SUMMARY The misuse and abuse of prescription opioids has become a serious public health problem in the United States and is a major factor in the recent increase in heroin addiction. Practices can help to curtail this problem by staying abreast of new developments and guidelines stressing the prudent use of narcotics.
The death in April of the musician Prince from an accidental overdose of fentanyl is only one of the more highly publicized instances of a public health problem in the United States that has reached epidemic scale. According to the Department of Health and Human Services (HHS), 44 people die every day in the U.S. from an overdose of prescription painkillers.
A recent analysis of more than 800,000 prescriptions written in 2013 showed that pain specialists and anesthesiologists wrote the most opioid prescriptions of any group of healthcare professionals—an average per physician of 900 - 1,100 and 500 prescriptions,...
SUMMARY The U.S. Department of Veterans Affairs (VA) has issued a proposed rule to allow advanced practice registered nurses to practice within their full authority at veterans’ hospitals across the country, preempting certain State laws prohibiting the practice. Although certified registered nurse anesthetists (CRNAs) have not yet been given the green light to furnish anesthetics, the VA continues to consider this issue.
Introduction
Few are unfamiliar with the general state of veterans and healthcare in our country. According to statistics recently released by the VA, an average of 20 veterans died from suicide in 2014. 1 Further, there is a backlog of nearly 500,000 veterans waiting 30 days or longer to receive care at VA facilities across the U.S. This is higher than the numbers from one year ago when reports were released that showed veterans dying while waiting for care as a result of the backlog. 2 In an...
Introduction
To hospitals, the Centers for Medicaid & Medicare Services (CMS) is acting like the terrible Wicked Witch of the West from the movie the Wizard of Oz because of their proposed plans for site-neutral rate reductions. The proposed modifications in reimbursement are included in the 2017 Hospital Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System (CMS-1656-P) proposal submitted on July 6, 2016. The law provides for payment system policy changes, quality reporting provisions, and reduced pay rates that many hospitals would prefer to douse with water and have them disappear like the Wicked Witch rather than have payments reduced at their off-campus facilities.
CMS is proposing a number of policies they believe will improve the quality of care Medicare patients receive. A key piece of the 2017 proposed legislation is the implementation of Section 603 of the Bipartisan Budget Act of 2015, which will affect how...
Prior to addressing the main topic of today’s alert, we felt it necessary to inform our readership of the recent proposed changes made by the Centers for Medicare and Medicaid Services (CMS) in its CY 2017 Proposed Physician Fee Schedule (PPFS). In the CY 2016 PPFS, CMS proposed reexamining the anesthesia codes reported in conjunction with colonoscopy procedures (i.e., 00740 and 00810) as potentially misvalued. In the CY 2017 PPFS, CMS continues to maintain that 00740 and 00810 are misvalued and it “look[s] forward to receiving input from interested parties and specialty societies for consideration during future notice and comment rulemaking.” Moreover, CMS notes that although sedation services are included in certain endoscopic procedures, that anesthesia is being separately reported. As such, “[i]n the CY 2017 PFS proposed rule, CMS is proposing values for the new CPT moderate sedation codes and proposing a uniform methodology for valuation of the procedural codes...
The transition to the International Classification of Diseases and Related Health Problems 10th revision (ICD-10) appears to have gone well so far, despite widespread anxiety that it would wreak havoc across healthcare as providers struggled to comply with the new coding structure, heightened specificity and documentation requirements. The Centers for Medicare and Medicaid Services (CMS) reports that total claims denials and other claims metrics remained essentially unchanged from the historical baseline to the fourth quarter of calendar year 2015.
In a blog post, Andy Slavitt, CMS acting administrator, likened the healthcare industry’s anticipatory concerns surrounding ICD-10 to the Y2K information technology disaster that never took place. “With preparation, planning, a focus on the customer, collaboration, clear accountability, and metrics, the dire Y2K fears didn’t come to pass. Instead, ICD-10 became like what actually occurred on Y2K, an implementation and transition most people never heard about,” he said.
So far, so good.
Nonetheless,...
All physicians, group practices and other providers who participate in Medicare are required to resubmit and recertify the accuracy of their enrollment information every five years through a revalidation process.
