 In last week’s Alert, we summarized the requirements for participating in Medicare’s Physician Quality Reporting System (PQRS) in 2013. One of the major changes to the PQRS program—which we deferred until this week—is the implementation of the Value-Based Payment Modifier (VBM) for groups of 100 or more eligible professionals (EPs), consisting of physicians and CRNAs and others described in detail below.Groups of 100 or more EPs — Watch out for the Value-Based Payment ModifierThe Patient Protection and Affordable Care Act (ACA) requires that Medicare implement a Value-Based Payment Modifier (VBM) that would apply to Medicare fee-for-service payments beginning in 2015. The VBM is intended to pay physicians differentially based on the quality and cost of their care.While CMS must adhere to certain statutory requirements, such as using the modifier to promote shared responsibility and systems-based care, the ACA gives CMS considerable flexibility in terms of implementing the VBM. The 2013 Medicare...
In last week’s Alert, we summarized the requirements for participating in Medicare’s Physician Quality Reporting System (PQRS) in 2013. One of the major changes to the PQRS program—which we deferred until this week—is the implementation of the Value-Based Payment Modifier (VBM) for groups of 100 or more eligible professionals (EPs), consisting of physicians and CRNAs and others described in detail below.Groups of 100 or more EPs — Watch out for the Value-Based Payment ModifierThe Patient Protection and Affordable Care Act (ACA) requires that Medicare implement a Value-Based Payment Modifier (VBM) that would apply to Medicare fee-for-service payments beginning in 2015. The VBM is intended to pay physicians differentially based on the quality and cost of their care.While CMS must adhere to certain statutory requirements, such as using the modifier to promote shared responsibility and systems-based care, the ACA gives CMS considerable flexibility in terms of implementing the VBM. The 2013 Medicare...  The anesthesia business, regardless of whether one chooses to define it as the practice of medicine, nursing, or some hybrid, is in the midst of upheaval. Increasing market consolidation, mergers, acquisitions and introduction of private equity funding have made the business of managing anesthesia delivery services increasingly complex. Bear in mind that delivering anesthesia and managing the delivery of anesthesia services are two very different things.
Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the...
The anesthesia business, regardless of whether one chooses to define it as the practice of medicine, nursing, or some hybrid, is in the midst of upheaval. Increasing market consolidation, mergers, acquisitions and introduction of private equity funding have made the business of managing anesthesia delivery services increasingly complex. Bear in mind that delivering anesthesia and managing the delivery of anesthesia services are two very different things.
Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the...  All of you are familiar with some of the regulatory requirements that affect your practice, as identified by their acronyms and initials: HIPAA, CMS, CoPs,PQRS, SCIP, ACO, HCAHPS. For hospital-based practices, there are now two additional “ingredients” in our regulatory alphabet soup that will require your attention: OPPE and FPPE.
Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.
The Joint Commission and other accrediting bodies and payers have established more stringent guidelines for the ongoing evaluation of medical staff members. The Ongoing Professional Practice Evaluation (OPPE) and Focused Professional Practice Evaluation (FPPE) are now becoming part of every hospitalbased anesthesia practice’s routine. These evaluations are expected to occur on a regular basis and serve as the key component to the hospital reappointment process.
Key Components
In adopting the Accreditation Council for...
All of you are familiar with some of the regulatory requirements that affect your practice, as identified by their acronyms and initials: HIPAA, CMS, CoPs,PQRS, SCIP, ACO, HCAHPS. For hospital-based practices, there are now two additional “ingredients” in our regulatory alphabet soup that will require your attention: OPPE and FPPE.
Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.
The Joint Commission and other accrediting bodies and payers have established more stringent guidelines for the ongoing evaluation of medical staff members. The Ongoing Professional Practice Evaluation (OPPE) and Focused Professional Practice Evaluation (FPPE) are now becoming part of every hospitalbased anesthesia practice’s routine. These evaluations are expected to occur on a regular basis and serve as the key component to the hospital reappointment process.
Key Components
In adopting the Accreditation Council for...
Participating in Medicare’s
Physician Quality Reporting System (PQRS) has taken on a new flavor this
year. While until now participating has meant a potential annual bonus
of several thousand dollars, not reporting in 2013 will entail
a penalty in 2015. Losing out on a bonus is less galling than
forfeiting a percentage of each remittance. No anesthesiologist, CRNA
or pain physician is doomed to lose money for failing to report the
applicable PQRS measure(s). This Alert will provide a reminder of the
steps you need to take to earn the bonus and to avoid future penalties.
