The national average Medicare anesthesia conversion factor (CF) effective January 1, 2016 will be $22.4426, down from $22.6093 in 2015, which is a decrease of $0.1667 per anesthesia unit. Geographically-adjusted CFs for the 90-odd Medicare localities are not yet available. The general Medicare physician fee schedule CF, which is used to calculate payments for visit services and pain medicine and other non-anesthesia procedures, will be $35.8279, a decrease of 10.56 cents per relative value unit (RVU). CMS announced the new CFs in the Final Rule containing Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016, released on October 30.After the elimination of the Sustainable Growth Rate (SGR) formula in last spring’s Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), we had hoped to see the last of the “negative updates” or cuts in Medicare payment rates. MACRA replaced the SGR with...
 Would you consider yourself an investment professional in your spare time? I didn’t think so. But many doctors who run their own practice are unknowingly held to that standard as fiduciaries to their 401(k) plan. If you’re playing that role, in part or whole, you’ve opened yourself up to personal liability if you (or those to whom you’ve delegated the decisions) fail to make the best choices for your plan’s investment line-up.
This situation may sound far-fetched—not unlike asking your receptionist to perform medical procedures between phone calls—but I’ve seen it happen time and time again. Many small medical practices have their own retirement savings plans, typically a 401(k) or the very similar 403(b). You may start your plan with the best intentions: to give yourself and your employees the ability to build tax-deferred retirement savings. But someone has to decide what investments will be offered in the plan. Someone also...
Would you consider yourself an investment professional in your spare time? I didn’t think so. But many doctors who run their own practice are unknowingly held to that standard as fiduciaries to their 401(k) plan. If you’re playing that role, in part or whole, you’ve opened yourself up to personal liability if you (or those to whom you’ve delegated the decisions) fail to make the best choices for your plan’s investment line-up.
This situation may sound far-fetched—not unlike asking your receptionist to perform medical procedures between phone calls—but I’ve seen it happen time and time again. Many small medical practices have their own retirement savings plans, typically a 401(k) or the very similar 403(b). You may start your plan with the best intentions: to give yourself and your employees the ability to build tax-deferred retirement savings. But someone has to decide what investments will be offered in the plan. Someone also...
Early this year, the U.S. Supreme Court ruled that the North Carolina State Board of Dental Examiners (Dental Board) violated the federal antitrust laws by preventing non-dentists from providing teeth whitening services in competition with the state’s licensed dentists in North Carolina State Board of Dental Examiners v. FTC, 135 S. Ct. 1101 (2015). The Dental Board had contended that its activity was immune from antitrust scrutiny under the “state action” doctrine because it was an exercise of the state’s sovereign power. The Court rejected that contention and upheld the Federal Trade Commission’s determination that the Dental Board’s enforcement actions against teeth whitening competitors had illegally restrained trade and did not amount to protected “state action.” To be protected, a state licensing agency such as a board of dentistry or of medicine that is made up of active members of the professions they regulate, such as practicing physicians, must be “actively...
 The Centers for Medicare and Medicaid Services (CMS) Bundled Payments for Care Improvement (BPCI) initiative is comprised of four broadly defined models of care, which link payments for the multiple services beneficiaries receive during an episode of care. Under the initiative, organizations enter into payment arrangements that include financial and performance accountability for episodes of care. The intent is for these models to lead to higher quality and more coordinated care at a lower cost to Medicare.
Traditional Medicare reimburses physicians on a fee-for-service (FFS) system, through Part B, and hospitals under an inpatient prospective payment system (IPPS) through Part A. Both systems are triggered by individual services being provided to beneficiaries for a discrete illness or course of treatment. Various studies have demonstrated that this approach can result in fragmented care with minimal coordination across providers and healthcare settings. As we have heard many times, the payment systems are geared...
The Centers for Medicare and Medicaid Services (CMS) Bundled Payments for Care Improvement (BPCI) initiative is comprised of four broadly defined models of care, which link payments for the multiple services beneficiaries receive during an episode of care. Under the initiative, organizations enter into payment arrangements that include financial and performance accountability for episodes of care. The intent is for these models to lead to higher quality and more coordinated care at a lower cost to Medicare.
