Anesthesiologists in the ICU: Economics and Other Considerations
Jody Locke, MA
Vice President of Anesthesia and Pain Management Services Anesthesia Business Consultants, Jackson, MI
 Very few private anesthesia practices provide services in their hospitals’ intensive care units (ICUs). The lack of enthusiasm for staffing the ICU relates directly to a perception that ICU coverage is not as profitable as operating room (OR) coverage. The entire Anesthesia Business Consultants client database only yields a few examples of private anesthesia practices covering the ICU. Are these outliers visionary or just clinical exceptions? In the current environment where a principle focus of payment reform is on bundled payment arrangements, it may be time to review what were once considered core competencies of anesthesiologists and reassess the strategic opportunity to enhance the scope of the relationship between the anesthesia practice and the facility.
Very few private anesthesia practices provide services in their hospitals’ intensive care units (ICUs). The lack of enthusiasm for staffing the ICU relates directly to a perception that ICU coverage is not as profitable as operating room (OR) coverage. The entire Anesthesia Business Consultants client database only yields a few examples of private anesthesia practices covering the ICU. Are these outliers visionary or just clinical exceptions? In the current environment where a principle focus of payment reform is on bundled payment arrangements, it may be time to review what were once considered core competencies of anesthesiologists and reassess the strategic opportunity to enhance the scope of the relationship between the anesthesia practice and the facility.
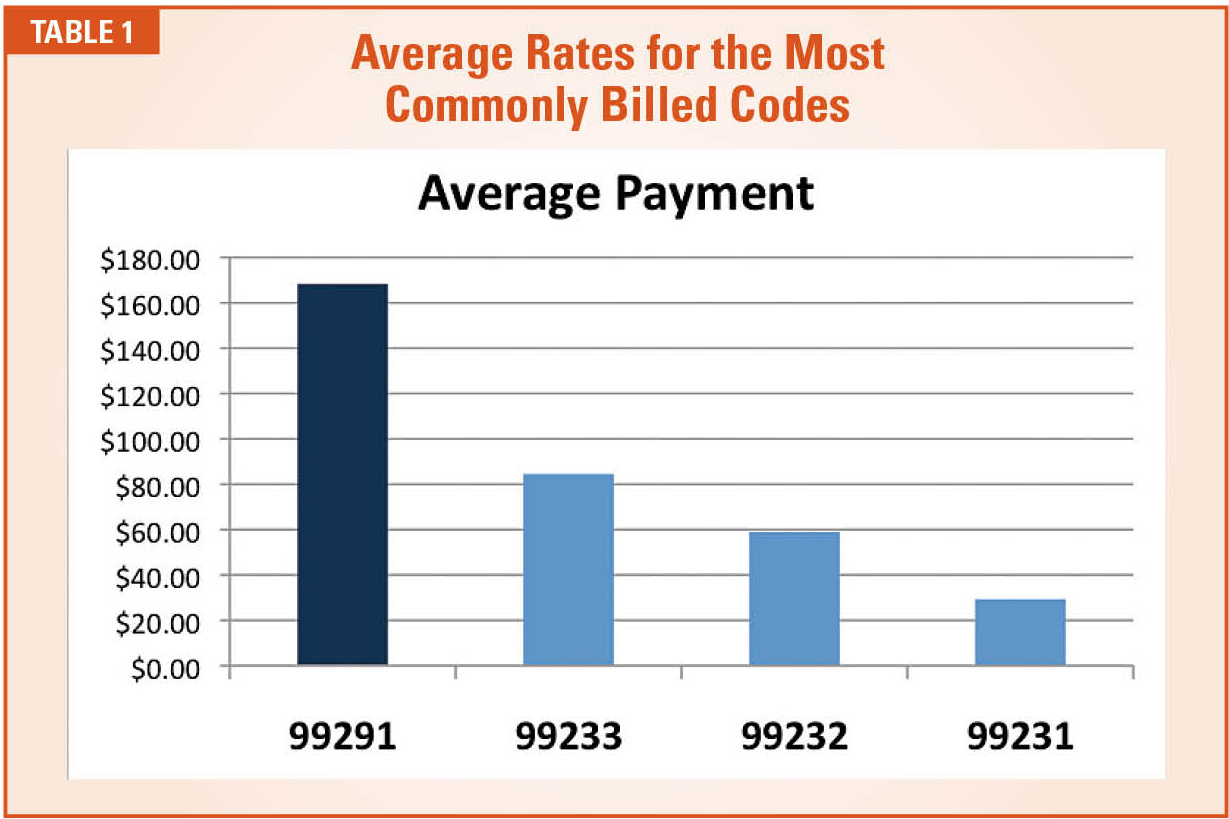
Quite different from anesthesia billing, ICU billing involves some unique compliance considerations. Conceptually, all patients must be triaged based on acuity of care. If a new patient introduced into the unit receives a full workup that takes an hour or more, the work would probably be billed with CPT Code 99291 (CPT Code 99291 – critical care, evaluation and management of the critically ill or critically injured patient; first 30-74 minutes), but specific criteria have to be met. If the acuity of care does not meet the CPT criteria, then the workup must be down-coded to a subsequent hospital visit, which is paid at a considerably lower rate. Table 1 indicates average rates for the most commonly billed codes. Obviously, the overall yield per workup will depend on the mix of patients and the conditions they present.
Most patients brought from the OR to the ICU will be stabilized on the first day, resulting in diminished acuity of care over time. A high-level initial workup would normally lead to one or more low-level hospital visits before the patient is released to the floor. As such, the revenue opportunity diminishes.