It is a testament to the
undue complexity of the program that we are now in its seventh year, and
yet uncertainty lingers. As a reminder, the incentive payments and
“payment adjustments” for each year are as follows:
YearPayment/AdjustmentMadeReporting YearPayment or (Adjustment)
200820071.5%2009 20081.5%
201020092.0%
201120102.0%
201220111.0%
201320120.5%
201420130.5%
201520140.5%
20152013(1.5%)
2016 onward2014 onward(2.0%)
...
The Centers for Medicare and
Medicaid Services (CMS) has been encouraging the growth of accountable
care organizations (ACOs) and other integrated models under the impetus
of the Affordable Care Act (ACA). The Federal Trade Commission (FTC),
on the other hand, remains fiercely protective of competition. If
competitors coalesce into a single large organization, there will be
fewer competitors.
The ACA provides that
“nothing [in the legislation] shall be construed to modify, impair or
supersede the operation of the antitrust laws.” In October 2011 the FTC
jointly with the Department of Justice issued its Final Statement of Antitrust Enforcement Policy Regarding Accountable Care Organizations—following, but not allaying, much criticism of the corresponding proposed rule.
The tension between the two
drives, integration versus competition, has increased steadily since the
passage of the ACA. A recent and unusual FTC decision to go to court
to block the acquisition of a medical group by a hospital...
 Failure of the Joint Select Committee on Deficit Reduction to reach agreement on $1.2 trillion in cuts to federal spending, has triggered automatic Federal budget cuts known as sequestration. The cuts were originally scheduled to go into effect January 2, 2013. Congress delayed implementation until March and President Obama signed the order late Friday evening, March 1.The 2% cut is evenly split between domestic and defense programs, with half affecting defense discretionary spending (weapons purchases, base operations, construction work, etc.) and the rest affecting both mandatory and discretionary domestic spending. Only a few mandatory programs, like the unemployment trust fund and, most notably, Medicare (more specifically—provider and hospital payments) are affected.Last Friday, the White House Budget Office provided an 83-page list identifying for each of 1,200 accounts what amount needed to be chopped. Medicare beneficiaries will not be subject to any reductions in their benefits. Rather, the expected $123 billion cut...
Failure of the Joint Select Committee on Deficit Reduction to reach agreement on $1.2 trillion in cuts to federal spending, has triggered automatic Federal budget cuts known as sequestration. The cuts were originally scheduled to go into effect January 2, 2013. Congress delayed implementation until March and President Obama signed the order late Friday evening, March 1.The 2% cut is evenly split between domestic and defense programs, with half affecting defense discretionary spending (weapons purchases, base operations, construction work, etc.) and the rest affecting both mandatory and discretionary domestic spending. Only a few mandatory programs, like the unemployment trust fund and, most notably, Medicare (more specifically—provider and hospital payments) are affected.Last Friday, the White House Budget Office provided an 83-page list identifying for each of 1,200 accounts what amount needed to be chopped. Medicare beneficiaries will not be subject to any reductions in their benefits. Rather, the expected $123 billion cut...
Several recent publications
have described strategies for hospitals and ambulatory surgical centers
to improve their operational health—their profitability, to be blunt.
Anesthesiologists are well aware of the role that they can play in O.R.
management and of the need to assume O.R. leadership responsibilities in
order to remain competitive. There are some valuable ideas to be
gleaned from articles and presentations directed to O.R. managers.
Anesthesiologists can take charge of most, if not all, of the processes
described below.
Many ways to improve O.R.
efficiency are already familiar. The value of on-time starts, fast
turnover times and block scheduling, to name but a few such ways, is a
given. Jeffry Peters’s February 28, 2013 webinar hosted by Becker’s
Healthcare and entitled Managing Surgical Services Lines under Accountable Care and Value-Based Purchasing
identified some additional operational changes that would help
hospitals obtain a “sustainable competitive advantage.” Peters is the
president and CEO...
 Over the New Year holiday, Congress finally passed legislation to stop the U.S. economy from going over the fiscal cliff. The new law included a temporary reprieve from the 26.5 percent cut provided for by the Medicare Sustainable Growth Rate (SGR) formula. There will be no SGR reduction throughout 2013—a development that lets us all breathe a deep sigh of relief, even though the formula itself, and its future depredations, are still in the law. Medicare payments to physicians and hospitals are not inviolate for the coming year, it must be noted: automatic two-percent reductions will hit Medicare as part of the “sequestration” process just two months from now if Congress and the White House do not reach another deal.
