Chronic Pain Management: An Overlooked Opportunity to Financially Partner with Your Hospital & Preserve Your Contract
Jerry Ippolito, MBA, MHSA
President, OR Efficiencies, LLC, Naples, FL
As anesthesiology’s private practice setting continues to change, the financial landscape appears more threatening than ever. More and more private practice groups are having to defend their longstanding hospital contracts to requests for proposals (RFPs). Relationships between anesthesia groups and their aligned hospitals, which have spanned decades, are being undermined by deteriorating medical practice and hospital finances. Hospitals are issuing RFPs and subsequently awarding contracts to national anesthesia practice management companies—akin to Home Depot coming into the community and forcing out the Ace Hardware store. In order to survive and effectively defend their contracts, private practice anesthesiology groups must strategically refocus and realign their relationships with partner hospitals. Anesthesiology groups must go into the hospital board room bringing value and presenting opportunities to assist hospitals to increase income— NOT simply ask for a larger stipend! An effective chronic pain management program is driven by anesthesiology, can add millions to a hospital’s bottomline and can easily offset anesthesiology stipends required to support the traditional hospital anesthesia program.
In the frequently heard and paraphrased words of one of our esteemed colleagues:
“Medicine is a Science; Surgery, Anesthesiology, and Nursing are disciplines; Healthcare is a Business” – Amr Abouleish, MD (UTMB)
As a growing number of hospitals face negative profit margins, and the true financial ramifications of the Affordable Care Act are yet unrealized, hospitals’ finance leaders are examining ways to expand revenue generating services. An effectively developed and comprehensive chronic pain management program can contribute millions of dollars to a hospital’s bottom-line revenue.
The Institute of Medicine reported that chronic pain affects 116 million adults in the U.S. The American Academy of Pain Medicine has indicated that the financial impact of chronic pain on the US economy is greater than diabetes, heart disease and cancer combined. As the population ages, yet remains physically active, the demand for pain management services will continue to grow. Many hospital administrators consider pain management a poor source of revenue. In fact, however, leading hospitals have found that comprehensive pain management programs, that are strategically positioned, energetically developed and well run can attain strong profitability within a relatively short time. Specifically, these programs can:
- Contribute large amounts to the hospital’s bottom line. In a mature practice employing one pain physician, annual revenue from facility fees alone can range from $2.5 million to $3 million. Revenue from professional fees represents another $1 million. Overall program profitability can and will range from three to four times the physician’s income.
- Generate sizable ancillary revenue from hospital services that support the pain practice, such as physical therapy, radiology, lab and behavioral medicine.
- Establish a new source of referrals for surgical services—such as orthopedic surgery and neurosurgery—that are independent of traditional referrals from primary care physicians and can generate additional OR revenue.
- Support key relationships with surgeons, anesthesiologists and other physicians.
While these financial results are within reach for most organizations, creating a strong pain management center takes careful planning and effective execution. Eight key characteristics are shared by the most effective and profitable programs:
- Demographic and Market Opportunity: Typically a population of 25,000 nongovernment-insured patients is required to support a successful one physician chronic pain practice. This number can vary depending on payer mix and payer contracts. In many markets, there is an opportunity to absorb market share beyond existing need. Survey primary care physicians and surgeons (especially orthopedic surgeons) on where they refer patients requiring pain management. A hospital-based program that offers comprehensive pain services has an opportunity for competitive differentiation and growth.
- Strategic Location: Pain management has a strong “consumer” dynamic, so convenience and ease of access are important. Ideally, a pain management program will be located in the hospital’s outpatient department or ambulatory surgery unit, accessed by an entrance separate from the main hospital entry.
- Reimbursement: In most instances, a hospital-based fee schedule provides the highest level of reimbursement. However, locating the pain center on the hospital campus is not the only option. According to Centers for Medicare & Medicaid Services (CMS) guidelines, an offsite facility can be reimbursed under the hospital- based fee schedule if it is within 35 miles of the hospital proper and meets other requirements that usually include the center operating under the hospital’s license. A pain center could also be located in a non-hospital based ambulatory surgery center (ASC). Planners should carefully analyze reimbursement under an ASC fee schedule and verify the impact on revenue. It needs to be recognized that CMS is beginning to review their criteria for hospital-based reimbursement programs. CMS has realized that the existing criteria are not an incentive to contain/reduce costs, nor an incentive to move patient care services to lower cost, non-hospital, ambulatory settings.
Anesthesiologists may be inclined to develop a private office-based center that is independent of the hospital. There are two significant reasons to put that idea aside: - Office-based services do not receive a facility fee but only a small site-of-service differential (SSD) which is a premium reimbursement payment for professional service fees. This financial comparison is demonstrated in the example provided under the heading “Hospital-Based Versus Office-Based Reimbursement” on page 13.
- Developing the center based location, and denying the hospital the opportunity to generate additional revenue (even worse, potentially diminishing existing hospital revenue sources) will only contribute to the deterioration of your group’s relationship with the hospital. This will NOT be a value-add for your group.