Section 6401 (a) of the Affordable Care Act established new screening requirements for providers; required them to be revalidated under those new requirements, and reinforced the revalidation regulations at 42 CFR §424.515. The first cycle of enrollment revalidations ended as the second cycle began in March 2016.
Required Actions
Physicians and other clinicians must submit their revalidation applications by the last day of the month in which they are due. Your Medicare Administrative Contractor (MAC) is expected to notify you of the due date within two to three months of your revalidation deadline, by email or by regular mail. Generally, this due date will remain with you throughout subsequent revalidation cycles.
Centers for Medicare & Medicaid Services (CMS) also maintains a list...
The ASA adopted its Statement on Principles for Alarm Management for Anesthesia Professionals at its annual meeting in October 2013. The introduction to the Statement provides as follows:
As Anesthesia Professionals, we interact with many different types of monitors, machines, infusion pumps and other equipment; many of these devices have audible and/or visual alarms. We rely on alarms to signal us when set parameters/ thresholds are violated and/or when a potentially abnormal situation has occurred. A given alarm’s clinical usefulness depends on numerous factors including attributes of the patient (e.g., baseline clinical status and vital signs), the clinical situation at the time (e.g., anesthetic and procedural factors), the intended recipient(s) (e.g., experience, hearing acuity), unintended recipients (who may be distracted or worried), and the physical environment (e.g., noise and light levels). Management of these alarms becomes challenging, especially in that we must rapidly discern when a trigger is trivial, meaningful or...
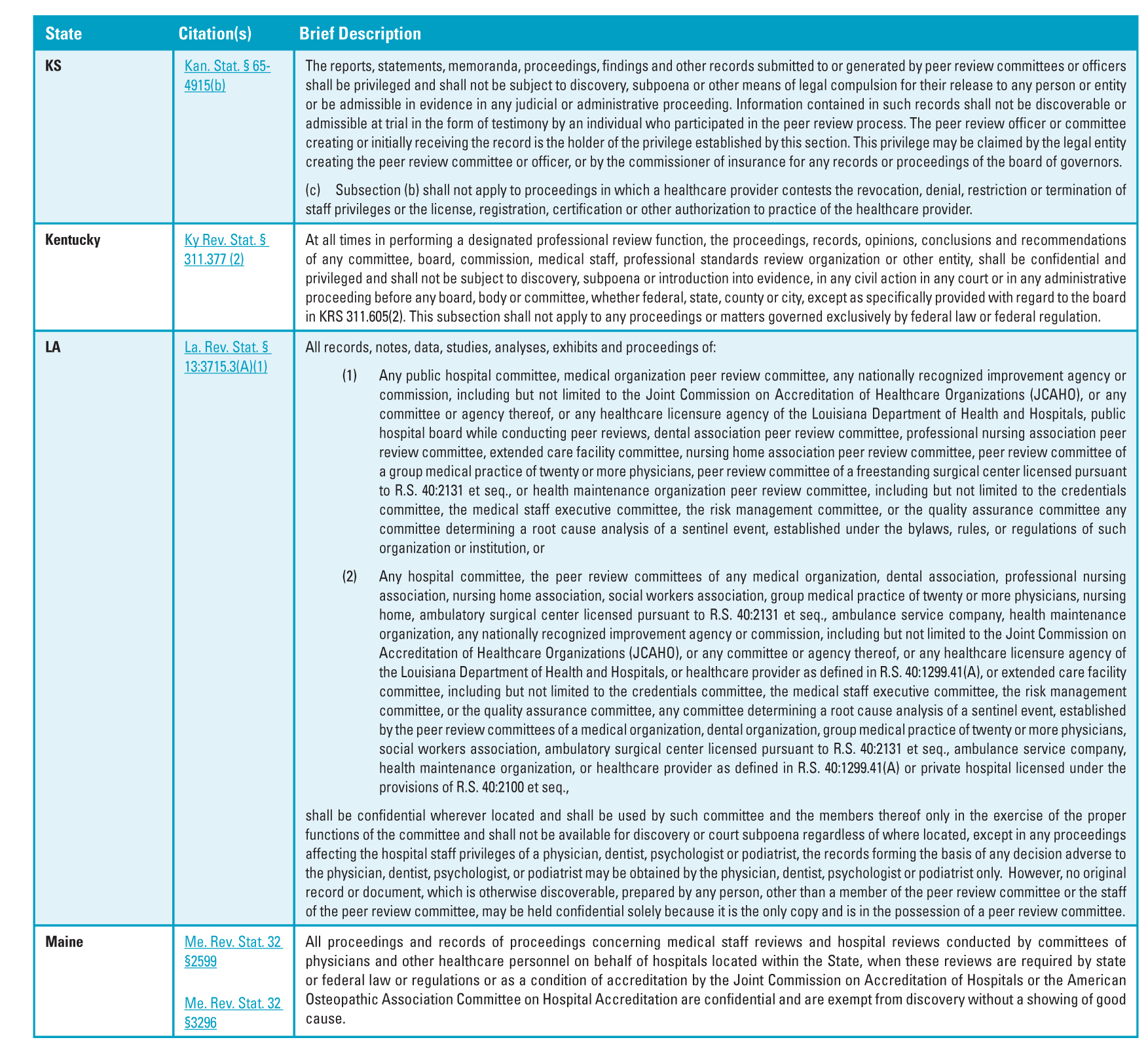 In the Winter 2016 issue of The Communique, we offered Part I of a summary of state laws (Alabama through Iowa) involving the peer review process. Here we are continuing that summary with the remaining states (Kansas through Wyoming).1
In the Winter 2016 issue of The Communique, we offered Part I of a summary of state laws (Alabama through Iowa) involving the peer review process. Here we are continuing that summary with the remaining states (Kansas through Wyoming).1
Have you ever found that you could not make heads or tails of a Medicare regulation? Have you wondered whether even CMS could decipher and coherently apply its own rules? The sheer volume of regulations makes it difficult to be certain of one’s interpretation:
Medicare is, to say the least, a complicated program. The Centers for Medicare & Medicaid Services (CMS) estimates that it issues literally thousands of new or revised guidance documents (not pages) every single year, guidance providers must follow exactingly if they wish to provide health care services to the elderly and disabled under Medicare’s umbrella. Currently, about 37,000 separate guidance documents can be found on CMS’s website.