For many anesthesia practices, the runup to negotiations with hospitals and payers is a cliffhanger—indeed, even contemplating future negotiations often feels precarious. Last year, one of the national anesthesia practice management...
Over the New Year holiday, Congress finally passed legislation to stop the U.S. economy from going over the fiscal cliff. The new law included a temporary reprieve from the 26.5 percent cut provided for by the Medicare Sustainable Growth Rate (SGR) formula. There will be no SGR reduction throughout 2013—a development that lets us all breathe a deep sigh of relief, even though the formula itself, and its future depredations, are still in the law. Medicare payments to physicians and hospitals are not inviolate for the coming year, it must be noted: automatic two-percent reductions will hit Medicare as part of the “sequestration” process just two months from now if Congress and the White House do not reach another deal.
For many anesthesia practices, the runup to negotiations with hospitals and payers is a cliffhanger—indeed, even contemplating future negotiations often feels precarious. Last year, one of the national anesthesia practice management...
In meetings and conferences where the presenter asks anesthesiologists and pain physicians whether they are participating in—or negotiating with—an Accountable Care Organization (ACO), very few, if any, of the doctors raise their hands. Everyone is aware of the concept of ACOs, but almost no one has any experience with them yet. Nevertheless, there are significant ACO developments across the country.Tens of millions of patients are already receiving medical services through ACOs. A year ago—even before the United States Supreme Court’s decision upholding most of the Affordable Care Act—32 ACOs were participating in the Medicare Pioneer demonstration program and 27 more had signed up to become Medicare ACOs. Becker’s Hospital Review briefly described 80 Accountable Care Organizations to Know, both commercial and Medicare, in an online article dated April 16, 2012. Many of these ACOs were formed by hospitals and health systems in partnership with health plans. They range in size from as...
 I am an anesthesiologist. The leadership of my small group of 15 physicians has been negotiating a merger with the large group in a nearby city. They have made some compelling arguments for the strategic advantages of an affiliation with a larger entity. But as logical as the rationale for merging is, so are the concerns and the questions raised by detractors. It is just not clear that all the disruption of closing out our current entity and transitioning to employment status with the big group will result in a more favorable situation for us as individuals or even as a division of the new entity. I personally worry about losing control of my practice and the clinical autonomy that attracted me to this practice in the first place. The fact is that I am still unsure how I will vote when we all get together to make a final...
I am an anesthesiologist. The leadership of my small group of 15 physicians has been negotiating a merger with the large group in a nearby city. They have made some compelling arguments for the strategic advantages of an affiliation with a larger entity. But as logical as the rationale for merging is, so are the concerns and the questions raised by detractors. It is just not clear that all the disruption of closing out our current entity and transitioning to employment status with the big group will result in a more favorable situation for us as individuals or even as a division of the new entity. I personally worry about losing control of my practice and the clinical autonomy that attracted me to this practice in the first place. The fact is that I am still unsure how I will vote when we all get together to make a final... 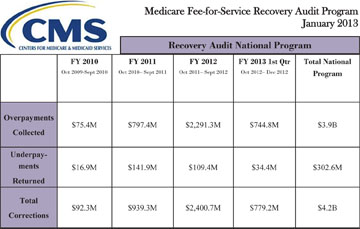 CMS’ Medicare Recovery Audit Contractor (RAC) Program has now been in effect in all 50 states for three years. The RACs, readers will recall, are contractors who are compensated on a contingency fee basis for finding and recouping overpayments made by Medicare to physicians, hospitals and other providers. Each of the four RACs is responsible for identifying overpayments—and underpayments—“in a geographically defined area that is roughly one-quarter of the country. In addition, [they] are responsible for highlighting to CMS common billing errors, trends, and other Medicare payment issues,” according to a report from CMS to Congress released earlier this month and entitled Recovery Auditing in the Medicare and Medicaid Programs.The RACs analyze Medicare FFS claims on a post-payment basis, using three different processes: (1) automated reviews of claims data, (2) semi-automated reviews where the RAC allows the provider to substantiate the claim with supporting documents and (3) complex reviews, where a qualified...
