How the MACRA Regulations as Proposed Will Affect Anesthesiologists, Part II (Alternative Payment Models)
Last week’s e-Alert introduced our readers to the proposed regulations implementing the MACRA Quality Payment Program (Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models). We focused in Part I on the MIPS pathway, which consolidates Medicare’s current quality, cost and EHR reporting programs and promised an overview of the second major physician payment pathway set forth in the proposed rule, the APM Incentive program.
All eligible clinicians will be participating in either the MIPS or the APM program in the near future, as the Physician Quality Reporting System (PQRS), the Value-Based Modifier (VBM) program and the EHR Incentive-Meaningful Use (MU) program phase out, by the end of 2018. Beginning on January 1, 2019, payments will reflect participation in MIPS or APM, based on each clinician’s performance in 2017. The APM incentives are as follows:
- For payment years 2019 to 2024, a lump sum payment equal to five percent of the estimated aggregate payment amounts for Medicare Part B services for the prior year;
- Exemption from MIPS; and
- For payment years 2026 and later, payment rates under the Medicare physician fee schedule for services furnished by the eligible clinician will be updated by 0.75 percent.
The proposed rule’s stringent criteria for qualifying APMs will relegate most anesthesiology practices to participating in MIPS. To be a “Qualifying APM Participant” (QP) the individual clinician must participate in an “Advanced APM.” Advanced APMs are defined so narrowly that almost no one will be able to choose that option. It is, nevertheless, important to understand CMS’s actions with respect to APMs because MIPS is a transitional program. Everything leads toward APMs.
Advanced APMs are the CMS Innovation Center models, Shared Savings Program tracks, or statutorily-required demonstrations where clinicians accept both risk and reward for providing coordinated, high quality and efficient care.
CMS proposes two types of Advanced APMs: Medicare Advanced APMs and “Other Payer Advanced APMs.” An Other Payer Advanced APM allows eligible clinicians to participate in an APM through non-Medicare payers, such as commercial plans or state Medicaid programs offering an APM. (The Other Payer Advanced APM will be available in payment year 2021.) APMs seeking to qualify under either of these types must meet all of the following requirements:
- The use of certified EHRs;
- Payment for covered professional services based on quality measures comparable to those found in MIPS; and
- Either (a) the Advanced APM Entity bear financial risk for monetary losses that are in excess of a nominal amount or (b) is a nationally recognized accredited patient-centered medical home, expanded under Section 1115A(c) of the Social Security Act.
MACRA itself created the requirement that APMs bear financial risk, and many providers and other interested parties have been waiting to see how CMS would define the amount of risk an APM must bear to quality. CMS proposes a “generally applicable financial risk standard” that requires APMs to include provisions that, if actual expenditures exceed expected expenditures, CMS can withhold payment, reduce payment rates or require the APM to incur a debt to CMS. The risk must be more than nominal, i.e., “meaningful for the entity but not excessive.” Could the standard be more subjective?
Additionally, to qualify clinicians for enhanced payments under MACRA, APMs must be compulsory, have a clear “thesis” that they are testing and require participants to have a formal agreement with CMS. If APMs offer multiple tracks varying the degree of financial risk or tailoring participation to different types of organizations, CMS would “assess the eligibility of each such track or option within the APM independently.” CMS proposes to notify the public of the APMs qualifying as Advanced APMs prior to each performance period, which will begin no later than January 1, 2017. Anesthesiologists should consult this list if they wish to make sure that an APM that they are considering joining is on the list. Table 32 in the proposed regulation contains a preliminary list showing APMS that qualify and do not qualify as “Advanced.”