Caring Hearts Personal Home Services, Inc. v. Burwell (No. 14-3234) (10th Cir. 2016). Caring Hearts, a home health agency, had been ordered to refund more than $800,000 to CMS on the grounds that some of the physical therapy or skilled nursing services...
 One of Robert Frost’s most popular poems is The Road Not Taken. It is about two paths that diverge in the woods. It is a wonderful and powerful metaphor for the decisions we make in life. By selecting one option we inevitably forgo another. More often than not this results in endless speculation as to whether it was the right choice. And so it is with the strategic decision to sell one’s anesthesia practice. The allure of being part of a bigger, stronger and better-managed entity is a powerful draw but does it really result in a more secure practice situation? That is the question of the day.
Anesthesia providers are a curious breed. They are credited with having the shortest decision cycle in medicine. They routinely make critical life and death decisions in a matter of seconds. Ironically, despite their facility in the operating room, when presented with major strategic...
One of Robert Frost’s most popular poems is The Road Not Taken. It is about two paths that diverge in the woods. It is a wonderful and powerful metaphor for the decisions we make in life. By selecting one option we inevitably forgo another. More often than not this results in endless speculation as to whether it was the right choice. And so it is with the strategic decision to sell one’s anesthesia practice. The allure of being part of a bigger, stronger and better-managed entity is a powerful draw but does it really result in a more secure practice situation? That is the question of the day.
Anesthesia providers are a curious breed. They are credited with having the shortest decision cycle in medicine. They routinely make critical life and death decisions in a matter of seconds. Ironically, despite their facility in the operating room, when presented with major strategic...
Most anesthesiologists know in general fashion that there are "compliance" issues with professional courtesy, co-payment waivers and discounts for cash payments. Yet confusion persists about exactly how to handle these situations.
The legal principles have not changed in the nearly two decades since the HHS Office of the Inspector General (OIG) issued its Compliance Program for Individual and Small Group Physician Practices. The basic standards are still as spelled out by the OIG:
In general, whether a professional courtesy arrangement runs afoul of the fraud and abuse laws is determined by two factors: (i) How the recipients of the professional courtesy are selected; and (ii) how the professional courtesy is extended. If recipients are selected in a manner that directly or indirectly takes into account their ability to affect past or future referrals, the anti-kickback statute—which prohibits giving anything of value to generate Federal health care program business—may be implicated. If...
