 Several clients have inquired as to the documentation and correct coding and billing for Transesophageal Echocardiography (TEE) services. A TEE is a special diagnostic tool, which may be used by properly trained physicians (i.e., anesthesiologists, cardiologists) to benefit patient care. A separately reported TEE may be performed for monitoring and/or diagnostic purposes. However, many payers will only reimburse diagnostic studies.
For example, to establish conditions such as myocardial ischemia or cardiac valve disorders, the anesthesiologist will be utilizing the transesophageal echo for diagnostic purposes. In this case, when the anesthesiologist has the additional certification or documented training in residency, and is privileged by the hospital to do the complete procedure, the anesthesiologist can and should bill separately for the TEE in addition to the anesthesia. The correct CPT code for the complete procedure is 93312. When you bill for both the anesthesia and the TEE, the coder must append...
Several clients have inquired as to the documentation and correct coding and billing for Transesophageal Echocardiography (TEE) services. A TEE is a special diagnostic tool, which may be used by properly trained physicians (i.e., anesthesiologists, cardiologists) to benefit patient care. A separately reported TEE may be performed for monitoring and/or diagnostic purposes. However, many payers will only reimburse diagnostic studies.
For example, to establish conditions such as myocardial ischemia or cardiac valve disorders, the anesthesiologist will be utilizing the transesophageal echo for diagnostic purposes. In this case, when the anesthesiologist has the additional certification or documented training in residency, and is privileged by the hospital to do the complete procedure, the anesthesiologist can and should bill separately for the TEE in addition to the anesthesia. The correct CPT code for the complete procedure is 93312. When you bill for both the anesthesia and the TEE, the coder must append...
We are in the middle of the
ASA Annual Meeting, which draws thousands of anesthesiologists from
across the country to spend several days at meetings and lectures, all
without compensation. We know the incentive for the rank-and-file: the
opportunity to attend an incomparable array of refresher courses, panel
discussions and other continuing education offerings. Hundreds of
anesthesiologists come to educate others and participate in committee
and board activities as specialty leaders.
The sight of so many
physicians spending valuable time together away from the operating room,
along with some questions heard lately, made us wonder how anesthesia
groups secure attendance at their own internal meetings. Board and
other governance meetings, finance and employment committee meetings,
and all-employee and departmental meetings are important—indeed, they
are indispensable to effective group management. While recognizing the
need to conduct business by meeting, few individuals wish they could
attend even more meetings, and many people will...
 The focus on quality outcomes in healthcare has been long in coming. As the cost of health care continues to rise faster than the cost of living, the nation finds itself facing a dilemma. Perhaps a free market approach to healthcare is not the best approach after all. Economic incentives and ground breaking research have clearly provided significant advances in some areas, but what has been their impact on cost? As diverse and independent as the specialty of anesthesiology is, its practitioners have challenged the leadership to take the lead in finding ways to provide quality care more consistently so that anesthesia is not a contributor to the cost of healthcare but a regulator of spending.
While virtually all anesthesiologists and CRNAs have now become familiar with the current requirements of the Physician Quality Reporting System (PQRS), this is just one example of a public approach to ensuring consistency based on...
The focus on quality outcomes in healthcare has been long in coming. As the cost of health care continues to rise faster than the cost of living, the nation finds itself facing a dilemma. Perhaps a free market approach to healthcare is not the best approach after all. Economic incentives and ground breaking research have clearly provided significant advances in some areas, but what has been their impact on cost? As diverse and independent as the specialty of anesthesiology is, its practitioners have challenged the leadership to take the lead in finding ways to provide quality care more consistently so that anesthesia is not a contributor to the cost of healthcare but a regulator of spending.
While virtually all anesthesiologists and CRNAs have now become familiar with the current requirements of the Physician Quality Reporting System (PQRS), this is just one example of a public approach to ensuring consistency based on...  By Abby Pendleton, Esq., Carey Kalmowitz, Esq. and Adrienne Dresevic, Esq. The Health Law Partners, P.C., Southfield, MI
On June 1, 2012, the Department of Health and Human Services Office of Inspector General (the “OIG”) issued its Advisory Opinion No. 12-06, which provides long-awaited guidance to the health care industry regarding the legal permissibility of an anesthesia delivery service model commonly referred to as the “company model.” Insofar as Advisory Opinion No. 12-06 is the initial OIG guidance that specifically focuses on such an arrangement and determines that the factual paradigms presented implicate risks under the Medicare and Medicaid Antikickback Statute (the “AKS”), this Advisory Opinion understandably is capturing broad attention within the medical and legal communities. While OIG Advisory Opinion 12-06 clarifies the almost-axiomatic observation that company model arrangements, especially those that contain the indicia that the OIG historically has identified as problematic under the AKS, certainly have the potential...