Most of the ICU codes include all the intensivist’s usual services, but some other services may be billed in addition to these as evaluation and management (E&M). The placement of invasive monitoring (arterial lines, central venous pressure (CVP) and Swan-Ganz catheters) may be inserted and paid separately. It is also possible that a patient might need an intubation only, which would be payable as a stand-alone service.
Economic Realities
 The economics of ICU coverage hinges on three factors: the volume of patient encounters, the acuity of care provided as assessed on a case-by-case basis and the payer mix of the patient population. A large hospital will typically have multiple types of ICUs and stepdown units. It is the cardiac critical care units (CCUs) and the surgical intensive care units (SICUs) that are of the most potential value. The clinical opportunity stems from the concept of providing a continuum of care from OR to ICU. A good example is the service at Lutheran General Hospital in Park Ridge, Illinois. For years, a team of critical care certified anesthesiologists have provided effective coverage to critically ill patients passing from the OR into the unit.
The economics of ICU coverage hinges on three factors: the volume of patient encounters, the acuity of care provided as assessed on a case-by-case basis and the payer mix of the patient population. A large hospital will typically have multiple types of ICUs and stepdown units. It is the cardiac critical care units (CCUs) and the surgical intensive care units (SICUs) that are of the most potential value. The clinical opportunity stems from the concept of providing a continuum of care from OR to ICU. A good example is the service at Lutheran General Hospital in Park Ridge, Illinois. For years, a team of critical care certified anesthesiologists have provided effective coverage to critically ill patients passing from the OR into the unit.
With regard to the volume potential of an ICU practice, it is unlikely that the unit will generate levels of payment that even come close to what the same physicians could generate in the OR. Generating these payments would require more patients than come from the OR. Busy practices might see eight to 10 new patients per day in the ICU.
The revenue potential is determined by the combination of coding and payer mix. Since ICU services are paid based on a general medical fee schedule, the level of the code and the fee schedule from which the services will be paid can make a huge difference. For example, Code 99291 has a Medicare allowable in one region of $244.61, while the Blue Cross Blue Shield allowable is $263.81. The Medicaid allowable is only $84.
With regard to coding , the importance of clear and complete documentation cannot be overstated. Coders of ICU services review provider documentation for a variety of factors, including diagnosis, the details of the patient’s evaluation, and treatment and the amount of time spent face to face with the patient. Code 99291 covers the first 74 minutes of care in a given day. Code 99292 (CPT Code 99292 – critical care, evaluation and management of the critically ill or critically injured patient; each additional 30 minutes) is used for additional 30-minute increments.