 Given the heightened level of interest in acquisitions of independent anesthesiology groups, physician shareholders are being confronted with a myriad of questions. Many are finding that anesthesiology groups in the local region are being acquired by larger medical groups. What should their practice do? What would be the value of their practice if they sought to be acquired? What does the acquisition process look like and how could maintaining a steady course of non-action not result in the best long term outcome?
Your Practice has Equity Value
Over the years, long-standing relationships have been developed with other healthcare providers and service contracts have been established with medical facilities, securing work for all the practice-employed physicians. A practice will accumulate a substantial amount of sweat equity, which has an equally substantial amount of economic value associated with it. Opportunity currently exists to monetize the value of this equity, and depending on regional...
Given the heightened level of interest in acquisitions of independent anesthesiology groups, physician shareholders are being confronted with a myriad of questions. Many are finding that anesthesiology groups in the local region are being acquired by larger medical groups. What should their practice do? What would be the value of their practice if they sought to be acquired? What does the acquisition process look like and how could maintaining a steady course of non-action not result in the best long term outcome?
Your Practice has Equity Value
Over the years, long-standing relationships have been developed with other healthcare providers and service contracts have been established with medical facilities, securing work for all the practice-employed physicians. A practice will accumulate a substantial amount of sweat equity, which has an equally substantial amount of economic value associated with it. Opportunity currently exists to monetize the value of this equity, and depending on regional...
For patients who undergo a surgical procedure, the anesthesiologist’s bill sometimes comes as a surprise. If the hospital and the surgeon are participating in the patient’s health plan but the anesthesiologist is not in the network and bills the difference between his or her full charge and what the health plan paid, the amount that the patient owes can be a nasty shock. Large balance bills are often stressful for patients and are a major source of medical debt.
Balance billing is a significant issue across the U.S. As insurance companies have narrowed provider networks to keep premiums down, the number of patients who inadvertently receive out-of-network care has jumped at hospitals, particularly with regard to contracted physicians such as anesthesiologists.
In March 2015, the Consumer Reports National Research Center conducted a survey of 2,200 adults that revealed that nearly one third of privately insured Americans received a surprise medical bill...
 Computers and improvements in modern anesthesia delivery have gone hand-in-hand. In 1952 Himmelstein and Scheiner reported that they began using an instrument called the cardiotachoscope and found it useful during surgery. In 1958 Ben Ettelson and James Reeves started Spacelabs to develop systems for the United States Air Force for monitoring vital signs of U.S. astronauts.1 This technology returned to earth, with the 1970s witnessing the expansion of digital electronics in operating rooms (ORs) and critical care units (CCUs). The 1980s saw clinical penetration of modularity and utilization of saturation and end-tidal carbon dioxide monitoring. As pharmaceuticals developed shorter and shorter clinical half-lives and microprocessor technology continued to improve, the concepts of closed-loop (CL) anesthesia, targeted-controlled infusion (TCI) devices and other computer controlled delivery systems moved from theoretical possibilities to clinically relevant systems.2
In the late 1990s Dr. Randy Hinkle, an anesthesiologist, formulated the initial concept that ultimately became Computer- Assisted...
Computers and improvements in modern anesthesia delivery have gone hand-in-hand. In 1952 Himmelstein and Scheiner reported that they began using an instrument called the cardiotachoscope and found it useful during surgery. In 1958 Ben Ettelson and James Reeves started Spacelabs to develop systems for the United States Air Force for monitoring vital signs of U.S. astronauts.1 This technology returned to earth, with the 1970s witnessing the expansion of digital electronics in operating rooms (ORs) and critical care units (CCUs). The 1980s saw clinical penetration of modularity and utilization of saturation and end-tidal carbon dioxide monitoring. As pharmaceuticals developed shorter and shorter clinical half-lives and microprocessor technology continued to improve, the concepts of closed-loop (CL) anesthesia, targeted-controlled infusion (TCI) devices and other computer controlled delivery systems moved from theoretical possibilities to clinically relevant systems.2
In the late 1990s Dr. Randy Hinkle, an anesthesiologist, formulated the initial concept that ultimately became Computer- Assisted...  “Transparency” is a word that you will encounter more and more frequently in health policy articles, including ABC’s publications. Information transparency is a key for enabling healthcare purchasers to make value-based decisions concerning the quality and price of services. Those data are slowly becoming more available, but they remain largely inaccessible to most potential users.