By Abby Pendleton, Esq., Carey Kalmowitz, Esq. and Adrienne Dresevic, Esq. The Health Law Partners, P.C., Southfield, MI
On June 1, 2012, the Department of Health and Human Services Office of Inspector General (the “OIG”) issued its Advisory Opinion No. 12-06, which provides long-awaited guidance to the health care industry regarding the legal permissibility of an anesthesia delivery service model commonly referred to as the “company model.” Insofar as Advisory Opinion No. 12-06 is the initial OIG guidance that specifically focuses on such an arrangement and determines that the factual paradigms presented implicate risks under the Medicare and Medicaid Antikickback Statute (the “AKS”), this Advisory Opinion understandably is capturing broad attention within the medical and legal communities. While OIG Advisory Opinion 12-06 clarifies the almost-axiomatic observation that company model arrangements, especially those that contain the indicia that the OIG historically has identified as problematic under the AKS, certainly have the potential...
The Office of the Inspector General (OIG) within the Department of Health and Human Services has published its Work Plan for 2013. On the list of Medicare issues on which the OIG will focus next year is the following:
Anesthesia Services—Payments for Personally Performed Services (New)
We will review Medicare Part B claims for personally performed
anesthesia services to determine whether they were supported in
accordance with Medicare requirements. We will also determine whether
Medicare payments for anesthesiologist services reported on a claim with
the “AA” service code modifier met Medicare requirements. Physicians
report the appropriate anesthesia modifier to denote whether the service
was personally performed or medically directed. (CMS’s Medicare Claims Processing Manual,
Pub. No. 100-04, ch.12, § 50) The service code “AA” modifier is used
for anesthesia services personally performed by an anesthesiologist, and
the “QK” modifier is used for medical direction of two, three, or four
concurrent...
 While the eventual fate of the Patient Protection Affordable Care Act (PPACA) will be decided in the near future, by either the Supreme Court or the next Congress and Administration, what is not open for debate is that healthcare has changed. As the business of medicine evolves to accommodate the changes called for in the healthcare reform laws, so should anesthesiologists anticipate their place in the new environment. The physician group that is able to make informed decisions will be best positioned to evolve and thrive in this era of change. Just like the old Saturday morning cartoon said, “Knowledge Is Power”; by gathering, understanding and responding to information, anesthesiologists can be certain to meet the needs of their clients and proactively position themselves as a catalyst for change.One way of taking that proactive step is to use data to help shine a light on the inner workings of your anesthesia...
While the eventual fate of the Patient Protection Affordable Care Act (PPACA) will be decided in the near future, by either the Supreme Court or the next Congress and Administration, what is not open for debate is that healthcare has changed. As the business of medicine evolves to accommodate the changes called for in the healthcare reform laws, so should anesthesiologists anticipate their place in the new environment. The physician group that is able to make informed decisions will be best positioned to evolve and thrive in this era of change. Just like the old Saturday morning cartoon said, “Knowledge Is Power”; by gathering, understanding and responding to information, anesthesiologists can be certain to meet the needs of their clients and proactively position themselves as a catalyst for change.One way of taking that proactive step is to use data to help shine a light on the inner workings of your anesthesia...  The acronym “HIPAA” has become a household name since the enactment of the Health Information Portability and Accountability Act of 1996, which, among other things, established rules for protecting and securing patients’ health information. In fact, it is not uncommon to hear about breaches of patient information costing healthcare providers and suppliers six and seven figure civil monetary penalties or settlements. Typically, such settlements and penalties have arisen out of patient complaints that the privacy of their protected health information (PHI) has been compromised. However, beginning November 2011, patient complaints will not be the only way in which the Department of Health and Human Services (HHS) Office of Civil Rights (OCR) will learn about non-compliant entities.Section 13411 of the American Recovery and Reinvestment Act of 2009, which established the Health Information Technology for Economic and Clinical Health (HITECH) Act, requires the Secretary of HHS to “provide for periodic audits to ensure...