Traditional Medicare reimburses physicians on a fee-for-service (FFS) system, through Part B, and hospitals under an inpatient prospective payment system (IPPS) through Part A. Both systems are triggered by individual services being provided to beneficiaries for a discrete illness or course of treatment. Various studies have demonstrated that this approach can result in fragmented care with minimal coordination across providers and healthcare settings. As we have heard many times, the payment systems are geared...
CMS released the long-awaited final rule on the Electronic Health Record Incentive Program-Stage 3 and Modifications to Meaningful Use in 2015 through 2017 (Final Rule) on October 6, 2015. In this rule, CMS made significant changes to current “Meaningful Use” (MU) requirements with the intent to ease the reporting burden for physicians and other providers and to support interoperability.The Electronic Health Record (EHR) Incentive Program was established by the American Recovery and Reinvestment Act of 2009. Separate Medicare and Medicaid programs provide for incentive payments to eligible professionals (EPs) who are meaningful users of certified EHR technology. The last year in which EPs could earn a Medicare incentive payment was 2014; the Medicaid program provides for incentives through 2016. Starting on January 1, 2015, EPs who do not demonstrate MU under either the Medicare EHR Incentive Program or the Medicaid EHR Incentive Program are subject to a payment “adjustment” or penalty—unless...
Anesthesia Business Consultants (ABC), a leading provider in billing and practice management for the anesthesia and pain management specialty, is pleased to announce the release of the fall issue of its quarterly newsletter, The Communiqué.The Communiqué is dedicated to publishing articles and advice, specific to the anesthesia and pain management community that are practical and tangible. The Communiqué is complimentary. It features articles focusing on the latest hot topics for anesthesiologists, nurse anesthetists, pain management specialists, anesthesia practice administrators and especially C-Suite executives in health systems where anesthesia is an important factor.ABC is pleased to provide The Communiqué electronically as well as in hard-copy versions.The fall 2015 issue features articles designed to help readers navigate the changes in the world of anesthesia. The Perioperative Surgical Home: “Right for our Group?” by Rick Bushnell, MD, MBA, a private practice anesthesiologist in Southern California, is a shining example of the response that the...
Telemedicine, in one form or another, is going to be part of most physician practices within the next decade. For many doctors, it will arrive sooner, if it is not already here. Five years ago, Dr. Girish Joshi wrote in the ASA Newsletter (Global Patient Perioperative Care through Clinical Pathways, ASA Newsletter. 2010; 74(8):10-12):Telemedicine is a term used to describe health care provided by a practitioner at a remote location with the help of advanced technologies. Telemedicine is expected to play an increasingly important role in outpatient settings (e.g., home health care, remote patient monitoring, chronic disease management and rural health care) as well as in hospital settings (e.g., emergency department and ICU). Other applications of telemedicine include battlefield medicine, maritime medicine and aviation health care. Telemedicine provided in the critical care setting is commonly referred to as e-ICU. e-ICU has been proposed as a potential means of bringing the expertise...
The third-party medical payment system is so complicated that incorrect payments are not uncommon. Sometimes the error is in the provider’s favor. The health insurer may ask the provider—in this instance, the anesthesia practice—to refund an alleged overpayment. How should the practice handle such requests? The American Medical Association (AMA) has published an excellent Overpayment Recovery Toolkit, which we summarize in this Alert while referring readers to the 14-page Toolkit for more detailed information. When do payers request refunds of overpayments?Managed care contracts typically permit the payer to recover alleged overpayments by reducing or “offsetting” overpaid amounts from pending or future claims payments. The problem does not generally arise with non-contracted payers since they are apt to reimburse the patient instead of the practice. Payers request refunds—or offset overpaid amounts against other payments to the physicians—when any of the following occur:Duplicate paymentsAnother insurer is responsible (coordination of benefits problem)Patient’s coverage has...