There has been considerable focus in recent years on the use of Code 99291. Many a practice has had to review its documentation patterns after a careful audit when it was revealed that the necessary criteria were not being met. The financial implications of such a development can be significant, sometimes reducing the revenue potential by 60 percent, the payment difference between codes 99291 and 99233 (CPT Code 99233 – subsequent hospital care, per day, for the evaluation and management of a patient).
The ICU and Health Reform
 Anesthesiologists have lost interest in covering the ICU for many reasons. The lack of comparable revenue potential is just one. In many facilities, the ICU is the domain of surgeons or cardiologists and primary care physicians who have claimed responsibility for the patients. Often, the result of this evolution is a domain where standards of care and provider availability are somewhat the luck of the draw. To avoid this, some hospitals have hired intensivists for their ICUs, but turf wars persist.
Anesthesiologists have lost interest in covering the ICU for many reasons. The lack of comparable revenue potential is just one. In many facilities, the ICU is the domain of surgeons or cardiologists and primary care physicians who have claimed responsibility for the patients. Often, the result of this evolution is a domain where standards of care and provider availability are somewhat the luck of the draw. To avoid this, some hospitals have hired intensivists for their ICUs, but turf wars persist.
There are two types of ICUs: closed and open. In a closed ICU, the hospital has either contracted with or hired a staff of trained intensivists to manage all patients. In the open ICU, various providers, including cardiologists and surgeons, come and go as they manage “their patients.” The data suggests that the incidence of mortality is lower in closed units.
An anesthesia ICU solution in which one team of providers manages the patient through the entire continuum of surgical and postoperative care offers a more appropriate alternative. In most facilities, the introduction of such a model would represent a dramatic cultural change, and, yet, one that is probably more consistent with where reimbursement mechanisms are heading than where they are now. The current model reflects a fee-for-service environment, which fosters competition between providers for payment.
Although the recent Republican effort to replace Obamacare failed, other market changes, including the move to value-based payment through MACRA’s (Medicare Access and CHIP Reauthorization Act) Quality Payment Program (QPP), are likely to go forward. Most observers believe that bundled payment programs will be expanded. For one thing, Medicare is clearly focused on exploring ways to reduce the overall cost of cardiac care. It is also reasonable to assume that plans will also be developed to address all expensive surgical procedures that involve multiple specialties such as total joint replacements. Such arrangements will ultimately require reducing overlaps and coordinating providers involved in package rate negotiation and distribution.
 Anesthesia has an opportunity to pre-empt this process and position itself to be a player in the negotiation of a reasonable rate structure. The key point is that the era of fee-for-service medicine, in which providers get paid to perform services, irrespective of the outcome, is evolving into an era of cost reduction, where providers are incentivized to help drive down the cost of care.
Anesthesia has an opportunity to pre-empt this process and position itself to be a player in the negotiation of a reasonable rate structure. The key point is that the era of fee-for-service medicine, in which providers get paid to perform services, irrespective of the outcome, is evolving into an era of cost reduction, where providers are incentivized to help drive down the cost of care.
The same concepts are being explored on the quality side. The Merit-Based Incentive Program (MIPS) arm of the QPP includes a measure related to transfer of care to the ICU. Payment incentives could be developed to explore ways to better coordinate care between the OR and the ICU. It is not clear how this would work, but that might be the opportunity.
Conclusion
The concept of taking on responsibility for the ICU represents out-of-the-box thinking. It is a paradigm shift. It makes no sense if the objective is to enhance practice revenue by adding a new line of business. In fact, most coverage arrangements require hospital support. What it also speaks to is a desire to broaden the relationship with the facility in an effort to better align the anesthesia practice’s and hospital’s incentives. What it also speaks to is the future of hospital contracting in which anesthesia looks for ways to apply its core competencies in ways that better support hospital administration’s strategic and financial objectives. The critical next step will be finding a way to make such arrangements financially viable for all parties.
 Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.
Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.