How Much Call is Too Much?
Robert Johnson, MBA Principal
Enhance Healthcare Consulting, Aventura, FL
 Anyone who has had to leave in the middle of a family dinner because of a call from labor and delivery or tried to sleep in the call room knowing that a recently completed case is bleeding and likely to come back that night probably also wonders whether they should be working somewhere with less call responsibility.
Anyone who has had to leave in the middle of a family dinner because of a call from labor and delivery or tried to sleep in the call room knowing that a recently completed case is bleeding and likely to come back that night probably also wonders whether they should be working somewhere with less call responsibility.
Working on call is part of the responsibility of being an anesthesiologist. It can also be an annoyance that can interfere with work/life balance. Driving back to the hospital for the second time on a beautiful Saturday afternoon, you may start to wonder whether you are on call more than others and possibly working in the wrong place. But how would you know? Your job may pay well and offer generous retirement benefits, but perhaps a job without cardiac, obstetric or trauma unit call responsibilities would make your life easier.
You might find an opportunity that pays less with fewer call days. Should you take the trade-off or keep looking?
The lack of published data on the frequency of required call responsibility among anesthesiologists makes it hard to compare professional opportunities. Surveys of compensation and time off are not hard to find. The same is not true for call.
Data is also lacking on the various types of call, including call from home (beeper call) and in-house call for hospitals that require 24/7 on-site coverage. The number of hours spent on call at the hospital also matters to many. If a position doesn’t require an obstetric beeper call rotation every other weekend, but requires in-house trauma call for the entire weekend, but only once a month, which is better? What are other anesthesiologists in your area required to do?
Colleagues often ask about the “typical” or “average” amount of call and how much call is “too much.”
 The lack of national published data prompted Enhance Healthcare to conduct its own survey utilizing Survey Monkey in order to gather information about the frequency and types of call taken by anesthesiologists across the United States.
The lack of national published data prompted Enhance Healthcare to conduct its own survey utilizing Survey Monkey in order to gather information about the frequency and types of call taken by anesthesiologists across the United States.
Our initial assumption was that there are two basic types of call about which to ask: 1) call from home (beeper call) and 2) in-house (restricted). We wanted to understand what circumstances led to various on-call requirements and whether and where call was provided by anesthesiologists compared to CRNAs. Finally, we wanted to see whether there were any significant relationships between specialty considerations and amount or type of call. We were particularly interested in 1) obstetric services (and the number of deliveries); and 2) trauma services and trauma classification level (I, II or III).
The survey consisted of eight to 13 questions, the total number of questions depending on answers to conditional questions (see Table 8 at the end of this article). Of 155 responses received, 21 responses were eliminated due to a lack of appropriate information.
We believe, but cannot demonstrate, that the remaining 134 respondents were all affiliated with different facilities. Therefore, the survey would represent 134 providers at 134 facilities. The surveys were distributed to anesthesia professionals across the country, so we believe the results are not skewed to any particular geographic area. We also stress that the results discussed in this article were not statistically validated at the time of publication. However, we intend to do so in future articles utilizing more sophisticated analyses, such as analysis of variance (ANOVA).
Beeper or In-house
 The first four survey questions asked respondents to report whether they take weekday and/or weekend call from home (beeper call) or in-house. The data revealed little or no difference in weekday versus weekend for either type of call (see Charts 1 and 2). The lack of difference between weekday and weekend values is probably due to the fact that, except for a few respondents, the same individuals who take weekday call also take weekend call.
The first four survey questions asked respondents to report whether they take weekday and/or weekend call from home (beeper call) or in-house. The data revealed little or no difference in weekday versus weekend for either type of call (see Charts 1 and 2). The lack of difference between weekday and weekend values is probably due to the fact that, except for a few respondents, the same individuals who take weekday call also take weekend call.

The data did show that there were three categories of call: 1) beeper only; 2) in-house only; and 3) a mix of beeper and in-house. Approximately 57 percent of respondents have (weekday and weekend) in-house call an average of five days per month. (See Table 1.) Approximately 85 percent of respondents have (combined weekend and weekday) beeper call as some component of their call an average of 7.8 days from home per month.