 One feature of the Affordable Care Act (ACA) that has received limited attention is the high-cost plan tax (HCPT), aka the “Cadillac plan” tax. Beginning in 2018, employer health benefit plans with a value exceeding certain thresholds will be subject to an excise tax of 40 percent on the incremental costs of those benefits. This tax is likely to affect anesthesia practices in two ways: (1) in many instances, patients with employer-provided insurance may be responsible for a greater share of their health costs and (2) practices that offer relatively rich health benefits may themselves owe the excise tax.
In 2018, the thresholds for the tax are $10,200 for individual coverage and $27,500 for family coverage. They will increase annually based on the general rate of inflation.
The Kaiser Family Foundation (KFF) published a report on August 25, 2015 (How Many Employers Could be Affected by the Cadillac Plan Tax?) in...
One feature of the Affordable Care Act (ACA) that has received limited attention is the high-cost plan tax (HCPT), aka the “Cadillac plan” tax. Beginning in 2018, employer health benefit plans with a value exceeding certain thresholds will be subject to an excise tax of 40 percent on the incremental costs of those benefits. This tax is likely to affect anesthesia practices in two ways: (1) in many instances, patients with employer-provided insurance may be responsible for a greater share of their health costs and (2) practices that offer relatively rich health benefits may themselves owe the excise tax.
In 2018, the thresholds for the tax are $10,200 for individual coverage and $27,500 for family coverage. They will increase annually based on the general rate of inflation.
The Kaiser Family Foundation (KFF) published a report on August 25, 2015 (How Many Employers Could be Affected by the Cadillac Plan Tax?) in...
Thursday, October 1, 2015 is the date on which all providers must start using ICD-10 diagnosis codes on their claims. We cannot overstate the importance of compliance. Claims must contain a valid ICD-10 code in order to be paid.ABC, as part of our commitment to compliance, is stepping up our efforts to help clients make a successful transition by offering an ICD-10 hotline. Beginning October 1st the ABC ICD-10 hotline, staffed by ICD-trained coders, will be available to handle your urgent questions. If you need help selecting the appropriate ICD-10 code, reporting services that span October 1st, figuring out what further information you need and where to find it, or answering any other questions regarding the new codes, we encourage you to call the ICD-10 hotline between the hours of 8:00 a.m. and 6:00 p.m. EST.Clients will be given the number for the ICD-10 hotline by their ABC client services representative...
 Anesthesia billing is complex and riddled with a minefield of potential compliance issues. Thoughtful anesthesia groups have effective compliance programs in place, designed to minimize the risk of government allegations of fraud and abuse. When crafting and maintaining an effective billing compliance program it is helpful to understand which areas of anesthesia billing have been the subject of legal action. Moreover, like it or not, when a compliance officer is able to point to specific instances in which anesthesia providers have been subject to criminal or civil penalties, s/he is more able to obtain the highest level of compliance from otherwise recalcitrant providers. This article will provide information on where to find details on legal cases impacting anesthesia providers and discuss strategies for implementing the lessons that can be learned from a thorough understanding of the cases.
How to Find the Cases
The government understands the value of publicizing the cases...
Anesthesia billing is complex and riddled with a minefield of potential compliance issues. Thoughtful anesthesia groups have effective compliance programs in place, designed to minimize the risk of government allegations of fraud and abuse. When crafting and maintaining an effective billing compliance program it is helpful to understand which areas of anesthesia billing have been the subject of legal action. Moreover, like it or not, when a compliance officer is able to point to specific instances in which anesthesia providers have been subject to criminal or civil penalties, s/he is more able to obtain the highest level of compliance from otherwise recalcitrant providers. This article will provide information on where to find details on legal cases impacting anesthesia providers and discuss strategies for implementing the lessons that can be learned from a thorough understanding of the cases.
How to Find the Cases
The government understands the value of publicizing the cases...
What does it mean when an anesthesiologist signs a patient’s medical record? What happens if the anesthesiologist’s signature is missing?In general, a signature has three basic purposes:Intent. The signature indicates confirmation that the signing party reviewed and approved the content or that s/he authored the document and approved the content.Integrity. The signature protects the integrity of the document against a claim that the entry was invalid or that it had been altered.Identity. The signature identifies the signing party.In the healthcare context, for medical review purposes, Medicare requires that the treating or ordering practitioner authenticate the services in question, with very few exceptions. The method used must be a handwritten or electronic signature. (Program Integrity Manual Chapter 3 Section 3.3.2.4)The point of the practitioner’s signature in patients’ medical records, operative reports, anesthesia records, orders and, test findings is to demonstrate that services reported to Medicare have been accurately and fully documented, reviewed...
