This tag contains 2 private blog which isn't listed here.
 Part I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations.
Part I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations.
3800 Hits
 Noah Rosenberg, M.D.Resident, Department of Family & Community Medicine, University of Massachusetts Memorial Medical Center, Worcester, MA
Fred E. Shapiro, D.O.Assistant Professor of Anesthesia, Harvard Medical School, Boston, ISOBS Founder
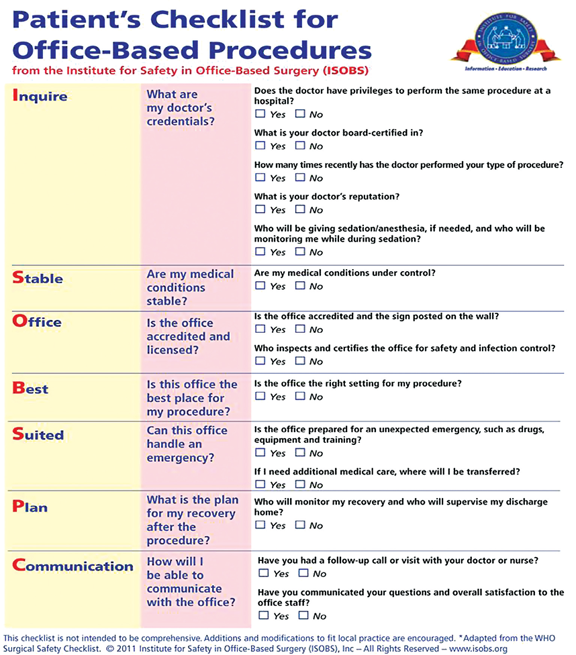
The Institute for Safety in Office-Based Surgery (ISOBS), an independent, non-profit 501(c)(3) organization, has developed a safety checklist for use in the office-based setting. A recent study to be published in the journal ePlastydemonstrated a more than 75% reduction in the number of surgical complications with use of the ISOBS Safety Checklist (see below for citation). While this positive effect on surgical complications validates much of the data already collected in the inpatient setting, it also clearly emphasizes the need for a tailored patient safety approach to the office-based setting. For that reason, ISOBS has developed a second checklist for use by patients to engage them in office-based surgical safety.
The ISOBS Patient Checklist (ISOBS PC) contains a number of questions...
Noah Rosenberg, M.D.Resident, Department of Family & Community Medicine, University of Massachusetts Memorial Medical Center, Worcester, MA
Fred E. Shapiro, D.O.Assistant Professor of Anesthesia, Harvard Medical School, Boston, ISOBS Founder
The Institute for Safety in Office-Based Surgery (ISOBS), an independent, non-profit 501(c)(3) organization, has developed a safety checklist for use in the office-based setting. A recent study to be published in the journal ePlastydemonstrated a more than 75% reduction in the number of surgical complications with use of the ISOBS Safety Checklist (see below for citation). While this positive effect on surgical complications validates much of the data already collected in the inpatient setting, it also clearly emphasizes the need for a tailored patient safety approach to the office-based setting. For that reason, ISOBS has developed a second checklist for use by patients to engage them in office-based surgical safety.
The ISOBS Patient Checklist (ISOBS PC) contains a number of questions...
5036 Hits
 The Anesthesia Quality Institute (AQI) is a non-profit corporation created to improve outcomes in anesthesia, based on aggregating, analyzing and reporting electronic data. Over the past three years AQI has recruited more than 220 anesthesia practices, from 44 states, to contribute data to the National Anesthesia Clinical Outcomes Registry (NACOR). The aggregate data has provided a unique and valuable perspective on the specialty of anesthesiology: What we do, what we know, and how we do it. At the same time, a picture is emerging of the other side of our national practice: What we don’t know and what we don’t do.
The widest performance gap in anesthesia today is our collective lack of insight regarding outcomes of the care we provide. Even among the participating groups in NACOR—a self-selected ‘choir’ of early adapters—fewer than 1 in 5 have the infrastructure to recognize and respond to the following event:
Mrs. Smith,...
The Anesthesia Quality Institute (AQI) is a non-profit corporation created to improve outcomes in anesthesia, based on aggregating, analyzing and reporting electronic data. Over the past three years AQI has recruited more than 220 anesthesia practices, from 44 states, to contribute data to the National Anesthesia Clinical Outcomes Registry (NACOR). The aggregate data has provided a unique and valuable perspective on the specialty of anesthesiology: What we do, what we know, and how we do it. At the same time, a picture is emerging of the other side of our national practice: What we don’t know and what we don’t do.
