It’s Update Time! 2015 Coding and Medicare Fee Schedule Updates for Anesthesia and Pain Medicine
Joette Derricks, CPC, CHC, CMPE, CSSGB
Vice President of Regulatory Affairs & Research, ABC
The American Medical Association 2015 CPT® Codebook is now available. It contains 9,951 total Current Procedural Terminology (CPT) codes and more than 500 code changes: 266 new, 147 deleted and 129 revised codes. The good news for anesthesia providers and coders is that the only change to the anesthesia code section (00100-01999) is the deletion of three codes, all due to low utilization. The deleted codes are:
- 00452 Anesthesia for procedures on clavicle and scapula; radical surgery
- 00622 Anesthesia for procedures on thoracic spine and cord; thoracolumbar sympathectomy
- 00634 Anesthesia for procedures in lumbar region; chemonucleolysis
The bulk of the coding changes for 2015 fall within the surgical section and the impact, if any, regarding most of these changes will become apparent upon the release of the American Society of Anesthesiologists (ASA) 2015 A Guide for Surgery/Anesthesia CPT® Codes 2015 Crosswalk (not available at press time). Since many of these surgical coding changes involve changes to the Centers for Medicare and Medicaid Services (CMS) Medicare Physician Fee Schedule (MPFS) for 2015, due to bundling of services, or revisions of the relative value units (RVUs), anesthesiologists will see some new and revised crosswalks in 2015.