 There are a number of factors that impact both the relative and absolute attractiveness of a practice to a potential partner/buyer. First off, it is assumed that all anesthesiologists provide high quality clinical care, but there is much more that needs to be considered when gauging whether or not a practice is attractive. Based on Cross Keys Capital’s extensive transactional experience as the most active investment banking firm representing physicians, and more specifically anesthesiologists, on the sale of their practice, we have identified seven high-level areas of focus that buyers use to evaluate the overall attractiveness of a practice.
Corporate Governance/Leadership. The board of directors needs to be comprised of high-quality, well respected physicians, medical directors and executives who have leadership experience in operating and guiding their group. This is a critical component when dealing with prospective buyers as a lack of leadership and structure could potentially be perceived as being...
There are a number of factors that impact both the relative and absolute attractiveness of a practice to a potential partner/buyer. First off, it is assumed that all anesthesiologists provide high quality clinical care, but there is much more that needs to be considered when gauging whether or not a practice is attractive. Based on Cross Keys Capital’s extensive transactional experience as the most active investment banking firm representing physicians, and more specifically anesthesiologists, on the sale of their practice, we have identified seven high-level areas of focus that buyers use to evaluate the overall attractiveness of a practice.
Corporate Governance/Leadership. The board of directors needs to be comprised of high-quality, well respected physicians, medical directors and executives who have leadership experience in operating and guiding their group. This is a critical component when dealing with prospective buyers as a lack of leadership and structure could potentially be perceived as being...
Have you conducted an enterprise-wide analysis of the risk of a loss of unsecured electronic protected health information (ePHI)? Do you have in place a written policy specific to the removal of hardware and electronic media containing ePHI into and out of your office or OR suite?Negative answers to those two questions were the major factors behind the ePHI breach that led to a $750,000 penalty levied against Cancer Care Group, P.C., a 13-physician radiation oncology practice with facilities throughout Indiana. In August, 2012, the Cancer Care Group notified the Office of Civil Rights (OCR) in the Department of Health and Human Services that a laptop bag had been stolen from an employee’s car in Indianapolis, Indiana a month earlier. According to the report, the laptop bag contained the employee’s computer, which did not contain ePHI, and computer server backup media, which contained the ePHI of approximately 55,000 individuals. The ePHI...
 You cannot manage what you cannot measure. This is today’s business mantra and no aspect of any serious business is exempt, from productivity of operations to quality of customer service. The goal is to use objective metrics to drive down cost and improve quality. Is it any wonder that the tools that are driving the management of business should be applied to medical and service specialties like anesthesia? Much as anesthesiologists and CRNAs may resist efforts to quantify their productivity and objectively assess the quality of care provided, this is becoming the new reality in medicine. To resist is to demonstrate one’s inflexibility and to invite alternative solutions. The largest and most aggressive players in the specialty are investing millions in the tools and technology of productivity and quality measurement. Whether this is ultimately good for the specialty is another question for another day.
From OR Utilization to Provider Productivity
The...
You cannot manage what you cannot measure. This is today’s business mantra and no aspect of any serious business is exempt, from productivity of operations to quality of customer service. The goal is to use objective metrics to drive down cost and improve quality. Is it any wonder that the tools that are driving the management of business should be applied to medical and service specialties like anesthesia? Much as anesthesiologists and CRNAs may resist efforts to quantify their productivity and objectively assess the quality of care provided, this is becoming the new reality in medicine. To resist is to demonstrate one’s inflexibility and to invite alternative solutions. The largest and most aggressive players in the specialty are investing millions in the tools and technology of productivity and quality measurement. Whether this is ultimately good for the specialty is another question for another day.