The widest performance gap in anesthesia today is our collective lack of insight regarding outcomes of the care we provide. Even among the participating groups in NACOR—a self-selected ‘choir’ of early adapters—fewer than 1 in 5 have the infrastructure to recognize and respond to the following event:
Mrs. Smith,...
4736 Hits
 Christopher Ryan, Esq. Giarmarco, Mullins & Horton, P.C., Troy, MI
Neda M. Ryan, Esq. Clark Hill, PLC, Birmingham, MI
Reporting post-operative pain management procedures often gives rise to questions, especially toward the beginning of the new year when the Centers for Medicare and Medicaid Services (CMS) issues its National Correct Coding Initiative (NCCI) edits. Historically, epidurals and blocks that are placed pre-operatively for the purpose of managing post-operative pain have been, and still are, separately reportable and not bundled into the anesthesia service itself. The exception to this general rule is when the epidural or block is the anesthetic itself. While CMS has not called for significant changes in 2013, anesthesia providers should, nevertheless, be aware of new post-operative pain management coding changes taking effect January 1, 2013.
NCCI Edits
The NCCI edits for 2013 provide, in part, that certain post-operative pain management procedures may only be separately reportable with...
Christopher Ryan, Esq. Giarmarco, Mullins & Horton, P.C., Troy, MI
Neda M. Ryan, Esq. Clark Hill, PLC, Birmingham, MI
Reporting post-operative pain management procedures often gives rise to questions, especially toward the beginning of the new year when the Centers for Medicare and Medicaid Services (CMS) issues its National Correct Coding Initiative (NCCI) edits. Historically, epidurals and blocks that are placed pre-operatively for the purpose of managing post-operative pain have been, and still are, separately reportable and not bundled into the anesthesia service itself. The exception to this general rule is when the epidural or block is the anesthetic itself. While CMS has not called for significant changes in 2013, anesthesia providers should, nevertheless, be aware of new post-operative pain management coding changes taking effect January 1, 2013.
NCCI Edits
The NCCI edits for 2013 provide, in part, that certain post-operative pain management procedures may only be separately reportable with...
6165 Hits
“Much has changed in health
care since HIPAA was enacted over fifteen years ago,” said HHS Secretary
Kathleen Sebelius in the Department of Health and Human Services’
January 17th press release announcing the publication of the
long-awaited final omnibus rule with Modifications to the HIPAA Privacy,
Security, Enforcement and Breach Notification Rules under the Health
Information Technology for Economic and Clinical Health Act and the
Genetic Information Nondiscrimination Act. “The new rule will help
protect patient privacy and safeguard patients’ health information in an
ever expanding digital age.”
The final omnibus rule will
go into effect on March 26, 2013. Covered entities such as anesthesia
and pain medicine practices and billing companies including ABC—and
their business associates—must be in compliance by September 23, 2013.
The final rule changes HIPAA in several important ways:
It toughens the definition and consequences of failure to notify affected parties of security and privacy breaches;It strengthens...
4851 Hits
 The Centers for Medicare and Medicaid Services (CMS) Contractor Medical Directors (CMDs) recently put together a list of common CMS claim issues that were of concern to various contractors. Several of these items involve services that may impact anesthesia or pain management providers.
1. Use of modifier -59 for imaging with those procedures that now INCLUDE imaging in the code description and payment e.g. paravertebral joint/nerve blocks; transforaminal epidurals, many others.
In some cases, the base procedure includes fluoroscopy or CT imaging and the provider decides to perform the service under ultrasound guidance. Since the ultrasound guidance is not “bundled” in the base procedure description, coders are incorrectly appending modifier 59. However, the base procedure includes the payment for the fluoroscopy or CT imaging. It is incorrect to substitute the required and bundled imaging for another type that is not bundled and bill it separately.
2. Billing for “not qualified” personnel...
The Centers for Medicare and Medicaid Services (CMS) Contractor Medical Directors (CMDs) recently put together a list of common CMS claim issues that were of concern to various contractors. Several of these items involve services that may impact anesthesia or pain management providers.
1. Use of modifier -59 for imaging with those procedures that now INCLUDE imaging in the code description and payment e.g. paravertebral joint/nerve blocks; transforaminal epidurals, many others.