Overall, the AMA/Specialty Society Relative Value Update Committee (RUC) has examined nearly 1,800 potentially misvalued medical services accounting for $39 billion in Medicare spending. To date, the RUC has recommended reductions in work RVUs and code deletions for 945 services, allowing for the redistribution of more than $3.5 billion. Another 218 procedures are still under review. The RUC review of specific procedures is based on fifteen different screening criteria. Examples of screening criteria are Medicare’s High Volume Growth Screen, where Medicare utilization for a specific code increased by at least 100 percent from 2006 to 2011, and when two CPT codes are reported together on the same day of service by the same provider of service more than 75 percent of the time. The RUC revaluation of codes may directly or indirectly impact physicians’ reimbursement.
New Transesophageal Echocardiography Code in 2015
One new CPT code of potential interest to anesthesiologists who are qualified to perform interventional Transesophageal Echocardiography (TEE) is CPT code 93355. The code description reads:
Echocardiography, transesophageal (TEE) for guidance of a transcatheter intracardiac or great vessel(s) structural intervention(s) (e.g., TAVR, transcatheter pulmonary valve replacement, mitral value repair, paravalvular regurgitation repair, left atrial appendage occlusion/closure, ventricular septal defect closure) (peri-and intraprocedural), real-time image acquisition and documentation, guidance with quantitative measurements, probe manipulation, interpretation and report, including diagnostic transesophageal echocardiography and, when performed, administration of ultrasound contrast, Doppler, color flow, and 3D.
Code 93355 is reported once per intervention and only by an individual who is not performing the interventional procedure. Note that code 93355 includes the work of:
- Passing the endoscopic ultrasound transducer through the mouth into the esophagus, when performed by the individual doing the TEE;
- Diagnostic TEE and ongoing manipulation of the transducer to guide sizing and/or placement of implants, determination of adequacy of the intervention, and assessment for potential complications; and
- Real-time image acquisition, measurements and interpretation of image(s), documentation of completion of the intervention and final written report.
Code 93355 cannot be reported in conjunction with any other TEE, Doppler, color flow or 3-D image reconstruction codes. In the final rule, CPT 93355 was assigned 6.38 RVUs which yields a national MPFS amount of $228.41.
Waiver of Co-insurance for Anesthesia Provided for Screening Colonoscopies
Another reporting and payment change of interest to anesthesiologists is the waiver of the patient co-insurance and deductible when anesthesia is provided for screening colonoscopies.
Effective January 1, 2015, the separately payable anesthesia service done in conjunction with a colorectal cancer screening test should be billed with modifier 33 on the same claim line as the anesthesia service. If the test began as a colorectal cancer screening test but resulted in unplanned tissue removal, e.g., a colonoscopy with polyp removal, etc., the anesthesia professional should report a PT modifier on the claim line rather than the 33 modifier. In order to report the services correctly, anesthesiologists providing anesthesia for colonoscopies will need to adequately document whether the service was a colorectal cancer screening test or a colorectal cancer screening test that was converted to a diagnostic or therapeutic procedure. Anesthesiologists may want to verify with the gastroenterologist the final CPT code used for all colonoscopies that they provide anesthesia services.
Medicare has two Healthcare Common Procedure Coding System (HCPCS)/CPT codes for colon cancer screening colonoscopies to distinguish whether the patient is at high risk or not. A patient is considered to be at high risk for colorectal cancer if they have any of the following:
- A close relative (sibling, parent, or child) who has had colorectal cancer or an adenomatous polyp; •• A family history of adenomatous polyposis;
- A family history of hereditary nonpolyposis colorectal cancer;
- A personal history of adenomatous polyps;
- A personal history of colorectal cancer;
- A personal history of inflammatory bowel disease, including Crohn's Disease and ulcerative colitis.
For the colorectal screening cancer test, the gastroenterologist has the choice of two G codes for Medicare patients and, as indicated in Table 1, both G codes would require the use of modifier 33 with the ASA code 00810 in order to have Medicare waive the co-insurance and deductible amounts. If modifier 33 is not reported, Medicare will reimburse the claim at 80 percent of the fee and the anesthesia provider will be required to bill the secondary insurer, or patient, as applicable, for the co-insurance.
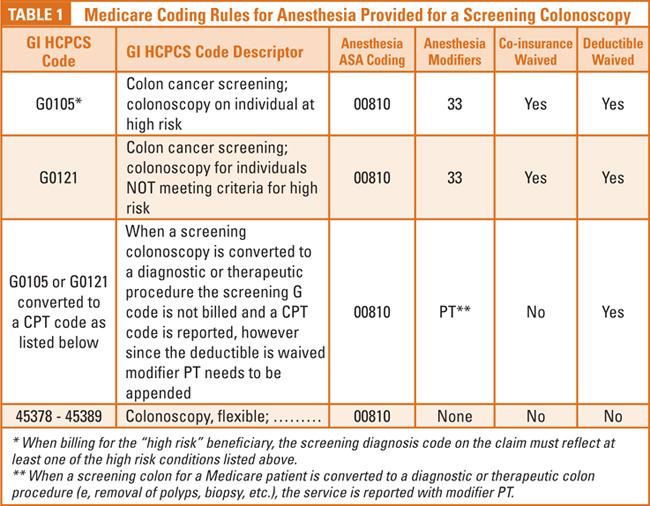
When a screening colon cancer colonoscopy is performed and the physician finds a problem (e.g., polyps, foreign object, bleeding, etc.), the procedure is no longer considered “screening.” In place of using the screening G codes, the GI procedure would be reported with the CPT code for a diagnostic or therapeutic colonoscopy (CPT 45378-45398) with modifier PT. When modifier PT is used the deductible is still waived but the co-insurance is not. Table 1 shows the coding rules applicable to the Medicare regulation.
In the discussion accompanying the Final Rule on the MPFS for 2015, CMS stated that the change regarding the waiver of the co-insurance for screening colorectal cancer testing is a national policy and takes precedence over any local coverage policy that limits Medicare coverage for anesthesia services furnished during a screening colonoscopy by an anesthesia professional. However, if the screening colonoscopy is converted to a diagnostic or therapeutic colon procedure, all Medicare medical necessity guidelines will remain unaffected.
Finally, in regards to colonoscopies, it is important for anesthesiologists to know that many of the lower gastrointestinal (GI) CPT codes reported by the gastroenterologist have been revised by the AMA in 2015. In addition, several new lower GI CPT codes have been added (e.g, Colonoscopy through stoma and Ileoscopy through stoma). For the 2015 reporting year, CMS has established G codes to mirror the 2014 CPT codes that were deleted in 2015. As a result, if the patient has Medicare (Fee for Service or Medicare Advantage), gastroenterologists have a complicated billing situation. That is to say:
- If the code has not changed from 2014 to 2015 or is new in 2015, physicians report the CPT code
- If the code has changed from 2014 to 2015, physicians report the G code for Medicare patient
- If the facility (ASC, hospital outpatient, etc.) is billing Medicare, the 2015 CPT code is used regardless of whether the code is new or has not changed
Of course, if it is a commercial, Medicaid, Exchange, or other payer, the physician should report the 2015 CPT code unless the payer advises them otherwise. While lower GI endoscopic billing is complicated for the GI physician in 2015, the anesthesiologist services would all fall under the ASA/CPT code 00810. The only additional information required is specific to the colorectal cancer screening codes and the use of modifier 33 or PT as discussed above.
Potential Sustainable Growth Rate Impact
The last CMS MPFS issue of concern to anesthesiologists is the payment rate effective for services furnished on or after January 1, 2015 and on or after March 1, 2015. Current law requires that physician payments be reduced by 21.2 percent from the 2014 rates. In prior years, Congress has taken action to avert a large reduction in the MPFS rates before they went into effect. The Protecting Access to Medicare Act of 2014 established a zero percent change in payment rates from January 1, 2015 through March 1, 2015. Therefore, the proposed reduction will not be implemented prior to March 1, 2015, allowing Congress time to address the proposed payment rate and consider a permanent change to the Sustainable Growth Rate (SGR) methodology. The Final Rule also addresses changes to malpractice RVUs and Geographic Practice Cost Indices (GPCIs), both of which may impact physician reimbursements.
Pain Medicine
Pain medicine practices are in for an overhaul in 2015. There will be several important Medicare changes including drug testing, epidural steroid injections (ESI), PQRS and a multitude of revised CPT codes/procedures.