From OR Utilization to Provider Productivity
The...  In last week’s Alert, we looked at Medicare’s Value-Based Modifier (VM) and the Quality and Resource Use Reports (QRURs) that will explain how the VM will affect individual payments. This week we will take a closer look at where Medicare’s move from volume to value will be heading after the VM system sunsets at the end of 2018, as laid out in the payment reform legislation (H.R. 2) that did away with the Sustainable Growth Rate (SGR) methodology in April of this year:
Starting in 2019, the amounts paid to eligible professionals (EPs) will be subject to adjustment for “value” through either the MIPs or an APM, depending on which option the individual EP selects.
The MIPS will replace three cumbersome, costly and almost-unintelligible programs, i.e., the VM, the Physician Quality Reporting System (PQRS) and the Meaningful Use [of Electronic Health Records] incentive program. In concept, at least, it represents a...
In last week’s Alert, we looked at Medicare’s Value-Based Modifier (VM) and the Quality and Resource Use Reports (QRURs) that will explain how the VM will affect individual payments. This week we will take a closer look at where Medicare’s move from volume to value will be heading after the VM system sunsets at the end of 2018, as laid out in the payment reform legislation (H.R. 2) that did away with the Sustainable Growth Rate (SGR) methodology in April of this year:
Starting in 2019, the amounts paid to eligible professionals (EPs) will be subject to adjustment for “value” through either the MIPs or an APM, depending on which option the individual EP selects.
The MIPS will replace three cumbersome, costly and almost-unintelligible programs, i.e., the VM, the Physician Quality Reporting System (PQRS) and the Meaningful Use [of Electronic Health Records] incentive program. In concept, at least, it represents a...  “No man is an island, entire of itself; every man is a piece of the continent, a part of the main” begins John Donne’s famous poem. Anesthesiologists have come to realize that not only are they “a piece of the continent” that is their group, but that they are interdependent on their hospital or health system. The anesthesiologist’s and the group’s well-being is bound up with that of their institution, and perhaps with the health and welfare of other entities as well.
The hospital “continent” is under enormous pressure to improve quality and to hold down costs, and so, therefore, is the “country” that is the anesthesia department. If the incumbent anesthesia groups are not properly managing their costs and quality, the chances are that their hospitals are looking for alternatives. ABC Vice President Jody Locke’s latest article for the Communiqué, Why Utilization and Productivity Metrics Matter, walks readers through the...
“No man is an island, entire of itself; every man is a piece of the continent, a part of the main” begins John Donne’s famous poem. Anesthesiologists have come to realize that not only are they “a piece of the continent” that is their group, but that they are interdependent on their hospital or health system. The anesthesiologist’s and the group’s well-being is bound up with that of their institution, and perhaps with the health and welfare of other entities as well.
The hospital “continent” is under enormous pressure to improve quality and to hold down costs, and so, therefore, is the “country” that is the anesthesia department. If the incumbent anesthesia groups are not properly managing their costs and quality, the chances are that their hospitals are looking for alternatives. ABC Vice President Jody Locke’s latest article for the Communiqué, Why Utilization and Productivity Metrics Matter, walks readers through the... 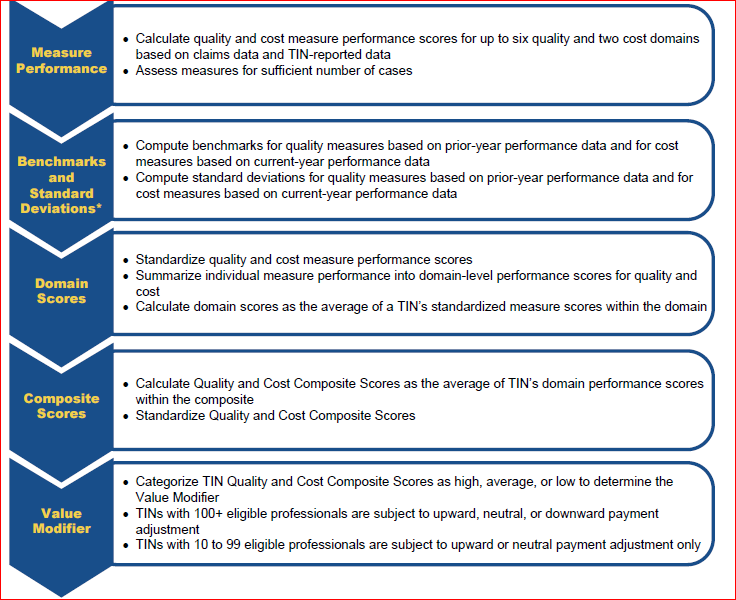 Next year, all physicians in groups of ten or more eligible professionals (EPs) will be subject to the Medicare Value-Based Payment Modifier (VM). Larger groups with 100 or more EPs are already seeing VM adjustments based on their 2013 performance.