In some cases, the base procedure includes fluoroscopy or CT imaging and the provider decides to perform the service under ultrasound guidance. Since the ultrasound guidance is not “bundled” in the base procedure description, coders are incorrectly appending modifier 59. However, the base procedure includes the payment for the fluoroscopy or CT imaging. It is incorrect to substitute the required and bundled imaging for another type that is not bundled and bill it separately.
2. Billing for “not qualified” personnel...
4061 Hits
The 2013 CPT®
Changes and Codebook are now available to health care providers.
Overall, the 2013 changes include 186 new codes, 119 deleted codes, and
263 revised codes. In addition CPT revised 18 modifiers and updated 150
guidelines. The very good news for anesthesia and pain management
providers is only a small handful of these changes directly impact the
services they routinely provide. Following are general comments
regarding the 2013 changes:
No Anesthesia codes were deleted, revised, or added for 2013.Pain management providers should take note of the four revised codes
and one new code in the nervous system section of CPT 2013. The
majority of changes occur in the denervation subsection, where CPT
revised codes 64612 and 64614 and added 64615 for bilateral
chemodenervation of muscles innervated by the facial, trigeminal,
cervical spinal and accessory nerves.CPT also changed the parenthetical note for code 76942, ultrasound
guidance for needle placement (eg,...
15339 Hits
 In a much awaited pronouncement, on June 1, 2012, the U.S. Department of Health and Human Service’s Office of Inspector General issued Advisory Opinion 12-06 addressing the propriety of two popular schemes to extract money from anesthesiologists, the so-called “company model” and the purported “management fee.”
The advisory opinion could not be more welcome: Just as Willie Sutton, the bank robber, targeted banks “because that’s where the money is,” owners of ambulatory surgery centers continue seek a share of anesthesia fees.
According to a survey conducted by the American Society of Anesthesiologists, 41% of the responding anesthesia practices (125 out of 308) reported being requested by an ASC or its referring physician practice to adopt a company model. Not surprisingly, those 125 practices reported that out of the total 332 requests to participate in a company model entity, the group lost the contract in at least 159 instances.
Company Model...
In a much awaited pronouncement, on June 1, 2012, the U.S. Department of Health and Human Service’s Office of Inspector General issued Advisory Opinion 12-06 addressing the propriety of two popular schemes to extract money from anesthesiologists, the so-called “company model” and the purported “management fee.”
The advisory opinion could not be more welcome: Just as Willie Sutton, the bank robber, targeted banks “because that’s where the money is,” owners of ambulatory surgery centers continue seek a share of anesthesia fees.
According to a survey conducted by the American Society of Anesthesiologists, 41% of the responding anesthesia practices (125 out of 308) reported being requested by an ASC or its referring physician practice to adopt a company model. Not surprisingly, those 125 practices reported that out of the total 332 requests to participate in a company model entity, the group lost the contract in at least 159 instances.
Company Model...
6033 Hits
[Author’s Note: A version of this article originally appeared in the August 2012 issue of Anesthesiology News.]
In a much awaited pronouncement, on June 1, 2012, the U.S. Department of Health and Human Service’s Office of Inspector General issued Advisory Opinion 12-06 addressing the propriety of two popular schemes to extract money from anesthesiologists, the so-called “company model” and the purported “management fee.”
The advisory opinion could not be more welcome: Just as Willie Sutton, the bank robber, targeted banks “because that’s where the money is,” owners of ambulatory surgery centers continue seek a share of anesthesia fees.
According to a survey conducted by the American Society of Anesthesiologists, 41% of the responding anesthesia practices (125 out of 308) reported being requested by an ASC or its referring physician practice to adopt a company model. Not surprisingly, those 125 practices reported that out of the total 332 requests to participate in...
5762 Hits
 The most important event of the year to date, for anesthesiologists and for everyone involved in health care in any way, was of course the Supreme Court decision upholding the Affordable Care Act. Also of great consequence to the anesthesia community was the “company model” Advisory Opinion issued by the Office of the Inspector General on June 1, 2012. Mark Weiss, Esq., whose name is familiar to many readers and for whose frequent contributions to the Communique we are very grateful, describes the company model and the management fee model “other schemes” and explains why these are illegal if they represent payment to the ambulatory surgical center for giving physicians access to Medicare patients. Mr. Weiss’s article adds further clarity by placing the OIG’s June opinion in the context of earlier determinations.
