Puttin’ on AIRS
Richard P. Dutton, MD, MBA, Executive Director, Anesthesia Quality Institute, Park Ridge, IL
The Anesthesia Quality Institute was founded to create and maintain the National Anesthesia Clinical Outcomes Registry (NACOR). This project is now two and a half years old and more than 135 practices, including nine ABC clients, have contributed more than 5 million records to this “every case, every day” registry. Participants have online access to the NACOR Reporting Server, where they can see continually updated summaries of their practice performance and aggregated national benchmarks. This information, and the ability to slice and dice it to examine subsets of interest, is an important business and quality management tool. After all, what can’t be measured can’t be improved.

“Say you inadvertently gave phenyle-phrine instead of ketorolac at the end of a case. The patient’s blood pressure went to 250/130 for a few minutes, but nothing bad happened. How would your report this event?”
Immature practice response: “Did anyone notice? No harm, no foul!”
Mature practice response: “I’ll record it in our incident system, and discuss it with our QM physician. Maybe other people have had the same problem.”
In a truly mature system there are secondary methods for collecting these events. An online or AIMS-based quality-capture form is completed for each case in very well-wired practices (ABC partner ePreop™ offers such a system). Another approach is to electronically search for unusual occurrences such as sudden wide swings in blood pressure or heart rate, use of naloxone or epinephrine, or unusually short or long procedures.

The presentation itself should focus on the key anesthesia decision points, such as what preoperative tests to order, what type of anesthesia to offer, and whether to proceed with a difficult case or cancel it. When presenting to a group, it makes sense to stop at these moments and ask “What would you do?” In large and well-wired practices this can be facilitated by use of an audience response system. The results will tend to provoke conversation, which in turn will reveal two seldom acknowledged aspects of clinical anesthesia: 1) There are many ways to skin a cat, and 2) Even if they’re in the next room, we have no idea what our colleagues are doing. A well-conducted M&M system will illustrate the acceptable variability in clinical practice that occursevery day, and support the discussion with brief references to the current evidence-based scientific literature. A second goal of the M&M discussion is to identify system issues that may have contributed to the incident, and solicit suggestions for how to improve them. Examples might include “put the ketorolac in a different drawer from the phenylephrine,” “buy enough video laryngoscopes,” and “increase anesthesia staffing at lunch time.” Aside from generating good ideas, the documentation from an M&M near miss conference might be valuable ammunition when requesting resources in the Executive Office.
A National Anesthesia M&M System: AIRS
 Recognizing the importance of incident-based QM at the ground level, the AQI Board of Directors made an early goal of developing such a system that could operate nationally. Fueling this request was the observation that other disciplines were already doing this (e.g. aviation, mountain climbing), and that similar systems were operated by anesthesia associations in other countries. The Anesthesia Incident Reporting System (AIRS) was born after 6 months of legal research, consultation with dozens of experts in anesthesia quality management and safety, and detailed exploration of technical possibilities. Reporting to AIRS is open to any provider with access to the Internet, by connecting to the following website: www.aqiairs.org. The report form is straightforward and easy to use, and anyone reading this article is welcome to go play around with it now. (There is a button on the last page that asks “is this a real case or a test?” If you’re experimenting, please don’t mark this as a real case!)
Recognizing the importance of incident-based QM at the ground level, the AQI Board of Directors made an early goal of developing such a system that could operate nationally. Fueling this request was the observation that other disciplines were already doing this (e.g. aviation, mountain climbing), and that similar systems were operated by anesthesia associations in other countries. The Anesthesia Incident Reporting System (AIRS) was born after 6 months of legal research, consultation with dozens of experts in anesthesia quality management and safety, and detailed exploration of technical possibilities. Reporting to AIRS is open to any provider with access to the Internet, by connecting to the following website: www.aqiairs.org. The report form is straightforward and easy to use, and anyone reading this article is welcome to go play around with it now. (There is a button on the last page that asks “is this a real case or a test?” If you’re experimenting, please don’t mark this as a real case!)
AIRS is intended for “Any unintended event related to anesthesia or pain management with the significant potential for patient harm.” Examples include unusual manifestations of patient disease, unusual reaction to medications, abnormal function of technology, drug shortages, and facility system failures. All reports to AIRS are absolutely confidential. They are protected from legal discovery by federal law, by virtue of AQI’s status as a Patient Safety Organization. Transmission to AIRS is by secure,encrypted communication protocols, and the AIRS database itself is secured behind a firewall at the AQI. Reports may be entered as confidential (the reporter’s email and practice information is recorded) or completely anonymous. Confidential reporting allows for further discussion about interesting cases, and the ability to enter follow-up information or patient outcome as it is develops.