In 2017, the VM will apply to all physicians, whether they are in solo practice or are in a group with two or more EPs. And in 2018, payments to nurse anesthetists and anesthesiologist assistants will also reflect the impact of the VM.
It is time for us to familiarize ourselves with the Physician Feedback Program and the Quality and Resource Use Reports (QRURs) that will let physicians find out how they are doing, in terms of the quality and cost metrics that will determine the VM payment adjustment, and compare themselves to their peers.
VM Recap
As we stated in our November 3, 2014 Alert (What Anesthesiologists Need to Know...
Next year, all physicians in groups of ten or more eligible professionals (EPs) will be subject to the Medicare Value-Based Payment Modifier (VM). Larger groups with 100 or more EPs are already seeing VM adjustments based on their 2013 performance.
In 2017, the VM will apply to all physicians, whether they are in solo practice or are in a group with two or more EPs. And in 2018, payments to nurse anesthetists and anesthesiologist assistants will also reflect the impact of the VM.
It is time for us to familiarize ourselves with the Physician Feedback Program and the Quality and Resource Use Reports (QRURs) that will let physicians find out how they are doing, in terms of the quality and cost metrics that will determine the VM payment adjustment, and compare themselves to their peers.
VM Recap
As we stated in our November 3, 2014 Alert (What Anesthesiologists Need to Know...  It’s come to the point that a good part of my work with anesthesia groups involves surgery: removing an earworm—a catchy tune that continually runs through the group’s mind.
In fact, it’s always the same tune, part of The Clash’s Should I Stay or Should I Go Now:
Should I stay or should I go now? Should I stay or should I go now? If I go, there will be trouble, and if I stay it will be double. So come on and let me know. This indecision’s bugging me.
Stay, as in should our group remain independent?
Go, as in should we sell out to someone, maybe anyone, who’ll buy us?
But as is generally the case in life, the decision is not purely either/or, black or white, yes or no. There are many alternatives. And that’s what we “operate on” as part of what I call the Future FinderTM...
It’s come to the point that a good part of my work with anesthesia groups involves surgery: removing an earworm—a catchy tune that continually runs through the group’s mind.
In fact, it’s always the same tune, part of The Clash’s Should I Stay or Should I Go Now:
Should I stay or should I go now? Should I stay or should I go now? If I go, there will be trouble, and if I stay it will be double. So come on and let me know. This indecision’s bugging me.
Stay, as in should our group remain independent?
Go, as in should we sell out to someone, maybe anyone, who’ll buy us?
But as is generally the case in life, the decision is not purely either/or, black or white, yes or no. There are many alternatives. And that’s what we “operate on” as part of what I call the Future FinderTM...
Most of the hospitals located in any of 75 Metropolitan Statistical Areas (MSAs) would be required to participate in a new program that bundles the payment for joint replacement surgeries under a proposal issued by CMS on July 9, 2015. As necessary members of the team that performs joint replacement surgeries, anesthesiologists in those MSAs should consider approaching their hospitals early in order to be sure of a seat at the table. And they should be prepared to share both the opportunity and the risks.The proposed rule for the Comprehensive Care for Joint Replacement (CCJR) is a significant departure from the voluntary Bundled Payment for Care Improvement (BPCI) program in that it requires virtually all affected hospitals to be financially responsible for all of the care of these patients for 90 days after discharge. (Hospitals already participating in the BPCI program will be excluded.)Physicians are not subject to the mandate but...