A set of other frequent contributors, Abby Pendleton, Esq., Carey Kalmowitz, Esq. and Adrienne Dresevic, Esq., all...
The most important event of the year to date, for anesthesiologists and for everyone involved in health care in any way, was of course the Supreme Court decision upholding the Affordable Care Act. Also of great consequence to the anesthesia community was the “company model” Advisory Opinion issued by the Office of the Inspector General on June 1, 2012. Mark Weiss, Esq., whose name is familiar to many readers and for whose frequent contributions to the Communique we are very grateful, describes the company model and the management fee model “other schemes” and explains why these are illegal if they represent payment to the ambulatory surgical center for giving physicians access to Medicare patients. Mr. Weiss’s article adds further clarity by placing the OIG’s June opinion in the context of earlier determinations.
A set of other frequent contributors, Abby Pendleton, Esq., Carey Kalmowitz, Esq. and Adrienne Dresevic, Esq., all...
3515 Hits
 Many states have laws or regulations in place that require health insurers in the state to reimburse claims within a certain timeframe or face penalties, oftentimes in the form of interest applied to the amount of the claim. Such laws or regulations are typically called “Prompt Pay” laws or “Clean Claim.” While each state or, sometimes, insurer, defines the requirements for a claim to be a “clean claim,” generally, a “clean claim” is a claim that has all of the information an insurer needs to either pay or deny the claim. A “non-clean claim” is a claim that requires additional information or documentation to make it clean. Each state sets forth the timeframes in which insurers have to reimburse a clean claim. Absent certain exceptions (e.g., instances of suspected fraudulent activity, contractual provisions setting forth alternative timeframes, etc.), failure to adhere to the timeframes results in penalties oftentimes in the form...
Many states have laws or regulations in place that require health insurers in the state to reimburse claims within a certain timeframe or face penalties, oftentimes in the form of interest applied to the amount of the claim. Such laws or regulations are typically called “Prompt Pay” laws or “Clean Claim.” While each state or, sometimes, insurer, defines the requirements for a claim to be a “clean claim,” generally, a “clean claim” is a claim that has all of the information an insurer needs to either pay or deny the claim. A “non-clean claim” is a claim that requires additional information or documentation to make it clean. Each state sets forth the timeframes in which insurers have to reimburse a clean claim. Absent certain exceptions (e.g., instances of suspected fraudulent activity, contractual provisions setting forth alternative timeframes, etc.), failure to adhere to the timeframes results in penalties oftentimes in the form...
4991 Hits
 With the ever-rising cost of healthcare, all parties are looking for ways to finance it. From high deductible health plans with savings components to consumer credit tools such as credit cards and loans, the face of healthcare financing is changing. The challenge for anesthesia in this ever-changing world comes back to the physician-patient relationship.
As noted in previous articles “The Benefits of Strategy” from the Winter 2012 issue of The Communique and “Planning for Payor Negotiations” from the Spring 2012 issue of The Communique, high deductible health plans (HDHPs) are a growing health insurance product line. This puts a greater emphasis on collecting larger sums of money from the patient. Moreover, the current economic climate has put a strain on the safety nets that are in place to help those with fewer resources. The self-pay category is growing and the need to address this issue is at the forefront in...
With the ever-rising cost of healthcare, all parties are looking for ways to finance it. From high deductible health plans with savings components to consumer credit tools such as credit cards and loans, the face of healthcare financing is changing. The challenge for anesthesia in this ever-changing world comes back to the physician-patient relationship.
As noted in previous articles “The Benefits of Strategy” from the Winter 2012 issue of The Communique and “Planning for Payor Negotiations” from the Spring 2012 issue of The Communique, high deductible health plans (HDHPs) are a growing health insurance product line. This puts a greater emphasis on collecting larger sums of money from the patient. Moreover, the current economic climate has put a strain on the safety nets that are in place to help those with fewer resources. The self-pay category is growing and the need to address this issue is at the forefront in...