- Comprehensive Scope of Services to Optimize Reimbursement: A full spectrum approach to pain management is not only critical to connecting with patients, but it is also important to the financial success of a pain management program. Procedures provide the greatest reimbursement for both the physician and the facility. Common pain management procedures include:
- Nerve blocks
- Trigger point injections
- Epidural injections
- Fluoroscopy procedures
- Stimulator insertions
- Patients’ evaluation and management (E&M) visits reimburse both the professional and facility fee at reduced or nominal levels. The pain physician receives nominal reimbursement for E&M services and the facility fee, which the hospital benefits from, is reduced or potentially denied unless visits are conducted by a licensed professional such as a nurse (RN), a physician assistants (PA) or a certified nurse practitioner (CNP). Typically, in instances where the non-physician professional cannot bill independently (e.g., RNs) that professional must be employed by the facility (not the physician/anesthesia practice) in order for the facility fee to be paid. Moreover, even in states where PAs and CNPs can bill independently, some payers will deny payments for these professionals’ E&M services. These reimbursement nuances for E&M visits simply exemplify the reimbursement variability involved in collecting for pain management services. Hospitals and anesthesia practices must fully understand and negotiate pain management services payer contracts on a payer-by-payer basis. Where payer contracts are not specifically negotiated, payers can and will pay what they want to, and payers believe it is their duty to deny claims unless specifically provided for in contracts.
- Sizable hospital revenue can be generated from the referral of patients to support services that are an integral part of a comprehensive program, such as:
- Physical therapy for patients suffering from joint pain,
- Nutritional counseling for overweight patients with back pain and,
- Behavioral counseling for patients who require lifestyle changes to progress and sustain relief. Tracking referrals to these services helps validate the ROI of the pain program.
- Well-trained, Strongly-motivated Physicians: To provide comprehensive services, an anesthesiologybased pain program should be led by an anesthesiologist who is fellowship- trained in pain medicine. The most successful pain centers are built around an anesthesiologist who is boarded in both anesthesiology and pain management. It is also important that the anesthesiologist have an entrepreneurial attitude, a strong work ethic and a financial incentive because practice volume drives hospital and program revenue. Successful programs use a productivity- based compensation plan. One possibility is to offer a guaranteed base salary during the first year, with compensation increasing to a higher incremental percent of collections in year two and three.
- Focused Marketing: Use a two-pronged marketing approach to target patients and referring physicians. Patient marketing efforts should focus on active baby boomers and position pain management as “a medical alternative to surgery.” The pain physician needs to make personal visits to referring physicians to introduce him or herself and market the practice. The pain physician can also develop referrals through lectures to the hospital medical staff and informational luncheons organized for community physicians and their office personnel.
- Efficiency and Optimized Throughput: The pain physician should focus his or her time on performing procedures and consulting with new patients. With the exception of some longer procedures, a pain physician should be able to see one patient every 15 minutes. In a mature practice, a PA will be able to handle most follow up E&M visits. These volume and throughput requirements call for an enhanced office layout. Three exam and procedure rooms are typically not enough. Most programs require five or six rooms to maintain patient flow for both the physician and the PA.
- Effective Billing and Collections: The first important step is to negotiate satisfactory contract rates for key procedures with your organization’s top nongovernment payers. Absent contract rates, payers generally reimburse pain services at the lowest possible level and as previously indicated, payers believe it is their job to deny claims. Further, it is paramount for both the anesthesia group and hospitals to engage professionals highly experienced and effective in the discipline of chronic pain billing as:
- Optimized billing and collections are critical to a center’s financial success, and
- Chronic pain programs continue to be highly scrutinized by both payers and the OIG with regard to billing fraud.
