. For many anesthesia providers and their administrative staff, the specific implications of the Patient Protection and Affordable Care Act (ACA) passed in March 2010 are more or less a black box. As is true of so many issues in healthcare, the devil is in the details; unfortunately this is just one more complicated issue that merits special management focus.
So what are Exchange plans and how do they work? It is important to understand that Exchange plan options are offered in every state. These insurance options are available through the Health Insurance Marketplace at Healthcare.gov. Essentially this provides options for those who are not covered through their employer. In each state where they are offered, private, commercial insurers have contracted to provide coverage at discounted rates. For...
If you have not spent much time thinking about the impact of the Exchange plans now being offered under Obamacare, you are not alone. For many anesthesia providers and their administrative staff, the specific implications of the Patient Protection and Affordable Care Act (ACA) passed in March 2010 are more or less a black box. As is true of so many issues in healthcare, the devil is in the details; unfortunately this is just one more complicated issue that merits special management focus.
So what are Exchange plans and how do they work? It is important to understand that Exchange plan options are offered in every state. These insurance options are available through the Health Insurance Marketplace at Healthcare.gov. Essentially this provides options for those who are not covered through their employer. In each state where they are offered, private, commercial insurers have contracted to provide coverage at discounted rates. For... 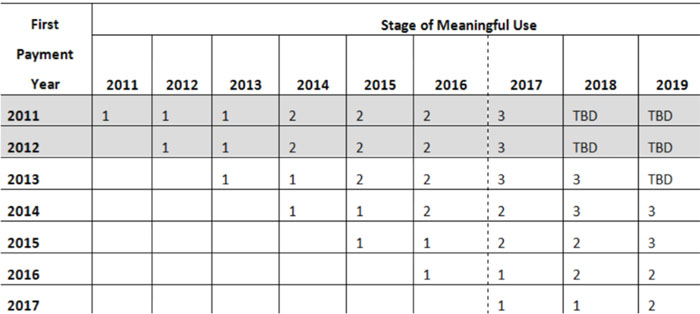 On January 29, CMS stated that it plans to shorten the EHR reporting period from the full year 2015 to 90 days. This will be accomplished through a formal rule-making process in which CMS will attempt to reduce program complexity and the reporting burden on providers including physicians.
Before addressing the requirements for earning MU incentive payments going forward, we would remind anesthesiologists that they benefit from an automatic exemption, based on their Provider, Enrollment, Chain and Ownership System (PECOS) specialty designation. This exemption is particularly important now, since eligible professionals (EPs) who are not exempt—including physicians who have enrolled in PECOS using one of the pain medicine codes rather than the anesthesiology code as their primary specialty designation—will face a one percent (-1%) penalty in 2015 if they have not attested to 2014 MU by February 28, 2015. The penalties will increase to two percent (-2%) in 2016 and three percent...
On January 29, CMS stated that it plans to shorten the EHR reporting period from the full year 2015 to 90 days. This will be accomplished through a formal rule-making process in which CMS will attempt to reduce program complexity and the reporting burden on providers including physicians.
Before addressing the requirements for earning MU incentive payments going forward, we would remind anesthesiologists that they benefit from an automatic exemption, based on their Provider, Enrollment, Chain and Ownership System (PECOS) specialty designation. This exemption is particularly important now, since eligible professionals (EPs) who are not exempt—including physicians who have enrolled in PECOS using one of the pain medicine codes rather than the anesthesiology code as their primary specialty designation—will face a one percent (-1%) penalty in 2015 if they have not attested to 2014 MU by February 28, 2015. The penalties will increase to two percent (-2%) in 2016 and three percent...  Dateline Phoenix
Phoenix. No, not the city in Arizona, but the mythical bird. The one that springs to life from the ashes of its predecessor.
Anesthesia groups, like birds, have a life cycle. Birth to death. Formation to failure.
The group’s founders hatch the concept and bring it into existence. The group obtains business traction in its infancy and grows until it reaches maturity.
But, sooner or later and as inevitable as the sunset, the group begins to decline: the loss of contractual relationships. The unfastening of the bonds that bind the group together. Its eventual dissolution isn’t far off. The flames of death engulf the group.
But unlike natural birds, many dying anesthesia groups have within them the kernel of rebirth. Enter the phoenix.
Death and Praxis
In today’s anesthesia market, we’re seeing two slightly different patterns of anesthesia group decline and death: the failed site of a national or...
Dateline Phoenix
Phoenix. No, not the city in Arizona, but the mythical bird. The one that springs to life from the ashes of its predecessor.
Anesthesia groups, like birds, have a life cycle. Birth to death. Formation to failure.
The group’s founders hatch the concept and bring it into existence. The group obtains business traction in its infancy and grows until it reaches maturity.
But, sooner or later and as inevitable as the sunset, the group begins to decline: the loss of contractual relationships. The unfastening of the bonds that bind the group together. Its eventual dissolution isn’t far off. The flames of death engulf the group.
But unlike natural birds, many dying anesthesia groups have within them the kernel of rebirth. Enter the phoenix.
Death and Praxis
In today’s anesthesia market, we’re seeing two slightly different patterns of anesthesia group decline and death: the failed site of a national or...