4015 Hits
F1RSTUseTM is the first—and only—full-service EHR management platform built exclusively for anesthesiologists and pain management specialists to satisfy with ease Stage 1 of Meaningful Use as required to earn the Medicare EHR incentive payment. It is the only product that provides the full service measures to ensure success: tracking the necessary data points, providing reports of successful measures and ensuring that you are meeting all of the CMS requirements.As a number of physicians have begun to incorporate the F1RSTUse system into their workflow, additional questions regarding the Meaningful Use program have been received. Read on to learn more about F1RSTUse and how it can support your Meaningful Use program.This checklist has been compiled from questions raised by anesthesiologists, colleagues, facilities, and patients. 1. What is the maximum incentive payment if I start now? – $39,000. If you have not already enrolled in the F1RSTUse system, the original $44,000 incentive payment is...
4779 Hits
 Several clients have inquired as to the documentation and correct coding and billing for Transesophageal Echocardiography (TEE) services. A TEE is a special diagnostic tool, which may be used by properly trained physicians (i.e., anesthesiologists, cardiologists) to benefit patient care. A separately reported TEE may be performed for monitoring and/or diagnostic purposes. However, many payers will only reimburse diagnostic studies.
For example, to establish conditions such as myocardial ischemia or cardiac valve disorders, the anesthesiologist will be utilizing the transesophageal echo for diagnostic purposes. In this case, when the anesthesiologist has the additional certification or documented training in residency, and is privileged by the hospital to do the complete procedure, the anesthesiologist can and should bill separately for the TEE in addition to the anesthesia. The correct CPT code for the complete procedure is 93312. When you bill for both the anesthesia and the TEE, the coder must append...
Several clients have inquired as to the documentation and correct coding and billing for Transesophageal Echocardiography (TEE) services. A TEE is a special diagnostic tool, which may be used by properly trained physicians (i.e., anesthesiologists, cardiologists) to benefit patient care. A separately reported TEE may be performed for monitoring and/or diagnostic purposes. However, many payers will only reimburse diagnostic studies.
For example, to establish conditions such as myocardial ischemia or cardiac valve disorders, the anesthesiologist will be utilizing the transesophageal echo for diagnostic purposes. In this case, when the anesthesiologist has the additional certification or documented training in residency, and is privileged by the hospital to do the complete procedure, the anesthesiologist can and should bill separately for the TEE in addition to the anesthesia. The correct CPT code for the complete procedure is 93312. When you bill for both the anesthesia and the TEE, the coder must append...
40745 Hits
 The focus on quality outcomes in healthcare has been long in coming. As the cost of health care continues to rise faster than the cost of living, the nation finds itself facing a dilemma. Perhaps a free market approach to healthcare is not the best approach after all. Economic incentives and ground breaking research have clearly provided significant advances in some areas, but what has been their impact on cost? As diverse and independent as the specialty of anesthesiology is, its practitioners have challenged the leadership to take the lead in finding ways to provide quality care more consistently so that anesthesia is not a contributor to the cost of healthcare but a regulator of spending.
While virtually all anesthesiologists and CRNAs have now become familiar with the current requirements of the Physician Quality Reporting System (PQRS), this is just one example of a public approach to ensuring consistency based on...
The focus on quality outcomes in healthcare has been long in coming. As the cost of health care continues to rise faster than the cost of living, the nation finds itself facing a dilemma. Perhaps a free market approach to healthcare is not the best approach after all. Economic incentives and ground breaking research have clearly provided significant advances in some areas, but what has been their impact on cost? As diverse and independent as the specialty of anesthesiology is, its practitioners have challenged the leadership to take the lead in finding ways to provide quality care more consistently so that anesthesia is not a contributor to the cost of healthcare but a regulator of spending.
While virtually all anesthesiologists and CRNAs have now become familiar with the current requirements of the Physician Quality Reporting System (PQRS), this is just one example of a public approach to ensuring consistency based on...
6488 Hits
 By Abby Pendleton, Esq., Carey Kalmowitz, Esq. and Adrienne Dresevic, Esq. The Health Law Partners, P.C., Southfield, MI
On June 1, 2012, the Department of Health and Human Services Office of Inspector General (the “OIG”) issued its Advisory Opinion No. 12-06, which provides long-awaited guidance to the health care industry regarding the legal permissibility of an anesthesia delivery service model commonly referred to as the “company model.” Insofar as Advisory Opinion No. 12-06 is the initial OIG guidance that specifically focuses on such an arrangement and determines that the factual paradigms presented implicate risks under the Medicare and Medicaid Antikickback Statute (the “AKS”), this Advisory Opinion understandably is capturing broad attention within the medical and legal communities. While OIG Advisory Opinion 12-06 clarifies the almost-axiomatic observation that company model arrangements, especially those that contain the indicia that the OIG historically has identified as problematic under the AKS, certainly have the potential...