The acronym “HIPAA” has become a household name since the enactment of the Health Information Portability and Accountability Act of 1996, which, among other things, established rules for protecting and securing patients’ health information. In fact, it is not uncommon to hear about breaches of patient information costing healthcare providers and suppliers six and seven figure civil monetary penalties or settlements. Typically, such settlements and penalties have arisen out of patient complaints that the privacy of their protected health information (PHI) has been compromised. However, beginning November 2011, patient complaints will not be the only way in which the Department of Health and Human Services (HHS) Office of Civil Rights (OCR) will learn about non-compliant entities.Section 13411 of the American Recovery and Reinvestment Act of 2009, which established the Health Information Technology for Economic and Clinical Health (HITECH) Act, requires the Secretary of HHS to “provide for periodic audits to ensure...  Every year, the time comes to begin looking at one or a set of payor contracts. A multitude of questions abound regarding appropriate rates, term length, and whether or not to participate or stay on panel. These are all good questions to raise. But are these the only questions to ask? This article seeks to explore the value of planning for payor negotiations.As a backdrop to the planning, it is important to remember the value of strategic planning as described by Sun Tzu:The general who wins a battle makes many calculations in his temple where the battle is fought. The general who loses a battle makes but few calculations beforehand. Thus do many calculations lead to victory, and few calculations to defeat: how much more no calculation at all! It is by attention to this point that I can foresee who is likely to win or lose.1The point is primarily to...
Every year, the time comes to begin looking at one or a set of payor contracts. A multitude of questions abound regarding appropriate rates, term length, and whether or not to participate or stay on panel. These are all good questions to raise. But are these the only questions to ask? This article seeks to explore the value of planning for payor negotiations.As a backdrop to the planning, it is important to remember the value of strategic planning as described by Sun Tzu:The general who wins a battle makes many calculations in his temple where the battle is fought. The general who loses a battle makes but few calculations beforehand. Thus do many calculations lead to victory, and few calculations to defeat: how much more no calculation at all! It is by attention to this point that I can foresee who is likely to win or lose.1The point is primarily to...  Abby Pendleton, Esq., The Health Law Partners, P.C., Southfield, MIStephanie P. Ottenwess, Esq., The Health Law Partners, P.C., Los Angeles, CAOn March 7, 2012, the Centers for Medicare and Medicaid Services (CMS) published its Notice of Proposed Rule Making (NPRM, or proposed rule) for Stage 2 user requirements for the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (“meaningful use,” or MU) in the Federal Register. 77 FR 13698.1 There is a three pronged focus to the Stage 2 criteria: standardizing data formats to dramatically simplify how information is both captured and shared across disparate IT systems in order to be better able to coordinate care with other physicians; ensuring that patients be able to access and easily download their healthcare records and images for their own use; and expanding the scope of tracked quality metrics to include specialists and to reflect and improve specific patient outcomes as well as care coordination.Although subsequent to...
Abby Pendleton, Esq., The Health Law Partners, P.C., Southfield, MIStephanie P. Ottenwess, Esq., The Health Law Partners, P.C., Los Angeles, CAOn March 7, 2012, the Centers for Medicare and Medicaid Services (CMS) published its Notice of Proposed Rule Making (NPRM, or proposed rule) for Stage 2 user requirements for the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (“meaningful use,” or MU) in the Federal Register. 77 FR 13698.1 There is a three pronged focus to the Stage 2 criteria: standardizing data formats to dramatically simplify how information is both captured and shared across disparate IT systems in order to be better able to coordinate care with other physicians; ensuring that patients be able to access and easily download their healthcare records and images for their own use; and expanding the scope of tracked quality metrics to include specialists and to reflect and improve specific patient outcomes as well as care coordination.Although subsequent to...
The percentage of patients requiring the highest level of service in the emergency department at Faxton St. Luke’s Healthcare in Utica, NY rose 43 percent in 2009, as reported in the New York Times on September 21, 2012. Level 5 ED visit services (CPT® code 99285) at Baptist Hospital in Nashville, TN increased by 82 percent in 2010, and by a comparable amount at Methodist Medical Center of Illinois in Peoria. More than 80 percent of Methodist Memorial’s Medicare ED evaluation and management (E/M) claims were for Level 5 services in 2010, as they were at Yuma Regional Medical Center in Yuma, AZ in 2007. At Baylor Medical Center in Irving, TX, 64 percent of all ED visits for Medicare patients were Level 5 services, and another 16 percent were Level 4.These are just a few examples of hospitals experiencing a startling rate of growth of high-intensity E/M services during the last few...
 The Anesthesia Quality Institute was chartered in 2009, and it began collecting case data in the National Anesthesia Clinical Outcome Registry (NACOR) on January 1, 2010. NACOR was designed to harness the power of the Information Age by aggregating and analyzing large quantities of data. Unlike traditional registries that depend on a trained abstractor to examine medical records and pull out the facts of interest, NACOR accumulates data by direct reporting from the electronic health records (EHR) that are in use every day, including administrative systems such as the ABC billing software and clinical support systems such as ePreop. As anesthesia practices become increasingly digital — driven by the “meaningful use” requirements of the federal government discussed elsewhere in this issue of the Communiqué — even larger quantities and types of data will be available. The barrier is no longer the creation of digital records; it is now the enormous challenge...
