Anesthesia Industry eAlerts
Sent to subscribers every Monday morning, our eAlerts deliver timely updates on regulatory, legislative and practice management developments of interest to anesthesia professionals.
Complete the simple form below to subscribe.
Medicare Eliminates Patient Cost-Sharing for Anesthesia for Screening Colonoscopies
December 8, 2014
Medicare will cover 100 percent of the allowable amount for screening colonoscopies effective January 1, 2015. Patients will still be responsible for co-payments and deductibles for diagnostic and therapeutic colonoscopies, however, as well as for co-payments for screening colonoscopies that end up with a biopsy or polyp removal.
If you provide anesthesia for a Medicare patient undergoing a screening colonoscopy, you will be able to collect 100 percent of the allowable amount from Medicare and will not need to bill the patient for any co-payment or deductible, beginning on January 1, 2015. You must, however, identify the service as screening rather than diagnostic or therapeutic through the use of the appropriate modifier on your claim.
In the interest of making preventive care more widely available, a provision of the Affordable Care Act, Section 4104, waived “colorectal cancer screening test” co-payments and deductibles for Medicare beneficiaries. For the same reason—to avoid patient cost-sharing’s becoming “a significant barrier to these essential preventive services”—CMS extended the waiver of coinsurance and deductible to anesthesia services furnished in conjunction with a screening colonoscopy in the Final Rule on the Physician Fee Schedule for 2015.
As CMS observed,
A recent study in The Journal of the American Medical Association (JAMA) cited an increase in the percentage of colonoscopies and upper endoscopy procedures furnished using an anesthesia professional, from 13.5 percent in 2003 to 30.2 percent in 2009 within the Medicare population, with a similar increase in the commercially-insured population. [Liu H, Waxman DA, Main R, Mattke S. Utilization of Anesthesia Services during Outpatient Endoscopies and Colonoscopies and Associated Spending in 2003-2009. (2012). JAMA, 307(11):1178-1184.] A 2010 study projected that the percentage of this class of procedures involving an anesthesia professional would grow to 53.4 percent by 2015. [Inadomi, J. M. et al. (2010). Projected increased growth rate of anesthesia professional–delivered sedation for colonoscopy and EGD in the United States: 2009 to 2015. Gastrointestinal Endoscopy, 72, 580-586.] These studies suggest that the prevailing practice for endoscopies in general and screening colonoscopies in particular is undergoing a transition, and that anesthesia separately provided by an anesthesia professional is becoming the prevalent practice. In preparation for the proposed rule, we reviewed these studies and analyzed Medicare claims data. We saw the same trend in screening colonoscopies for Medicare beneficiaries with 53 percent of the screening colonoscopies for Medicare claims submitted in 2013 had [sic] a separate anesthesia claim reported.
By extending the waiver to anesthesia for screening colonoscopies, CMS has implicitly acknowledged that anesthesia provided by an anesthesia professional is just as “medically necessary” as the moderate sedation that is bundled into the gastroenterologist’s fee. If the service is important enough to be treated like other screening procedures for which the copayment and deductible are waived, logically the anesthesiologist must be paid by Medicare too.
Some of the Medicare Administrative Contractors (MACs) have issued policies limiting more or less narrowly the circumstances under which they will deem anesthesia for routine screening colonoscopies medically necessary. In its response to several public comments filed on the proposal that gave rise to the Final Rule, CMS stated, “This final rule with comment period establishes national policy and takes precedence over any local coverage policy that limits Medicare coverage for anesthesia services furnished during a screening colonoscopy by an anesthesia professional.” Practices with claims that are denied on medical-necessity grounds may need to appeal while their MAC catches up with the new Medicare policy.
Use Modifiers to Differentiate Between Screening and Diagnostic/Therapeutic Services
Going forward, Medicare will pay 100 percent of the allowed amount for screening colonoscopies and there will be no cost-sharing. Diagnostic or therapeutic colonoscopies, on the other hand, continue to require co-payments and deductibles. What about procedures that start out as screening, but in which a polyp or other tissue is found and removed?
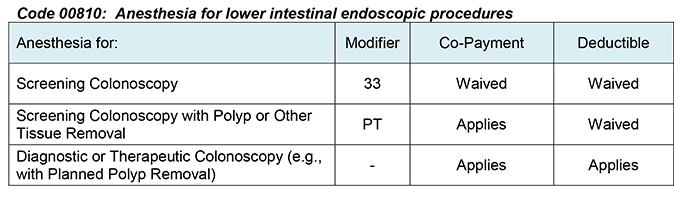
CMS indicated in the Final Rule that providers should include modifier 33 on the claim line with the code for an anesthesia service furnished in conjunction with a colorectal cancer screening test (i.e., 00810, Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to duodenum). In procedures that begin as a colorectal cancer screening test, but for which another service such as a colonoscopy with polyp removal is actually furnished, the anesthesia professional should report modifier PT on the claim line rather than modifier 33.
This is because CMS believes that a specific statutory provision, section 1834(d)(3)(D) of the Social Security Act, prevents it from paying for an anticipated screening colonoscopy that ends up involving a biopsy or polyp removal as a screening colonoscopy. Patients are therefore required by the statute to pay their 20 percent co-payment amount for diagnostic or therapeutic colonoscopies. A different part of the Social Security Act, section 1833(b)(1) as amended by the ACA, addresses screening colonoscopies, however. Under that provision, Medicare can and does waive the deductible for colorectal screening tests whether or not there is a biopsy or removal of tissue. The Final Rule applies that waiver to the anesthesia service in conjunction with the planned screening procedure that turned into a biopsy or polypectomy. Thus there are three distinct scenarios:
In order to report the services correctly, anesthesiologists providing anesthesia for colonoscopies will need to adequate document whether the service was a colorectal cancer screening test or a colorectal cancer screening test that was converted to a diagnostic or therapeutic procedure. The anesthesiologist may want to corroborate the nature of the procedure with the gastroenterologist.
If the goal is prevention of disease, it is not logical to waive the patient’s financial responsibility only for screening colonoscopies that do not involve polyp or tissue removal and not for procedures that end up with unplanned diagnostic or therapeutic services—but the result is an artifact of provisions of the Social Security Act being written or amended at different times, not as a whole piece. That is why legislators introduced the "Removing Barriers to Colorectal Cancer Screening Act" in Congress, as H.R. 1070 in the House (2013) and as S. 2348 in the Senate (2014). The bill would eliminate cost sharing for Medicare beneficiaries receiving a routine screening colonoscopy, even when a polyp is removed—something that Congress did for patients with commercial insurance in the ACA itself. Unfortunately, the legislation is stuck in Committee and is not given good odds of passage.
Eliminating the patient co-payment and deductible for anesthesia for screening colonoscopies is still an important advance. It will benefit those patients who were until now deterred by the cost-sharing amounts for which they were liable. The change will also be welcomed by anesthesia practices that will receive payment more quickly and without the need to bill patients.
With best wishes,
Tony Mira
President and CEO