CMS’ Medicare Recovery Audit Contractor (RAC) Program has now been in effect in all 50 states for three years. The RACs, readers will recall, are contractors who are compensated on a contingency fee basis for finding and recouping overpayments made by Medicare to physicians, hospitals and other providers. Each of the four RACs is responsible for identifying overpayments—and underpayments—“in a geographically defined area that is roughly one-quarter of the country. In addition, [they] are responsible for highlighting to CMS common billing errors, trends, and other Medicare payment issues,” according to a report from CMS to Congress released earlier this month and entitled Recovery Auditing in the Medicare and Medicaid Programs.The RACs analyze Medicare FFS claims on a post-payment basis, using three different processes: (1) automated reviews of claims data, (2) semi-automated reviews where the RAC allows the provider to substantiate the claim with supporting documents and (3) complex reviews, where a qualified...  Part I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations.
Part I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations.
"Physicians’ relationships with the pharmaceutical industry should be transparent and focused on benefits to patients." (Jeremy A. Lazarus, MD, President, American Medical Association, Statement on Final Physician Payment Sunshine Act Rule, February 1, 2013.)“You should know when your doctor has a financial relationship with the companies that manufacture or supply the medicines or medical devices you may need. Disclosure of these relationships allows patients to have more informed discussions with their doctors.” (Peter Budetti, MD, JD, CMS Deputy Administrator for Program Integrity, quoted in Rule Increases Transparency in Health Care, press release, February 1, 2013.)Have you ever received a consulting fee, a meal, a textbook, a mug or a pen set from a drug company or a device manufacturer? If the value of the item was more than $10, it would likely be reportable to a new registry under the Physician Payment Sunshine Act and the final regulations (“Final Rule”) published by CMS on February...
 Noah Rosenberg, M.D.Resident, Department of Family & Community Medicine, University of Massachusetts Memorial Medical Center, Worcester, MA
Fred E. Shapiro, D.O.Assistant Professor of Anesthesia, Harvard Medical School, Boston, ISOBS Founder
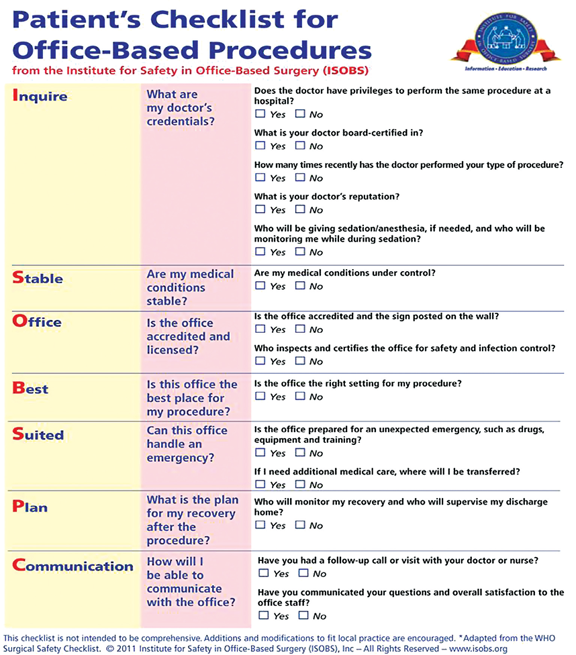
The Institute for Safety in Office-Based Surgery (ISOBS), an independent, non-profit 501(c)(3) organization, has developed a safety checklist for use in the office-based setting. A recent study to be published in the journal ePlastydemonstrated a more than 75% reduction in the number of surgical complications with use of the ISOBS Safety Checklist (see below for citation). While this positive effect on surgical complications validates much of the data already collected in the inpatient setting, it also clearly emphasizes the need for a tailored patient safety approach to the office-based setting. For that reason, ISOBS has developed a second checklist for use by patients to engage them in office-based surgical safety.
The ISOBS Patient Checklist (ISOBS PC) contains a number of questions...
Noah Rosenberg, M.D.Resident, Department of Family & Community Medicine, University of Massachusetts Memorial Medical Center, Worcester, MA
Fred E. Shapiro, D.O.Assistant Professor of Anesthesia, Harvard Medical School, Boston, ISOBS Founder
The Institute for Safety in Office-Based Surgery (ISOBS), an independent, non-profit 501(c)(3) organization, has developed a safety checklist for use in the office-based setting. A recent study to be published in the journal ePlastydemonstrated a more than 75% reduction in the number of surgical complications with use of the ISOBS Safety Checklist (see below for citation). While this positive effect on surgical complications validates much of the data already collected in the inpatient setting, it also clearly emphasizes the need for a tailored patient safety approach to the office-based setting. For that reason, ISOBS has developed a second checklist for use by patients to engage them in office-based surgical safety.