Price transparency is playing a more and more critical role in health care. As Costs of Care Executive Director Neel Shah, M.D. has stated, “We make purchasing decisions for every other commodity based on transparent price and quality information (think Yelp, Travelocity). Why not healthcare, too?”
There is a widely-held view that publishing price information could both rein in the enormous range of costs people pay and lower the level of prices in general. This kind of price transparency potentially may allow patients to comparison shop for health care as they would a car, house or television, forcing higher priced providers to lower their prices to stay competitive.
The Patient Protection and Affordable Care Act (ACA) has enabled an additional 15 million individuals to obtain health care insurance. With many of the newly insured (and others) choosing one of the less expensive “bronze” or “silver” plans, which typically cover 60 to...
 The National Practitioner Data Bank (NPDB) was established under Title IV of the Health Care Quality Improvement Act of 1986 and has been operational since September of 1990. The NPDB impacts both anesthesiologists and certified registered nurse anesthetists (CRNAs) as certain entities are required to report adverse actions taken against their licenses, clinical privileges and professional society memberships. The issue of the NPDB most commonly arises under scenarios involving medical malpractice claims as, often, any and all payments made—regardless of whether those payments are made to dispose of a claim or to satisfy a judgment—must be reported to the NPDB.
The Data Bank
According to the NPDB Guidebook,
The intent of [the NPDB] is to improve the quality of health care by encouraging State licensing boards, hospitals and other health care entities, and professional societies to identify and discipline those who engage in unprofessional behavior; and to restrict the ability of...
The National Practitioner Data Bank (NPDB) was established under Title IV of the Health Care Quality Improvement Act of 1986 and has been operational since September of 1990. The NPDB impacts both anesthesiologists and certified registered nurse anesthetists (CRNAs) as certain entities are required to report adverse actions taken against their licenses, clinical privileges and professional society memberships. The issue of the NPDB most commonly arises under scenarios involving medical malpractice claims as, often, any and all payments made—regardless of whether those payments are made to dispose of a claim or to satisfy a judgment—must be reported to the NPDB.
The Data Bank
According to the NPDB Guidebook,
The intent of [the NPDB] is to improve the quality of health care by encouraging State licensing boards, hospitals and other health care entities, and professional societies to identify and discipline those who engage in unprofessional behavior; and to restrict the ability of... 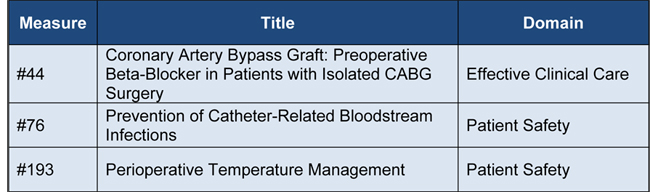 The Physician Quality Reporting System (PQRS) was one of the hottest topics on attendees’ minds at the January 23-25, 2015 ASA Practice Management Conference in Atlanta. There is still a great deal of confusion regarding how anesthesiologists and pain physicians can satisfy the reporting requirements and avoid the penalties. In addition to explanations given at the Conference, the following recent publications clarify those requirements:
CMS 2015 PQRS Implementation Guide; 2015 PQRS Measure-Applicability Validation (MAV) Process for Claims-Based Reporting of Individual Measures
ASA 2015 PQRS FAQS, and
MGMA PQRS/Value-Modifier Survival Guide
As most readers know, eligible professionals (EPs) who do not satisfactorily report PQRS measures in 2015 will see a negative two percent (-2%) payment adjustment—government-speak for “penalty”—on all of their Medicare remittances in 2017. The questions most frequently asked are: what quality measures can anesthesiologists, nurse anesthetists, anesthesiologist assistants and pain physicians report? And how many do they have to report? ...
The Physician Quality Reporting System (PQRS) was one of the hottest topics on attendees’ minds at the January 23-25, 2015 ASA Practice Management Conference in Atlanta. There is still a great deal of confusion regarding how anesthesiologists and pain physicians can satisfy the reporting requirements and avoid the penalties. In addition to explanations given at the Conference, the following recent publications clarify those requirements:
CMS 2015 PQRS Implementation Guide; 2015 PQRS Measure-Applicability Validation (MAV) Process for Claims-Based Reporting of Individual Measures
ASA 2015 PQRS FAQS, and
MGMA PQRS/Value-Modifier Survival Guide
As most readers know, eligible professionals (EPs) who do not satisfactorily report PQRS measures in 2015 will see a negative two percent (-2%) payment adjustment—government-speak for “penalty”—on all of their Medicare remittances in 2017. The questions most frequently asked are: what quality measures can anesthesiologists, nurse anesthetists, anesthesiologist assistants and pain physicians report? And how many do they have to report? ...  The American Medical Association 2015 CPT® Codebook is now available. It contains 9,951 total Current Procedural Terminology (CPT) codes and more than 500 code changes: 266 new, 147 deleted and 129 revised codes. The good news for anesthesia providers and coders is that the only change to the anesthesia code section (00100-01999) is the deletion of three codes, all due to low utilization. The deleted codes are:
00452 Anesthesia for procedures on clavicle and scapula; radical surgery
00622 Anesthesia for procedures on thoracic spine and cord; thoracolumbar sympathectomy
00634 Anesthesia for procedures in lumbar region; chemonucleolysis
The bulk of the coding changes for 2015 fall within the surgical section and the impact, if any, regarding most of these changes will become apparent upon the release of the American Society of Anesthesiologists (ASA) 2015 A Guide for Surgery/Anesthesia CPT® Codes 2015 Crosswalk (not available at press time). Since many of these surgical...