The combined results show that a typical provider taking in-house call could expect their facility to require an average of six days per month on-site in the hospital. A provider at a facility requiring beeper call could expect, on average, to spend eight days per month on beeper call. A limitation of the survey was that it did not ask respondents to indicate first call versus second call; however, the results suggest that the average provider at a typical facility has slightly more than one call day weekly (presumably first call) and one weekend per month.
Taking only in-house call and only beeper call represent 57 percent and 85 percent of respondents, respectively.
 Along with the number of days spent on call, time spent continuously on-site is also an issue. Since the in-house providers who responded to the survey were working an assigned shift (i.e., only 24 hours), only respondents taking call from home were asked how long they spent on-site when called in from home. Tables 2 and 3 show that, on average, anesthesiologists spend a little over four hours on a weekday and over seven hours on a weekend day on-site when called into the facility from home. The authors note that, to their surprise, the total hours spent on-site did not appear to differ significantly by specialty being covered at the facility. We are planning a follow-up study on this topic.
Along with the number of days spent on call, time spent continuously on-site is also an issue. Since the in-house providers who responded to the survey were working an assigned shift (i.e., only 24 hours), only respondents taking call from home were asked how long they spent on-site when called in from home. Tables 2 and 3 show that, on average, anesthesiologists spend a little over four hours on a weekday and over seven hours on a weekend day on-site when called into the facility from home. The authors note that, to their surprise, the total hours spent on-site did not appear to differ significantly by specialty being covered at the facility. We are planning a follow-up study on this topic.


In-house On-Call Characteristics
We asked participants whether their facility required in-house call (on-site presence 24/7). Hospitals typically refer to in-house call as “restricted call” and beeper call as “unrestricted call.” Sixtyseven percent of respondents reported that their facilities require in-house call (Chart 3). One would expect that the percentage of respondents taking in-house call, either with or without a beeper, would be close to this percentage. However, as shown in Charts 1 and 2, the combined percentage for weekday and percent difference. This may be because providers who do not take in-house call work at facilities where in-house call is required of others (e.g., obstetric anesthesiologists or CRNAs). Chart 4 compares CRNA and physician anesthesiologist providers.



On-Call Characteristics By Specialty: Obstetrics
 Eighty-three percent of respondents indicated that their facilities had an obstetrics program. Annual deliveries ranged from 300 to 11,000. Table 4 shows the impact of an obstetrics program on percentages of call type. Days of call type per month do not appear to differ significantly between obstetric and non-obstetric call. (Thirteen respondents indicated an obstetrics program at their institutions but did not provide an annual number of births. Their responses were not included in calculations involving the number of births.)
Eighty-three percent of respondents indicated that their facilities had an obstetrics program. Annual deliveries ranged from 300 to 11,000. Table 4 shows the impact of an obstetrics program on percentages of call type. Days of call type per month do not appear to differ significantly between obstetric and non-obstetric call. (Thirteen respondents indicated an obstetrics program at their institutions but did not provide an annual number of births. Their responses were not included in calculations involving the number of births.)
However, the proportions of call types were significantly different in obstetrics, particularly in the “in-house only” and “beeper only” categories. This is consistent with our finding suggesting that the size of an obstetrics program would have an impact on whether or not it had an in-house call component. Further study is warranted to separate other variables such as trauma and use of CRNAs for in-house call.
On-Call Characteristics By Specialty: Trauma
Forty-eight percent of the respondents worked at a facility with a trauma program. There were few differences in the number of trauma on-call days between facilities with and without trauma programs, with the exception of a decrease in beeper-only call from 9.6 to 8.7 days. As with obstetrics, the presence of a trauma program alone does not appear to change the number of days on call. We are planning an additional study to analyze the confounding variables of obstetrics and trauma in programs with and without CRNAs.