Epidural Steroid Injection Reimbursement
Of particular interest to pain medicine physicians are changes to the payment for ESI. Payments for ESIs were significantly reduced in the 2014 MPFS, provoking an outcry from the pain medicine community. As a result, CMS will raise payments for 2015 using prior resource inputs pending further review and recommendations from the AMA RUC. CMS will not, however, pay separately for image guidance in 2015. It is our understanding that pain medicine organizations have already begun looking at potential CPT code and other changes to ESI services and will work with the AMA RUC to provide additional feedback to CMS. Table 2 compares the MFPS national reimbursement for epidurals in 2013, 2014 and 2015.

Bundling of Ultrasound with Joint Injections
In addition to the CPT codes above, pain medicine providers may be interested in the bundling of ultrasound with the following procedures in 2015 (as listed in Table 3). Again, the payment amounts reflect MPFS national reimbursement levels.
New Codes for Transversus Abdominis Plane Blocks
New codes for post-op pain blocks are on the way. Starting in 2015, anesthesia providers will report transversus abdominis plane (TAP) blocks with one of four codes depending on whether the service is performed by injection or continuous infusion and unilaterally or bilaterally. The codes and their descriptors are listed in Table 4.

Total Rewrite of Drug Screening Codes and Guidelines
The CPT 2015 manual revamped the entire code set for drug screens and issued new guidelines and definitions. Instead of differentiating testing procedures based on qualitative or quantitative methodology, the new reporting mechanism differentiates procedures according to whether they are:
- Presumptive (used to identify possible use or non-use of a drug or drug class);
- Definitive (qualitative or quantitative methods that identify possible drug use or non-use and identify the specific drugs and associated metabolites); or
- Therapeutic Drug Assays (quantitative procedures performed to monitor clinical response to a known, prescribed medication).
The updated reporting mechanism has been designed to address the following:
- Ability to be easily modified for future changes and technological advances;
- Identification of updated clinical settings, and
- Identification of “sources” for specimen(s).
The Presumptive Drug Class Screening section includes Guidelines for the Presumptive Drug Class Screening section, Drug Class List A (which itemizes commonly assayed drugs within the listing) and Drug Class List B (which itemizes assays that require more resources than Class A). This section also includes guidelines that explain the intended use for the listing and the codes. Five new codes have been developed to identify presumptive testing with introductory guidelines explaining the intent for use of these codes.
Definitive Drug Testing includes fifty-nine new definitive drug testing codes. The codes are arranged by drug classes. Refer to the Definitive Drug Classes Listing table for drugs and metabolites included in each definitive drug class.
Based on the latest information from Medicare, next year pain management physicians may be required to use the entirely new sets of CPT codes for commercial payers and Medicare G codes to report qualitative and quantitative drug screens. At the AMA-CPT 2015 Symposium held in November 2014, CMS officials presented numerous G codes that were created for 2015. CMS’ overall position is that when the timing of a CPT code creation precludes adequate timeframe for CMS consideration of comments and RUC valuation, they will implement or default to the use of G code(s). In the 2015 MPFS Final Rule, CMS indicated they would also create a G code if the revisions and or deletions to AMA-CPT may affect the code RVU value. In addition, they would add G code(s) when AMA-CPT separated a CPT code into two CPT codes.
In the Final Medicare Rule for 2015, CMS said, “These codes represent various drug screening codes, many of which are specific to individual drug testing. While we appreciate the recommendations for these tests, we are concerned about the potential for overpayment when billing for each individual drug test rather than a single code that pays the same regardless of the number of drugs that are being tested for. Therefore, it is our recommendation to delay pricing for these codes at this time, until further information and education is obtained.”
As of press time, CMS had not yet released the clinical lab fee schedule for 2015. Stay tuned for additional updates as we learn more on how Medicare and other payers plan to respond to these extensive changes.

Joette Derricks, CPC, CHC, CMPE, CSSGB serves as Vice President of Regulatory Affairs and Research for ABC. She has 30+ years of healthcare financial management and business experience. She is a member of MGMA, HCCA, AAPC and other associations and a regular speaker at practice management conferences. She can be reached at Joette.Derricks@AnesthesiaLLC.com.