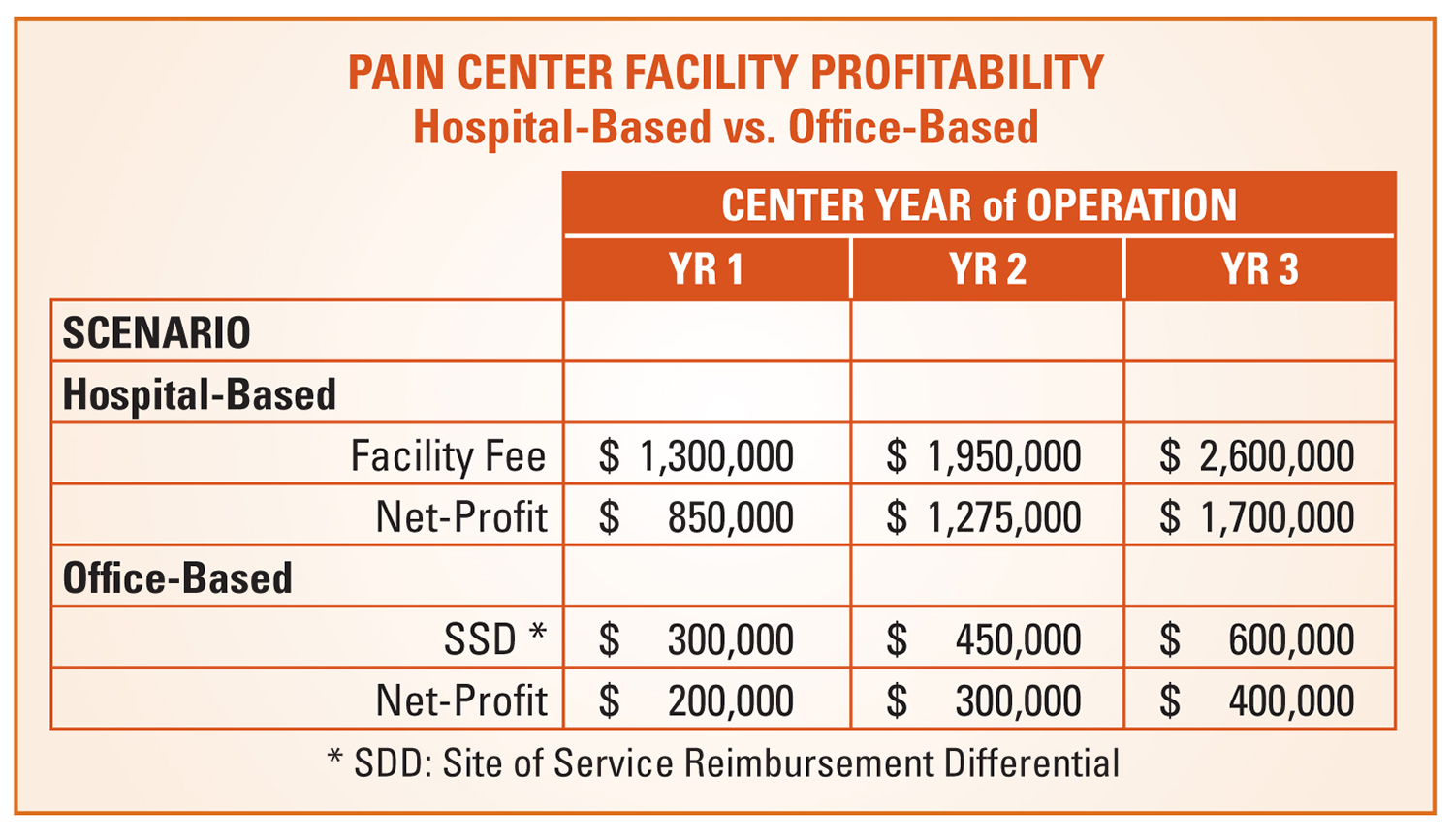
Hospital-Based Versus Office-Based Reimbursement
 The example in the table above indicates both the level of a pain program’s potential profitability and the differences of profitability depending on the center’s facility base. The example summarizes a pro-forma developed for a major southeastern health system’s chronic pain management program. Hospitals have found that comprehensive pain management programs that are strategically located, energetically developed and well run can attain strong profitability within a two to three year period.
The example in the table above indicates both the level of a pain program’s potential profitability and the differences of profitability depending on the center’s facility base. The example summarizes a pro-forma developed for a major southeastern health system’s chronic pain management program. Hospitals have found that comprehensive pain management programs that are strategically located, energetically developed and well run can attain strong profitability within a two to three year period.
Financial projections were based on the following assumptions:
- A single anesthesiologist pain practice supported by a PA;
- Payer-mix skewed towards “government- pay” at below average reimbursement levels due to the prevalence of military health plans in the market (most successful programs will demonstrate even higher levels of profitability);
- Professional revenue and physician compensation are the same under both scenarios, and
- Profitability does not reflect any allocations of indirect costs, or additional revenue, from ancillary service volume (radiology, physical therapy, etc.) and surgical referrals.
Summary:
We are in an anesthesia environment where individual practices find it increasingly necessary to ask hospitals for higher and higher financial stipends as a result of anesthesia program deficits. These deficits can, and do, easily approach one million dollars or more. An aggressive and proactive anesthesiology group, that is sincerely interested in financially partnering with its aligned hospital, can offset anesthesia program deficits by assisting hospitals to develop new programs and additional sources of revenue. Development of an effective chronic pain management program is only one of these opportunities.
 Jerry Ippolito, MBA, MHSA is President of OR Efficiencies, LLC, Naples, FL. OR Efficiencies, LLC is a management consulting firm specializing in assisting hospitals and ASCs to improve their perioperative services and anesthesiology programs. Mr. Ippolito can be reached at ippolito.orefficiencies@gmail.com.
Jerry Ippolito, MBA, MHSA is President of OR Efficiencies, LLC, Naples, FL. OR Efficiencies, LLC is a management consulting firm specializing in assisting hospitals and ASCs to improve their perioperative services and anesthesiology programs. Mr. Ippolito can be reached at ippolito.orefficiencies@gmail.com.