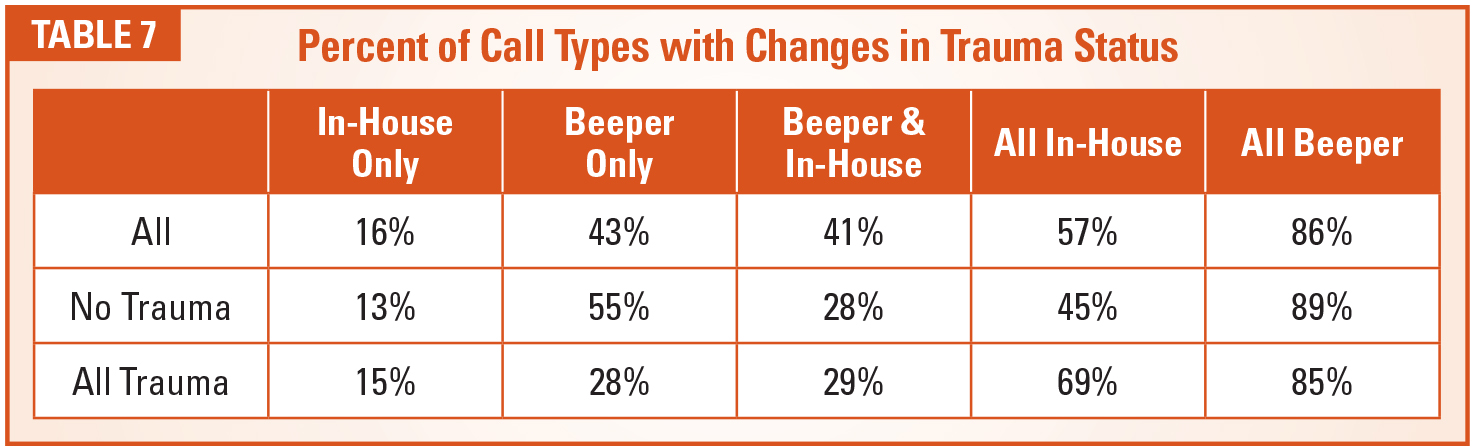
As seen in Table 6, trauma programs do have an impact on the proportions of call type. The most dramatic difference was seen in beeper only call in institutions with and without a trauma center (28 percent and 55 percent, respectively).
Not surprisingly, there was an apparent correlation between trauma level and number of days and types of call. (Level I and II trauma programs require 24/7 anesthesia in-house coverage.)
A preliminary view of the differences to be analyzed in future reports is shown in Chart 6. As stated earlier, the use of CRNAs has a large impact on the absolute number of physician anesthesiologists used for call, but the number also varies by trauma level.



Conclusion
 How much call an anesthesiologist takes is subject to many variables. This study looked at weekdays, weekends, obstetrics and trauma. There do not appear to be differences between weekday and weekend coverage. Neither the number of days nor the hours per day required on-site for call appear to differ much between the facilities that require obstetric and trauma coverage. However, the relative proportions of call responsibility for beeper and in-house call reveal significant differences.
How much call an anesthesiologist takes is subject to many variables. This study looked at weekdays, weekends, obstetrics and trauma. There do not appear to be differences between weekday and weekend coverage. Neither the number of days nor the hours per day required on-site for call appear to differ much between the facilities that require obstetric and trauma coverage. However, the relative proportions of call responsibility for beeper and in-house call reveal significant differences.
Further study to analyze the covariant impact on this phenomenon is warranted, along with further review of the impact of the various trauma levels.
The answer to the question of how much call is too much call is: it’s complicated! At a minimum, clinicians should carefully review call requirements for any practice they are thinking of joining, with consideration for the potential impact of obstetrics and trauma on how much inhouse coverage they will be required to provide.
 Robert Johnson, MBA, principal at Enhance Healthcare Consulting, is a healthcare executive with broad experience in multiple healthcare environments. He started at Johns Hopkins Hospital as a perfusionist in the cardiac operating rooms and eventually became administrator of the anesthesiology department. He has also served as senior associate chief operating officer at Duke Hospital and held positions with Baylor College of Medicine, the University of Pittsburgh and Sheridan Healthcare. As a vice president for Hospital Corporation of America, he played a critical role in leading negotiations with hospital-based physician practices. He joined EHC as a principal in 2014. He can be reached at bob.johnson@enhancehc.com or (404) 905-7014.
Robert Johnson, MBA, principal at Enhance Healthcare Consulting, is a healthcare executive with broad experience in multiple healthcare environments. He started at Johns Hopkins Hospital as a perfusionist in the cardiac operating rooms and eventually became administrator of the anesthesiology department. He has also served as senior associate chief operating officer at Duke Hospital and held positions with Baylor College of Medicine, the University of Pittsburgh and Sheridan Healthcare. As a vice president for Hospital Corporation of America, he played a critical role in leading negotiations with hospital-based physician practices. He joined EHC as a principal in 2014. He can be reached at bob.johnson@enhancehc.com or (404) 905-7014.