CMS recently released the third year of information from the Medicare Provider Utilization and Payment Data: Physician and Other Supplier database. The database is comprehensive and offers the following information for every physician or Part B supplier who submitted claims in 2014: name, address, gender, specialty, procedure (by HCPCS/CPT™ code), place of service, number of services, number of Medicare beneficiaries, average payment amount, average allowed charge and average submitted charge. What is missing is any information on patients or on outcomes. This being a Medicare database, it excludes the two-thirds of patients who are not in...
“Transparency” is a word that you will encounter more and more frequently in health policy articles, including ABC’s publications. Information transparency is a key for enabling healthcare purchasers to make value-based decisions concerning the quality and price of services. Those data are slowly becoming more available, but they remain largely inaccessible to most potential users.
CMS recently released the third year of information from the Medicare Provider Utilization and Payment Data: Physician and Other Supplier database. The database is comprehensive and offers the following information for every physician or Part B supplier who submitted claims in 2014: name, address, gender, specialty, procedure (by HCPCS/CPT™ code), place of service, number of services, number of Medicare beneficiaries, average payment amount, average allowed charge and average submitted charge. What is missing is any information on patients or on outcomes. This being a Medicare database, it excludes the two-thirds of patients who are not in...  Effective anesthesiology group governance is no longer a luxury but instead an important survival skill. Why?
The external environment is threatening— changes in reimbursement, threats from competitors, hospital consolidation—all add up to the need to make decisions, change and adapt.
The internal dynamics of many groups are challenging—getting “the entire herd roughly moving west,” dealing with disruptive physicians, developing an agreed upon group strategy—all require a well organized governance system.
Whether your group’s Board includes all the shareholder physicians, or you have chosen a subset of the shareholders to serve as the Board, there are a number of steps that you can take to strengthen your Board’s performance. Here are several of the most important steps that an anesthesiology group Board can take.
Improve Board Meetings
We begin with Board meetings. Why Board meetings?
No matter your group’s size, meetings are a tool that all groups use in their governance processes....
Effective anesthesiology group governance is no longer a luxury but instead an important survival skill. Why?
The external environment is threatening— changes in reimbursement, threats from competitors, hospital consolidation—all add up to the need to make decisions, change and adapt.
The internal dynamics of many groups are challenging—getting “the entire herd roughly moving west,” dealing with disruptive physicians, developing an agreed upon group strategy—all require a well organized governance system.
Whether your group’s Board includes all the shareholder physicians, or you have chosen a subset of the shareholders to serve as the Board, there are a number of steps that you can take to strengthen your Board’s performance. Here are several of the most important steps that an anesthesiology group Board can take.
Improve Board Meetings
We begin with Board meetings. Why Board meetings?
No matter your group’s size, meetings are a tool that all groups use in their governance processes....  “Patient Safety Issues Spur NIH Shake-Up” was an above-the-fold headline in the Washington Post on May 11, 2016. NIH Director Francis Collins, MD is replacing top leadership at the 200-bed Clinical Center with a new management team with experience in oversight, compliance and patient safety in the wake of an independent review that found that safety had become “subservient to research demands.”
Also in the news recently was a study published in The BMJ (BMJ 2016; 353 doi: http://dx.doi.org/10.1136/bmj.i2139 [Published 03 May 2016]) by researchers at Johns Hopkins urging the Centers for Disease Control (CDC) to list medical error, broadly defined, as the third most common cause of death in the U.S. after heart disease (611,105 deaths per year) and cancer (584,881 deaths per year). According to the study, the annual number of U.S. deaths attributable to medical error is approximately 251,454—more than three times higher than the 98,000 preventable deaths cited...