The American Medical Association 2015 CPT® Codebook is now available. It contains 9,951 total Current Procedural Terminology (CPT) codes and more than 500 code changes: 266 new, 147 deleted and 129 revised codes. The good news for anesthesia providers and coders is that the only change to the anesthesia code section (00100-01999) is the deletion of three codes, all due to low utilization. The deleted codes are:
00452 Anesthesia for procedures on clavicle and scapula; radical surgery
00622 Anesthesia for procedures on thoracic spine and cord; thoracolumbar sympathectomy
00634 Anesthesia for procedures in lumbar region; chemonucleolysis
The bulk of the coding changes for 2015 fall within the surgical section and the impact, if any, regarding most of these changes will become apparent upon the release of the American Society of Anesthesiologists (ASA) 2015 A Guide for Surgery/Anesthesia CPT® Codes 2015 Crosswalk (not available at press time). Since many of these surgical...
Are we heading toward a health care system in which medical care comes with a money-back guarantee? That would seem to be the ultimate stage of accountability. We do not see anesthesia, pain medicine or any other practices offering to refund payments if patients are not satisfied on the horizon. We are aware of only one instance of a money-back offer in health care: Janssen Pharmaceuticals recently entered into an arrangement with the English National Health Service under which Janssen UK will refund the cost of its hepatitis C drug Olysio for patients who do not successfully clear the virus after 12 weeks. Janssen will also offer free access to pre-treatment blood tests to determine which patients are likely to benefit from treatment. (McKee S. Janssen offers NHS to pay for Olysio failures. PharmaTimes Digital, January 15, 2015.)
Warranties are starting to take hold, however. In the commercial arena, warranties obligate...
Even though there has been a substantial amount of information published regarding the implementation of ICD-10 over the last ten years, there are many misconceptions that continue to plague the physician community. Rumors run rampant; some are valid while others are completely unfounded. Frequently we hear the need for change in healthcare, yet resistance to change continues to stifle our ability to move forward. The unknown is a scary place. It is more comfortable to work with an established system that is flawed rather than implement a new, technologically advanced system. Reflecting back several years ago with the implementation of the 5010 HIPAA electronic transactions standard, many organizations were negatively affected because they were not prepared, yet after some adjustments, 5010 is successfully operating behind the scenes with little to no effort. Let’s review ten questions concerning ICD-10 in an attempt to dispel the myths.
Who developed ICD-10?
The World Health...
If anesthesiologists and pain specialists are like other physicians, at least as far as this question goes, online rating web sites like HealthGrades and Vitals do not provide much useful information on provider quality.
A recent study funded by the American Board of Internal Medicine (ABIM) found that there is little to no association between physicians’ online ratings and how well they score on performance measures or on patient-experience surveys conducted by their own practices. Researchers led by Bradley M. Gray, PhD looked at 1,299 physicians who completed an ABIM Practice Improvement Module® (PIM) in diabetes or hypertension between July 2011 and November 2012. These modules guide physicians through a review of patient data and support quality improvement work and reporting in their practices. PIM patient survey responses and chart abstractions were compared against the ratings physicians received on eight leading, publicly available and free rating websites. Sites were selected from...
If anesthesiologists and pain specialists are like other physicians, at least as far as this question goes, online rating web sites like HealthGrades and Vitals do not provide much useful information on provider quality.
A recent study funded by the American Board of Internal Medicine (ABIM) found that there is little to no association between physicians’ online ratings and how well they score on performance measures or on patient-experience surveys conducted by their own practices. Researchers led by Bradley M. Gray, PhD looked at 1,299 physicians who completed an ABIM Practice Improvement Module® (PIM) in diabetes or hypertension between July 2011 and November 2012. These modules guide physicians through a review of patient data and support quality improvement work and reporting in their practices. PIM patient survey responses and chart abstractions were compared against the ratings physicians received on eight leading, publicly available and free rating websites. Sites were selected from...
Does your practice have any Medicare appeals pending? If you have appealed a decision within the last several years, be prepared to wait a long time for a ruling. The backlog of provider appeals has grown so that the system is heavily overloaded, causing at least a two-year delay for appeals to be heard at the Administrative Law Judge (ALJ) level. One of the key contributing factors is the RAC program. The number of appeal from RAC determinations has grown exponentially since the program began in 2011. In 2013 alone, there was a 506 percent increase in appealed RA program claims over fiscal year 2012, versus a 77 percent increase in appealed claims not related to the RA program during that same period of time.
The RACs are paid a hefty commission of approximately 9.0-12.5 percent for denied claims. They may keep this bounty unless the claim denial is later overturned...