The Anesthesia Quality Institute was chartered in 2009, and it began collecting case data in the National Anesthesia Clinical Outcome Registry (NACOR) on January 1, 2010. NACOR was designed to harness the power of the Information Age by aggregating and analyzing large quantities of data. Unlike traditional registries that depend on a trained abstractor to examine medical records and pull out the facts of interest, NACOR accumulates data by direct reporting from the electronic health records (EHR) that are in use every day, including administrative systems such as the ABC billing software and clinical support systems such as ePreop. As anesthesia practices become increasingly digital — driven by the “meaningful use” requirements of the federal government discussed elsewhere in this issue of the Communiqué — even larger quantities and types of data will be available. The barrier is no longer the creation of digital records; it is now the enormous challenge...
October 1, 2012, as we noted in last week’s Alert, is the deadline for ambulatory surgical centers to begin reporting quality measures to CMS or face payment penalties. October 1st is also a momentous date for hospitals, with the start of the Medicare Hospital Inpatient Value-Based Purchasing (VBP) Program.Value-Based Purchasing for HospitalsThe VBP Program is scheduled to launch a week from now, as required by the Affordable Care Act. This program marks the beginning of an historic change in how Medicare pays health care providers and facilities—for the first time, hospitals across the country will be paid for inpatient acute care services based on care quality, not on the quantity of the services they provide.In fiscal year 2013, which starts on October 1st, the VBP Program will pay out an estimated $850 million to more than 3,500 participating hospitals based on their overall performance on a set of twenty quality measures....
New Technology Enables Anesthesiologists and Pain Management Specialists to Attest to Meaningful UseWith the deadline fast approaching, more and more anesthesiologists are wondering if there is a quick and easy way to qualify for the Medicare Meaningful Use Incentive.The Medicare and Medicaid EHR Incentive Program provides a financial incentive of up to $44,000 per provider for achieving "meaningful use," which is the use of certified electronic health record(EHR) technology to achieve health and efficiency goals. Stage 1 EHR meaningful use is based on core and menu objectives for eligible professionals as outlined by CMS—which are intended to set a baseline for electronic data capture and information sharing.ABC Can Help You Reap the Benefits of Meaningful Use Through Full EHR with F1RSTUseAnesthesia Business Consultants, LLC (ABC) is pleased to offer the anesthesia community a first—a viable way for anesthesiology and pain management practices to attest to Stage 1 Meaningful Use. Introducing F1RSTUse,...
We are in the fifth year of Medicare’s Physician Quality Reporting System (PQRS) and most anesthesiologists and nurse anesthetists are at least aware of the program, even if they are not participating. Now it is the turn of the ambulatory surgery centers (ASCs) to start reporting quality measures to CMS or face payment penalties.Not only are anesthesiologists generally involved in the quality and safety protocols that ASCs must report, many are in leadership or management positions in their ASCs and have a particular interest in compliance with reporting requirements. Whether or not they are directly responsible for the completeness and accuracy of the reporting—the new ASC requirements do not in any way require anesthesiologists to report any measures, but some may voluntarily assume the role within and for their facility—ASC anesthesiologists will benefit from understanding what procedural changes the facility is making, and why. Beginning October 1, 2012, the ASC Quality Reporting...
Many “Covered Entities” within the meaning of the privacy and security provisions of the Health Insurance and Portability Act of 1996 (HIPAA) are managing more and more of their patient information electronically. Indeed, not moving to electronic health records (EHRs) may cost physicians a percentage of their Medicare remittances—or at least the loss of a potential bonus of up to $44,000—under the EHR Incentive Program, as discussed in our last several Alerts.Collecting, analyzing, reporting and storing electronic patient information present perhaps even greater HIPAA challenges than does the use of paper records, however. Data entered on a computer can be copied more easily, more cheaply, more prolifically and even passively. Once unsecured data are moved from the computer on which they are created to other media, manually or wirelessly, controlling the information becomes nearly impossible. The key word in the preceding sentence is “unsecured.” The recently finalized HIPAA regulations on Breach Notification impose...