The ISOBS Patient Checklist (ISOBS PC) contains a number of questions... 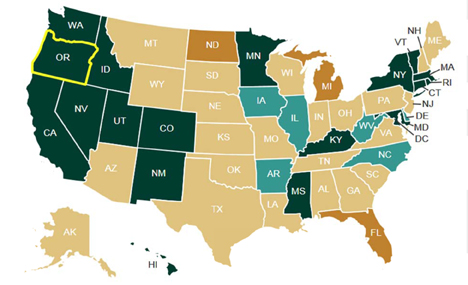 The creation of Health
Insurance Exchanges (HIEs) is among the most important changes to the
health care system made by the Affordable Care Act (ACA). The HIEs are
marketplaces where consumers and small businesses can shop for private
health insurance plans. Many anesthesia and pain medicine patients will
be covered by health plans participating in HIEs beginning as soon as
October 2013. Payment rates under such plans have the potential to make
or break providers. Additionally, some group practices may choose to
offer coverage through the HIEs. A basic familiarity with HIE structure
and operations is therefore in order.
Who
The ACA provides that
effective January 1, 2014, there shall be at least one HIE in each of
the fifty states. States have the option of (1) setting up their own
HIEs, (2) partnering with the federal government to run an exchange, or
(3) opting out—in which case, the Department of...
The creation of Health
Insurance Exchanges (HIEs) is among the most important changes to the
health care system made by the Affordable Care Act (ACA). The HIEs are
marketplaces where consumers and small businesses can shop for private
health insurance plans. Many anesthesia and pain medicine patients will
be covered by health plans participating in HIEs beginning as soon as
October 2013. Payment rates under such plans have the potential to make
or break providers. Additionally, some group practices may choose to
offer coverage through the HIEs. A basic familiarity with HIE structure
and operations is therefore in order.
Who
The ACA provides that
effective January 1, 2014, there shall be at least one HIE in each of
the fifty states. States have the option of (1) setting up their own
HIEs, (2) partnering with the federal government to run an exchange, or
(3) opting out—in which case, the Department of...  The Anesthesia Quality Institute (AQI) is a non-profit corporation created to improve outcomes in anesthesia, based on aggregating, analyzing and reporting electronic data. Over the past three years AQI has recruited more than 220 anesthesia practices, from 44 states, to contribute data to the National Anesthesia Clinical Outcomes Registry (NACOR). The aggregate data has provided a unique and valuable perspective on the specialty of anesthesiology: What we do, what we know, and how we do it. At the same time, a picture is emerging of the other side of our national practice: What we don’t know and what we don’t do.
The widest performance gap in anesthesia today is our collective lack of insight regarding outcomes of the care we provide. Even among the participating groups in NACOR—a self-selected ‘choir’ of early adapters—fewer than 1 in 5 have the infrastructure to recognize and respond to the following event:
Mrs. Smith,...
The Anesthesia Quality Institute (AQI) is a non-profit corporation created to improve outcomes in anesthesia, based on aggregating, analyzing and reporting electronic data. Over the past three years AQI has recruited more than 220 anesthesia practices, from 44 states, to contribute data to the National Anesthesia Clinical Outcomes Registry (NACOR). The aggregate data has provided a unique and valuable perspective on the specialty of anesthesiology: What we do, what we know, and how we do it. At the same time, a picture is emerging of the other side of our national practice: What we don’t know and what we don’t do.
The widest performance gap in anesthesia today is our collective lack of insight regarding outcomes of the care we provide. Even among the participating groups in NACOR—a self-selected ‘choir’ of early adapters—fewer than 1 in 5 have the infrastructure to recognize and respond to the following event:
Mrs. Smith,...
Anesthesia revenue streams are an attractive target for investors of various stripes.
Across the country,
ambulatory surgical centers (ASCs) and certain medical specialty groups
are looking at beefing up their incomes by sharing in anesthesia
profits. At the January 24-26, 2013 ASA Practice Management Conference,
Judith Jurin Semo, Esq., who presented an Update on the Company Model,
noted that trade press articles encouraging such ventures appear
regularly, going back at least to 2004 (Outpatient Surgery). The
“company model” arrangement, which allows a third party to use an
intermediate corporation to collect the professional fees while paying
the anesthesiologists a negotiated rate, has been the object of
considerable concern on the part of the ASA and the anesthesia community
at large. Polled informally, one-third of anesthesiologists report
having been approached about participating in a company model.