By Abby Pendleton, Esq., Carey Kalmowitz, Esq. and Adrienne Dresevic, Esq. The Health Law Partners, P.C., Southfield, MI
On June 1, 2012, the Department of Health and Human Services Office of Inspector General (the “OIG”) issued its Advisory Opinion No. 12-06, which provides long-awaited guidance to the health care industry regarding the legal permissibility of an anesthesia delivery service model commonly referred to as the “company model.” Insofar as Advisory Opinion No. 12-06 is the initial OIG guidance that specifically focuses on such an arrangement and determines that the factual paradigms presented implicate risks under the Medicare and Medicaid Antikickback Statute (the “AKS”), this Advisory Opinion understandably is capturing broad attention within the medical and legal communities. While OIG Advisory Opinion 12-06 clarifies the almost-axiomatic observation that company model arrangements, especially those that contain the indicia that the OIG historically has identified as problematic under the AKS, certainly have the potential...
3389 Hits
The percentage of patients requiring the highest level of service in the emergency department at Faxton St. Luke’s Healthcare in Utica, NY rose 43 percent in 2009, as reported in the New York Times on September 21, 2012. Level 5 ED visit services (CPT® code 99285) at Baptist Hospital in Nashville, TN increased by 82 percent in 2010, and by a comparable amount at Methodist Medical Center of Illinois in Peoria. More than 80 percent of Methodist Memorial’s Medicare ED evaluation and management (E/M) claims were for Level 5 services in 2010, as they were at Yuma Regional Medical Center in Yuma, AZ in 2007. At Baylor Medical Center in Irving, TX, 64 percent of all ED visits for Medicare patients were Level 5 services, and another 16 percent were Level 4.These are just a few examples of hospitals experiencing a startling rate of growth of high-intensity E/M services during the last few...
4045 Hits
Many “Covered Entities” within the meaning of the privacy and security provisions of the Health Insurance and Portability Act of 1996 (HIPAA) are managing more and more of their patient information electronically. Indeed, not moving to electronic health records (EHRs) may cost physicians a percentage of their Medicare remittances—or at least the loss of a potential bonus of up to $44,000—under the EHR Incentive Program, as discussed in our last several Alerts.Collecting, analyzing, reporting and storing electronic patient information present perhaps even greater HIPAA challenges than does the use of paper records, however. Data entered on a computer can be copied more easily, more cheaply, more prolifically and even passively. Once unsecured data are moved from the computer on which they are created to other media, manually or wirelessly, controlling the information becomes nearly impossible. The key word in the preceding sentence is “unsecured.” The recently finalized HIPAA regulations on Breach Notification impose...
5275 Hits
 Does the title of this article seem boring – or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences...
Does the title of this article seem boring – or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences...
4367 Hits
 The Anesthesia Quality Institute was founded to create and maintain the National Anesthesia Clinical Outcomes Registry (NACOR). This project is now two and a half years old and more than 135 practices, including nine ABC clients, have contributed more than 5 million records to this “every case, every day” registry. Participants have online access to the NACOR Reporting Server, where they can see continually updated summaries of their practice performance and aggregated national benchmarks. This information, and the ability to slice and dice it to examine subsets of interest, is an important business and quality management tool. After all, what can’t be measured can’t be improved.
Or can it? Although we pride ourselves on our data-driven, scientific, high-tech practice, anesthesiology remains as much art as science. As the popularity of morbidity and mortality conferences attests, there is a lot to be learned from the unfortunate experience of others. Schadenfreude aside,...
The Anesthesia Quality Institute was founded to create and maintain the National Anesthesia Clinical Outcomes Registry (NACOR). This project is now two and a half years old and more than 135 practices, including nine ABC clients, have contributed more than 5 million records to this “every case, every day” registry. Participants have online access to the NACOR Reporting Server, where they can see continually updated summaries of their practice performance and aggregated national benchmarks. This information, and the ability to slice and dice it to examine subsets of interest, is an important business and quality management tool. After all, what can’t be measured can’t be improved.
Or can it? Although we pride ourselves on our data-driven, scientific, high-tech practice, anesthesiology remains as much art as science. As the popularity of morbidity and mortality conferences attests, there is a lot to be learned from the unfortunate experience of others. Schadenfreude aside,...
4970 Hits