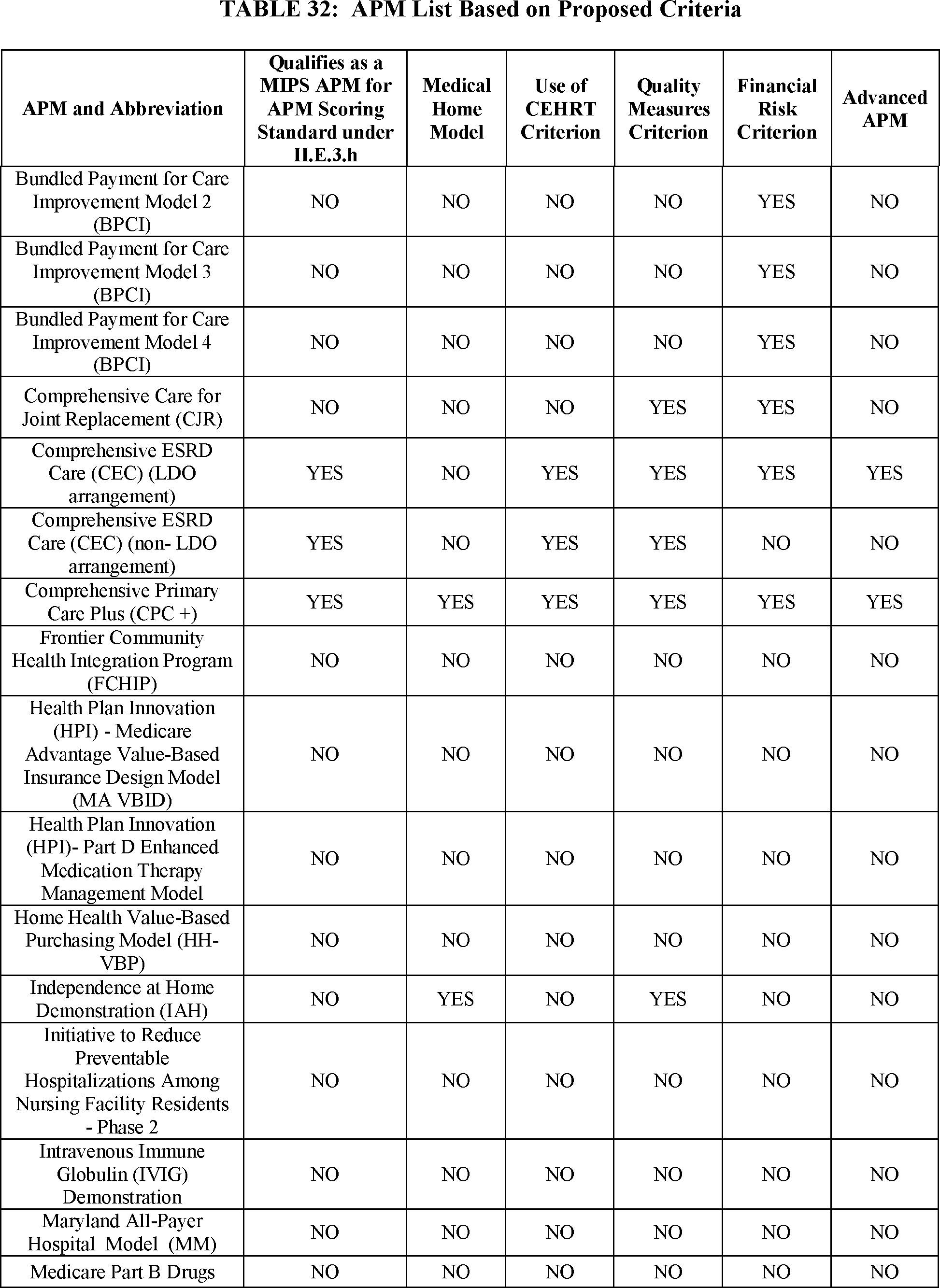{kind=link}

For an eligible clinician to be considered a QP and qualify for the incentive payment, he or she must be part of an Advanced APM, which meets or exceeds the financial risk and patient count thresholds. Clinicians must participate in an Advanced APM for at least one year to become a QP.
Eligible clinicians who do not qualify as QPs may qualify as Partial QPs by meeting slightly lower financial risk or patient count thresholds. Partial QPs are not eligible for the five percent APM incentive payment or, after 2025, for the 0.75 percent increase in the Medicare conversion factor. However, they could choose whether or not to be subject to the MIPS payment adjustment (which could be positive or negative).
CMS estimates that in 2019, the first year in which there will be a payment consequence for MIPS performance, between approximately 30,658 and 90,000 eligible clinicians would become QPs through participation in Advanced APMs and will receive between $146 million and $429 million in APM incentive payments. Those ranges are not quite as wide as they might appear when one considers that the elaborate conditions for qualification of APMs and QPs in the proposed rule may undergo substantial changes before they are finalized toward the end of this year. As Jordan T. Cohen and Thomas S. Crane wrote in the latest installment of their blog, Alternative Payment Models (APMs) Under MACRA Proposed Rule, the proposal “is extensive, subject to change, with deadlines likely extended. Nevertheless, the proposed rule gives a clear road map of Congress and CMS’s expectations for physicians to thrive under this new payment model that moves away from fee-for-service payments based on volume toward an incentive system that rewards the provision of higher quality and value service with a greater patient-centered focus.”