“Patient Safety Issues Spur NIH Shake-Up” was an above-the-fold headline in the Washington Post on May 11, 2016. NIH Director Francis Collins, MD is replacing top leadership at the 200-bed Clinical Center with a new management team with experience in oversight, compliance and patient safety in the wake of an independent review that found that safety had become “subservient to research demands.”
Also in the news recently was a study published in The BMJ (BMJ 2016; 353 doi: http://dx.doi.org/10.1136/bmj.i2139 [Published 03 May 2016]) by researchers at Johns Hopkins urging the Centers for Disease Control (CDC) to list medical error, broadly defined, as the third most common cause of death in the U.S. after heart disease (611,105 deaths per year) and cancer (584,881 deaths per year). According to the study, the annual number of U.S. deaths attributable to medical error is approximately 251,454—more than three times higher than the 98,000 preventable deaths cited...  Deciding on new models for an anesthesiology practice is one of our very biggest challenges. It is not realistic for anesthesiologists to continue believing that if they consistently provide good quality care, all of their financial and business issues will take care of themselves. “The beliefs and strategies that have gotten us to where we are today will not get us to where we want to be tomorrow,” as ABC Vice President Jody Locke writes in his article The Road Not Taken in this issue of The Communiqué.
The transition to value-based payment, combined with the strong trend toward larger anesthesia groups and tight affiliations with national anesthesia companies and/or with health systems, has changed the landscape for traditional independent practices. Bill Britton sums up the current environment in Critical Issues to Consider When Exploring the Sale of Your Practice: hospitals are facing mounting pressures to minimize operating costs, including the...
Deciding on new models for an anesthesiology practice is one of our very biggest challenges. It is not realistic for anesthesiologists to continue believing that if they consistently provide good quality care, all of their financial and business issues will take care of themselves. “The beliefs and strategies that have gotten us to where we are today will not get us to where we want to be tomorrow,” as ABC Vice President Jody Locke writes in his article The Road Not Taken in this issue of The Communiqué.
The transition to value-based payment, combined with the strong trend toward larger anesthesia groups and tight affiliations with national anesthesia companies and/or with health systems, has changed the landscape for traditional independent practices. Bill Britton sums up the current environment in Critical Issues to Consider When Exploring the Sale of Your Practice: hospitals are facing mounting pressures to minimize operating costs, including the...  Last week’s e-Alert introduced our readers to the proposed regulations implementing the MACRA Quality Payment Program (Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models). We focused in Part I on the MIPS pathway, which consolidates Medicare’s current quality, cost and EHR reporting programs and promised an overview of the second major physician payment pathway set forth in the proposed rule, the APM Incentive program.
All eligible clinicians will be participating in either the MIPS or the APM program in the near future, as the Physician Quality Reporting System (PQRS), the Value-Based Modifier (VBM) program and the EHR Incentive-Meaningful Use (MU) program phase out, by the end of 2018. Beginning on January 1, 2019, payments will reflect participation in MIPS or APM, based on each clinician’s performance in 2017. The APM incentives are as follows:
For... In the Winter 2016 issue of The Communique, we offered Part I of a summary of state laws (Alabama through Iowa) involving the peer review process. Here we are continuing that summary with the remaining states (Kansas through Wyoming).1
1Special thanks is given to Amy Bell for her assistance in preparing this article.
Last week’s e-Alert introduced our readers to the proposed regulations implementing the MACRA Quality Payment Program (Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models). We focused in Part I on the MIPS pathway, which consolidates Medicare’s current quality, cost and EHR reporting programs and promised an overview of the second major physician payment pathway set forth in the proposed rule, the APM Incentive program.
All eligible clinicians will be participating in either the MIPS or the APM program in the near future, as the Physician Quality Reporting System (PQRS), the Value-Based Modifier (VBM) program and the EHR Incentive-Meaningful Use (MU) program phase out, by the end of 2018. Beginning on January 1, 2019, payments will reflect participation in MIPS or APM, based on each clinician’s performance in 2017. The APM incentives are as follows:
For... In the Winter 2016 issue of The Communique, we offered Part I of a summary of state laws (Alabama through Iowa) involving the peer review process. Here we are continuing that summary with the remaining states (Kansas through Wyoming).1
1Special thanks is given to Amy Bell for her assistance in preparing this article.