AIRS is open to both hits—incidents which cause an injury—and near misses. The reporting form solicits some basic structured data (patient age and BMI, type of surgical procedure, classification of the incident by body system and cause) as well as a free text description of the event. The reporter is asked to opine about the preventability of the event and lessons learned. The goal is for reporting to take less than 5 minutes for any case. Compatibility with existing incident reporting systems and local requirements is achieved by having an “email echo” feature that will send a copy of the case report to any desired third party, such as the practice or hospital QM person. Some AQI participant practices are exploring the use of AIRS on a system-wide basis, to capture all their anesthesia incidents. AQI will support this use by providing practice-specific summaries of the cases that are submitted.
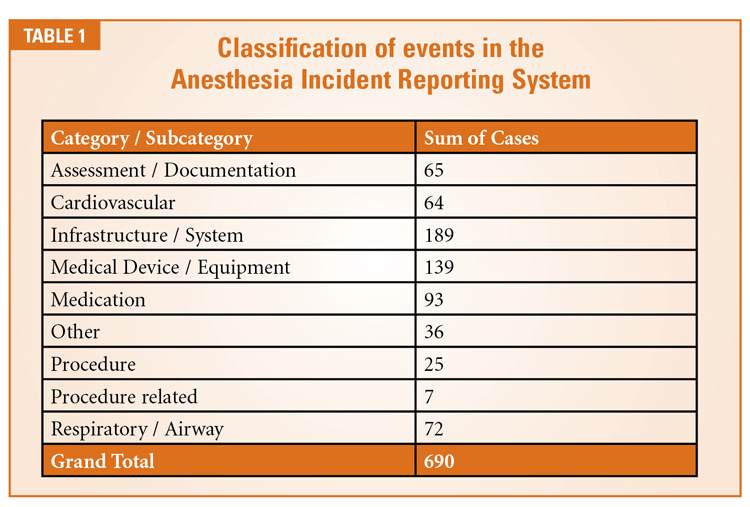 AIRS opened to the public on October 1, 2011. Since that time it has garnered nearly 600 reports. Table 1 shows the broad classifications of submitted events (some cases fit in more than one class). Most of the reported events occurred in the OR, but incidents have also been captured from the ICU, obstetric unit, PACU, pain clinic and general medical ward. Incidents are reported most commonly in ASA-3 patients, and about three-quarters of the incidents were deemed preventable by the reporter.
AIRS opened to the public on October 1, 2011. Since that time it has garnered nearly 600 reports. Table 1 shows the broad classifications of submitted events (some cases fit in more than one class). Most of the reported events occurred in the OR, but incidents have also been captured from the ICU, obstetric unit, PACU, pain clinic and general medical ward. Incidents are reported most commonly in ASA-3 patients, and about three-quarters of the incidents were deemed preventable by the reporter.
All AIRS reports are confidentially reviewed by members of the AIRS Steering Committee (Table 2), for two purposes. First, any trends in new events are noted. These may be relatively trivial— such as the repeated reporting of noninvasive blood pressure monitors that spontaneously reverted from automatic to manual mode, leaving a gap in monitoring—but the fact that they recur suggests the need for systematic improvement. AQI has shared the existence of these events with the Anesthesia Patient Safety Foundation and the Society for Technology in Anesthesia, who are working with the manufacturers to find a solution. The AIRS Committee also looks for unique cases with exceptional teaching value. These are abstracted and fictionalized, then summarized in a series of case reports published on a monthly basis in the ASA Newsletter. These cases have been appearing since October, 2011 (all are available for review online at http://www.aqihq.org/casereportsandstats.aspx). Each report describes the incident itself, the pathophysiology of the event, the system factors that may have contributed, and the key points for provider education. For example, the phenylephrine for ketorolac event described above is based on a real occurrence submitted to AIRS, and was the subject of the January, 2012, AIRS Case Report in the Newsletter.
 AIRS: The Future
AIRS: The Future
 AIRS: The Future
AIRS: The FutureWith basic infrastructure now established, the AQI will leverage AIRS in a number of ways. First, we will promote it at every opportunity, until its existence and purpose are as ingrained in the minds of practicing anesthesiologists as the Malignant Hyperthermia Hotline. (Any provider who would like to receive free magnets or stickers with the AIRS web address can contact j.mlodoch@asahq.org.) Second, we will continue to select and publish interesting and educational cases—the August ASA Newsletter will include an AIRS case resulting from a little known but life-threatening complication of a very common anesthesia procedure. Third, we will continue to work on the AIRS reporting software to make it as specialty specific, but easy to use, as we possibly can. And finally, we will work with AQI participant practices to build fluid two-way communications based on AIRS that facilitate both local analysis of anesthesia events and national aggregation and reporting. If you haven’t visited the AIRS website yet, you can check it out now at http://www.aqihq.org/airsIntro.aspx. My colleagues at AQI and I hope to see you there soon.
 Richard P. Dutton, MD, MBA is Visiting Professor of Anesthesiology, University of Maryland School of Medicine and AQI Executive Director. To contact Dr. Dutton or the AQI, visit www.aqihq.org.
Richard P. Dutton, MD, MBA is Visiting Professor of Anesthesiology, University of Maryland School of Medicine and AQI Executive Director. To contact Dr. Dutton or the AQI, visit www.aqihq.org.