The company model is becoming familiar, but is it legal?
The Federal Anti-Kickback Statute
The chief...
 Christopher Ryan, Esq. Giarmarco, Mullins & Horton, P.C., Troy, MI
Neda M. Ryan, Esq. Clark Hill, PLC, Birmingham, MI
Reporting post-operative pain management procedures often gives rise to questions, especially toward the beginning of the new year when the Centers for Medicare and Medicaid Services (CMS) issues its National Correct Coding Initiative (NCCI) edits. Historically, epidurals and blocks that are placed pre-operatively for the purpose of managing post-operative pain have been, and still are, separately reportable and not bundled into the anesthesia service itself. The exception to this general rule is when the epidural or block is the anesthetic itself. While CMS has not called for significant changes in 2013, anesthesia providers should, nevertheless, be aware of new post-operative pain management coding changes taking effect January 1, 2013.
NCCI Edits
The NCCI edits for 2013 provide, in part, that certain post-operative pain management procedures may only be separately reportable with...
Christopher Ryan, Esq. Giarmarco, Mullins & Horton, P.C., Troy, MI
Neda M. Ryan, Esq. Clark Hill, PLC, Birmingham, MI
Reporting post-operative pain management procedures often gives rise to questions, especially toward the beginning of the new year when the Centers for Medicare and Medicaid Services (CMS) issues its National Correct Coding Initiative (NCCI) edits. Historically, epidurals and blocks that are placed pre-operatively for the purpose of managing post-operative pain have been, and still are, separately reportable and not bundled into the anesthesia service itself. The exception to this general rule is when the epidural or block is the anesthetic itself. While CMS has not called for significant changes in 2013, anesthesia providers should, nevertheless, be aware of new post-operative pain management coding changes taking effect January 1, 2013.
NCCI Edits
The NCCI edits for 2013 provide, in part, that certain post-operative pain management procedures may only be separately reportable with...
“Much has changed in health
care since HIPAA was enacted over fifteen years ago,” said HHS Secretary
Kathleen Sebelius in the Department of Health and Human Services’
January 17th press release announcing the publication of the
long-awaited final omnibus rule with Modifications to the HIPAA Privacy,
Security, Enforcement and Breach Notification Rules under the Health
Information Technology for Economic and Clinical Health Act and the
Genetic Information Nondiscrimination Act. “The new rule will help
protect patient privacy and safeguard patients’ health information in an
ever expanding digital age.”
The final omnibus rule will
go into effect on March 26, 2013. Covered entities such as anesthesia
and pain medicine practices and billing companies including ABC—and
their business associates—must be in compliance by September 23, 2013.
The final rule changes HIPAA in several important ways:
It toughens the definition and consequences of failure to notify affected parties of security and privacy breaches;It strengthens...
 The Centers for Medicare and Medicaid Services (CMS) Contractor Medical Directors (CMDs) recently put together a list of common CMS claim issues that were of concern to various contractors. Several of these items involve services that may impact anesthesia or pain management providers.
1. Use of modifier -59 for imaging with those procedures that now INCLUDE imaging in the code description and payment e.g. paravertebral joint/nerve blocks; transforaminal epidurals, many others.
In some cases, the base procedure includes fluoroscopy or CT imaging and the provider decides to perform the service under ultrasound guidance. Since the ultrasound guidance is not “bundled” in the base procedure description, coders are incorrectly appending modifier 59. However, the base procedure includes the payment for the fluoroscopy or CT imaging. It is incorrect to substitute the required and bundled imaging for another type that is not bundled and bill it separately.
2. Billing for “not qualified” personnel...
The Centers for Medicare and Medicaid Services (CMS) Contractor Medical Directors (CMDs) recently put together a list of common CMS claim issues that were of concern to various contractors. Several of these items involve services that may impact anesthesia or pain management providers.
1. Use of modifier -59 for imaging with those procedures that now INCLUDE imaging in the code description and payment e.g. paravertebral joint/nerve blocks; transforaminal epidurals, many others.
In some cases, the base procedure includes fluoroscopy or CT imaging and the provider decides to perform the service under ultrasound guidance. Since the ultrasound guidance is not “bundled” in the base procedure description, coders are incorrectly appending modifier 59. However, the base procedure includes the payment for the fluoroscopy or CT imaging. It is incorrect to substitute the required and bundled imaging for another type that is not bundled and bill it separately.
2. Billing for “not qualified” personnel...