Last week, we announced the availability of a new web-based electronic health record (EHR) that will permit anesthesiologists to satisfy the Meaningful Use requirements for the Medicare EHR Incentive Program. Although this technology, F1RSTUse, is relatively simple, requires little additional data entry and is an option for ABC clients and non-clients alike, it will not be the best solution for every reader. Those of you who are not in a position to implement F1RSTUse or any EHR will be interested in a new hardship exception created by CMS when it released the final regulation on the Stage 2 Meaningful Use requirements on August 23, 2012.Anesthesiologists not participating in the EHR Incentive Program are the targets of the new exception based on “scope of practice,” along with radiologists and pathologists. In the final rule, CMS added a new section, §495.102(d)(4)(iv), to the regulations which provides that “eligible professionals” (EPs) who designate their...
New Technology Enables Anesthesiologists and Pain Management Specialists to Attest to Meaningful Use
On Thursday, August 23, 2012 the Centers for Medicare and Medicaid Services (CMS) released the final rule on Stage 2 of the federal electronic health record (EHR) system incentive program.ABC is very pleased to announce F1RSTUse, the first complete EHR platform built exclusively for anesthesiologists and pain management specialists to satisfy easily Stage 1 of Meaningful Use as required to earn the Medicare EHR incentive payment. Stage 1 requirements remain in effect for the next several years; one of the major changes of the August 23rd final rule was to extend the deadline to meet Stage 2 criteria until 2014. Other changes contained in the 672-page rule (PDF) will be reviewed in future Alerts.The industry has been discussing the impracticality of attesting to Meaningful Use with current technologies and relationships that are in place for anesthesia. We at ABC also noted the lack of ease implementing this requirement for the specialty. Attestation was...
Advanced Integration Streamlines Data Collection to Speed Billing, Improve Efficiency and Enhance AnalysisAnesthesia Business Consultants (ABC) announces that it has partnered with Surgical Information Systems (SIS), a leading anesthesia information management system (AIMS) provider, to streamline revenue cycle workflow. The alliance provides integration that enables data captured in SIS’ AIMS to flow into ABC’s anesthesia billing tools to improve billing accuracy and timeliness. It also offers analytics capabilities that enable ABC clients to collect and analyze anesthesia-specific perioperative data.With over 300 successful perioperative implementations, SIS solutions deliver proven benefits to anesthesia providers and hospitals across the United States and Canada. SIS is recognized by top industry associations for its commitment to advance anesthesia solutions. SIS was the first AIMS provider to achieve Anesthesia Quality Institute (AQI) Preferred Vendor status, and SIS Anesthesia is exclusively endorsed by the American Hospital Association (AHA) indicating the solution has met AHA requirements for quality, integrity,...
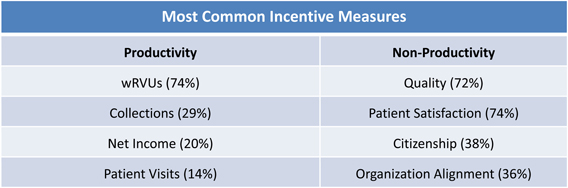 Preparing for negotiations requires an appreciation of the other side’s needs, wants, values and constraints. Anesthesiologists who have contracts with their hospitals or surgery centers are in a continuous cycle of negotiations—as soon as one contract is signed, it is time to start working toward the next agreement. One good place to start in understanding the facility’s position is to look at the advice hospitals are receiving from their consultants. Below is an article recently written for that audience by ABC Vice President for Regulatory Affairs & Research Joette Derricks, CPC, CHC, CMPE, CSSGB. This article addresses hospital employment of physicians who bill using RBRVS Relative Value Units, and of course anesthesiologists use the Relative Value Guide’s Base and Time Unit methodology and typically have group exclusive contracts to provide services to the hospital’s patients, but the discussion below can be read with the differences in mind. It is important to...
Preparing for negotiations requires an appreciation of the other side’s needs, wants, values and constraints. Anesthesiologists who have contracts with their hospitals or surgery centers are in a continuous cycle of negotiations—as soon as one contract is signed, it is time to start working toward the next agreement. One good place to start in understanding the facility’s position is to look at the advice hospitals are receiving from their consultants. Below is an article recently written for that audience by ABC Vice President for Regulatory Affairs & Research Joette Derricks, CPC, CHC, CMPE, CSSGB. This article addresses hospital employment of physicians who bill using RBRVS Relative Value Units, and of course anesthesiologists use the Relative Value Guide’s Base and Time Unit methodology and typically have group exclusive contracts to provide services to the hospital’s patients, but the discussion below can be read with the differences in mind. It is important to...  Does the title of this article seem boring – or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences...
Does the title of this article seem boring – or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences...