eAlerts
-
April 4, 2022
While academic anesthesia departments often provide services in the Intensive Care Unit (ICU), this is quite rare among private practices. Hence the question, why more private practices don’t want to take responsibility for the care of post-surgical patients in the ICU? It would seem that covering the ICU was a logical line extension and entirely consistent with the concept of the peri-operative surgical home. Isn’t the cardiovascular anesthesiologist who managed the patient through a CABG or mitral valve repair the ideal person to ensure that the patient recovers well in the ICU? As is true of so many aspects of medical care, the answer to the question involves tradition, politics and economics.
-
November 8, 2021
A critical aspect of any governance model is succession planning. Identifying and developing strong leadership and assuring a peaceful transition of power are items that need to be added to every group’s strategic planning agenda.
-
March 29, 2021
Each year the American Society of Anesthesiologists (ASA) publishes an updated version of its Relative Value Guide (RVG). Most updates include only minor coding changes, although every so often there are relevant policy statement updates. The revisions contained within the 2020 RVG stand as a significant exception. This is because a certain set of flat-fee services that had previously been assigned base unit values within earlier RVG editions were now listing only work relative value units (RVUs) for these services. The table below includes three representative examples.

From a billing and management perspective, all anesthesia services can be divided into three categories: time-based surgical services, obstetric anesthesia and flat fees. This distinction reflects the three basic payment methodologies used by payers. Surgical anesthesia services are paid based on a base-plus-time formula. Obstetric anesthesia (OB) may be paid based on base plus time, but there are often specific rules for the amount of time that can be paid, and some payers adjudicate OB claims based on flat fees.
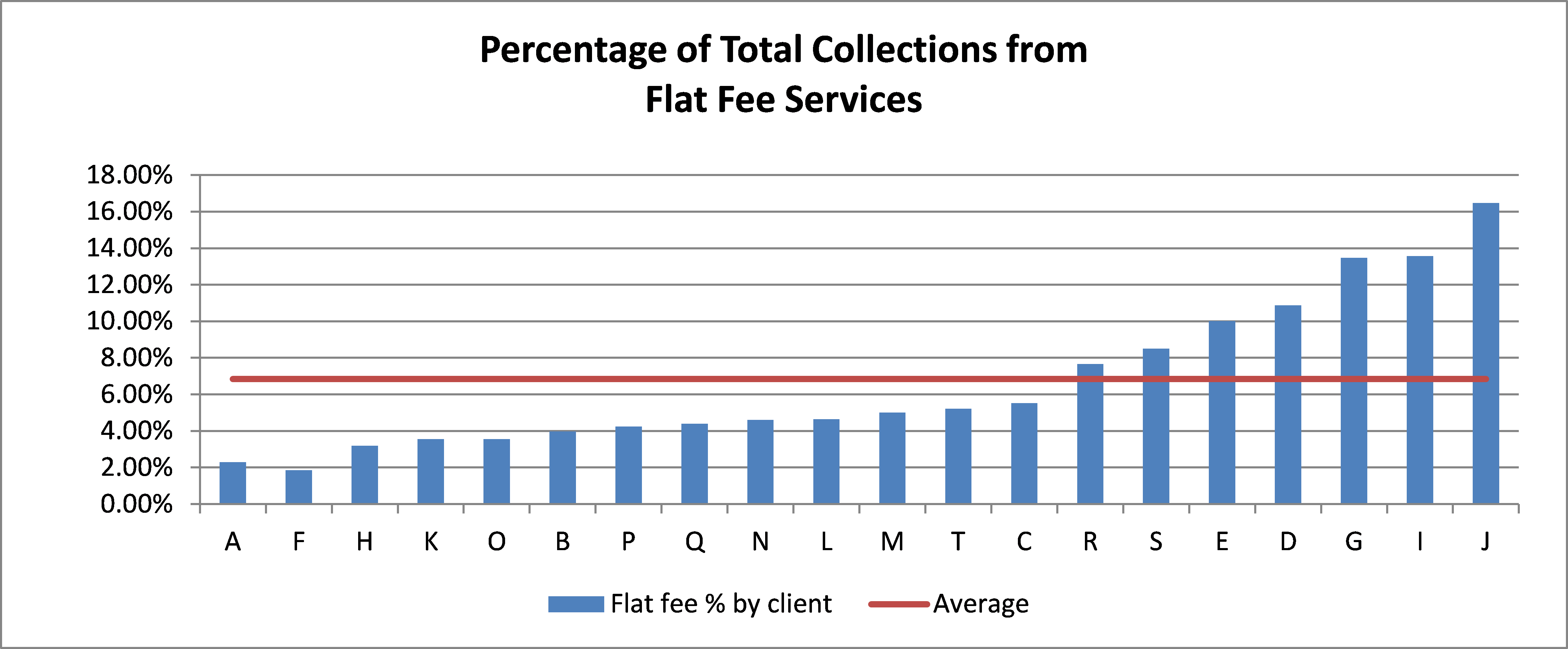
Non-time-based services are paid from a fee schedule and may be subject to other considerations based on Correct Coding Initiative (CCI) rules. Traditionally, this category includes three distinct subsets: invasive monitoring, nerve blocks and ultrasonic guidance (USG), as well as follow-up visits. There has been a dramatic increase in the number of nerve blocks performed in the past few years, which has represented a significant increase in revenue for some clients. The chart below indicates the percentage of flat fee collections received by a sample of 20 clients for services performed in 2020. Even though that was the year of the pandemic, these percentages are representative of typical practice trends, and we would expect them to hold true for 2021, as well.
Portion of Practice
The diversity of rates raises some interesting questions. Why do some practices get such a small percentage of collections from flat fee services? Typically, this is because their practitioners do not perform many nerve blocks for acute pain management. This may be a revenue opportunity or it may simply be a reflection of the fact that a higher percentage of services are provided in ambulatory surgery centers where nerve blocks are less commonly performed.
The ASA decision to drop the base values from the guide is a reflection of the current contracting reality. The majority of anesthesia contracts with payers specify an anesthesia unit rate. Increasingly, flat fee services default to some percentage of Medicare rates. Most anesthesia practices will go to the mat to get the best unit rate possible for their surgical and OB services. However, they often neglect to request reasonable payment for their flat fee service, and this may be another revenue opportunity—especially if they perform blocks routinely. For our clients, we negotiate these flat fee rates simultaneously with the anesthesia rates on an annual basis.
Impact on Practice
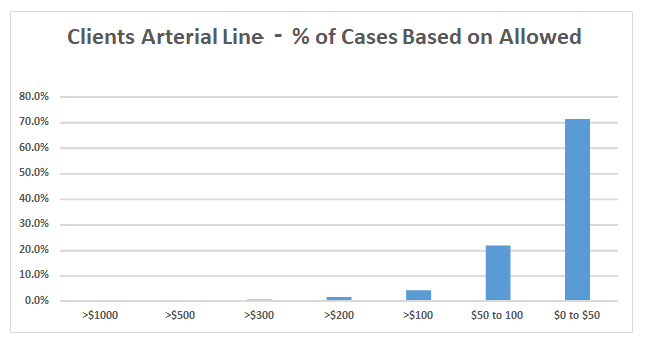
The three charts below reflect the current reality of flat fee billing. Taking the three codes listed above, we have done an analysis of a large sample of our clients to see what percentage of services were paid at or around the Medicare allowable. While some practices may have a few plans that still pay for these services based on the historical ASA base values, these are very much the exceptions. It should be noted that, for this analysis, we only considered the payer allowable amount. We did not consider the impact of patient responsibility.
The average Medicare allowable for arterial line placements is $47.63. We determined that 56.5 percent of all arterial lines billed on behalf of the sample clients in 2020 were paid at the Medicare allowable rate.
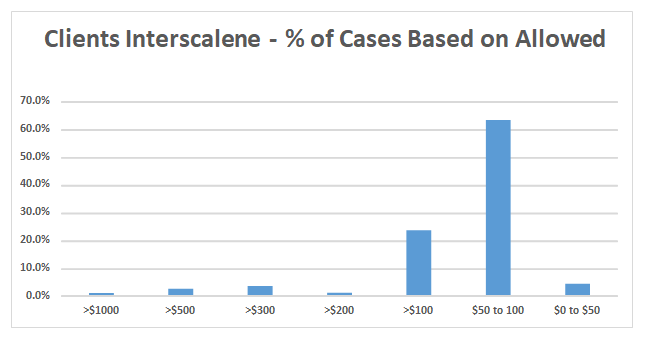
The average Medicare allowable for interscalene blocks was $68.04. In this sample, 33 percent of all procedures were paid at the Medicare rate. In addition, we found that 67.7 percent were paid at less than $100.
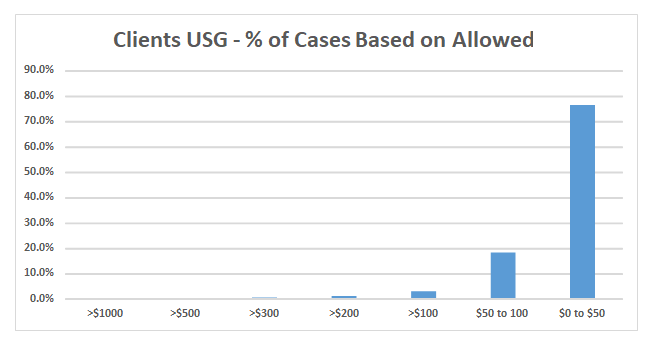
The average Medicare allowable for USG is $33.64. USG services for blocks are routinely paid when used for needle guidance for interscalene, femoral and sciatic blocks. It is not separately payable for TAP blocks.
Opportunity for Practice
It used to be that the ASA Relative Value Guide was the gold standard for contracting. While that may still be true for surgical and OB anesthesia services, it is definitely no longer the case for all the separately payable procedures practitioners are now performing. It is this reality that the current RVG now reflects.
What can we conclude from this analysis? Clinically appropriate non-time-based services, such as nerve blocks, represent additional financial benefit on existing surgical volume. Taking full financial advantage of the opportunity requires that the practice’s contracting strategy takes them into consideration in order to negotiate reasonable fee schedules. This is just one of the inherent challenges for the specialty. Windows of opportunity for practice enhancement in the current environment are often elusive. With purposeful leadership, such opportunities may be seized.
For further discussion regarding the flat fee services within your practice, please reach out to your account executive or contact us at info@anesthesiallc.com.
With best wishes,
Tony Mira
President and CEO -
May 24, 2021
In last week’s e-alert, we discussed the various policy issues associated with the use of nurse practitioners (NPs), physician assistants (PAs) and nurse anesthetists (CRNAs) in a chronic pain practice. That discussion raised a number of practical questions about the services that these non-physician practitioners (NPPs) actually provide and the economics of using these providers in a chronic pain practice. As a follow-up to that article, today’s alert takes a deeper dive into the numbers. For the purpose of this discussion, we will focus solely on PAs.
-
September 14, 2020
The majority of our clients do not work in facilities that have an anesthesia electronic medical record (EMR). Despite some early trepidation about the transition from a paper record to an EMR, most installations have gone fairly smoothly. The majority of our clients report that they are reasonably happy with the new system. As is so often the case with new technology, younger physicians tended to embrace EMRs faster and more enthusiastically than their older colleagues. Although there was once a variety of companies offering an anesthesia EMR, the field has contracted considerably. Epic and Cerner now dominate the market for inpatient systems. Anesthesia Touch—a product we developed—is also a popular option for hospitals still on paper, as well as for outpatient facilities.