Anesthesia Industry eAlerts
Sent to subscribers every Monday morning, our eAlerts deliver timely updates on regulatory, legislative and practice management developments of interest to anesthesia professionals.
Complete the simple form below to subscribe.
Anesthesia Conversion Factors If There Is No Legislation
January 19, 2010
When anesthesiologists begin receiving their Medicare payments for services provided in January 2010, they should see no change from their 2009 conversion factors. On March 1st, however, Medicare rates will drop 21.2 percent – unless Congress passes legislation correcting the impact of the Sustainable Growth Rate on which the calculation of the annual fee schedule is based. Table 1 below shows the anesthesia conversion factors for 2008, 2009 and 2010, and the year-to-year differences between them, by carrier/contractor locality.
Table 1. 2009, 2009 and 2010 Anesthesia Conversion Factors

The first thing one notices is that the difference between 2009 and 2010 rates is not a uniform -21.2 percent. Some localities even have a positive update. This is because the geographic adjuster applicable to each locality varies considerably. On January 1, 2010, the statutory “floor” on the geographic practice cost indices (GPCIs) floor for “work” relative values was removed (except in Alaska).
The negative changes are in general larger than the increases. The conversion factor for Puerto Rico, which has for the entire life of the Medicare Fee Schedule been several standard deviations from the mean, incurs the greatest decrease. Table 2 lists the 91 localities in the order of their decrease.
Table 2. Localities in Order of Decrease
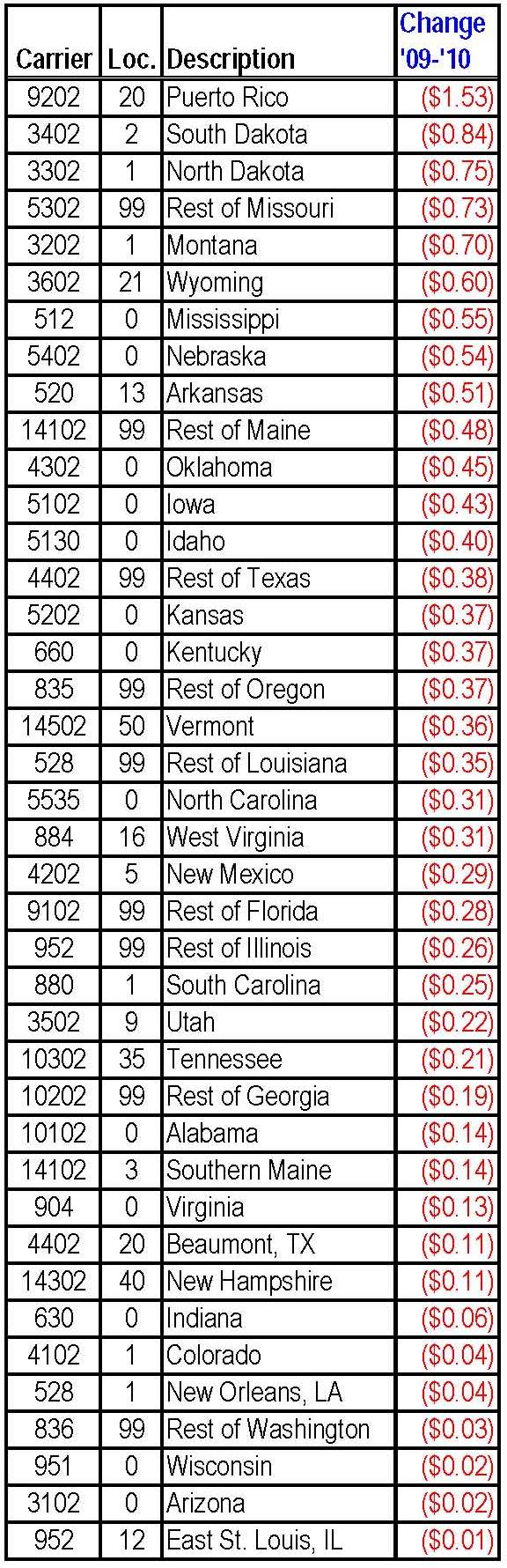
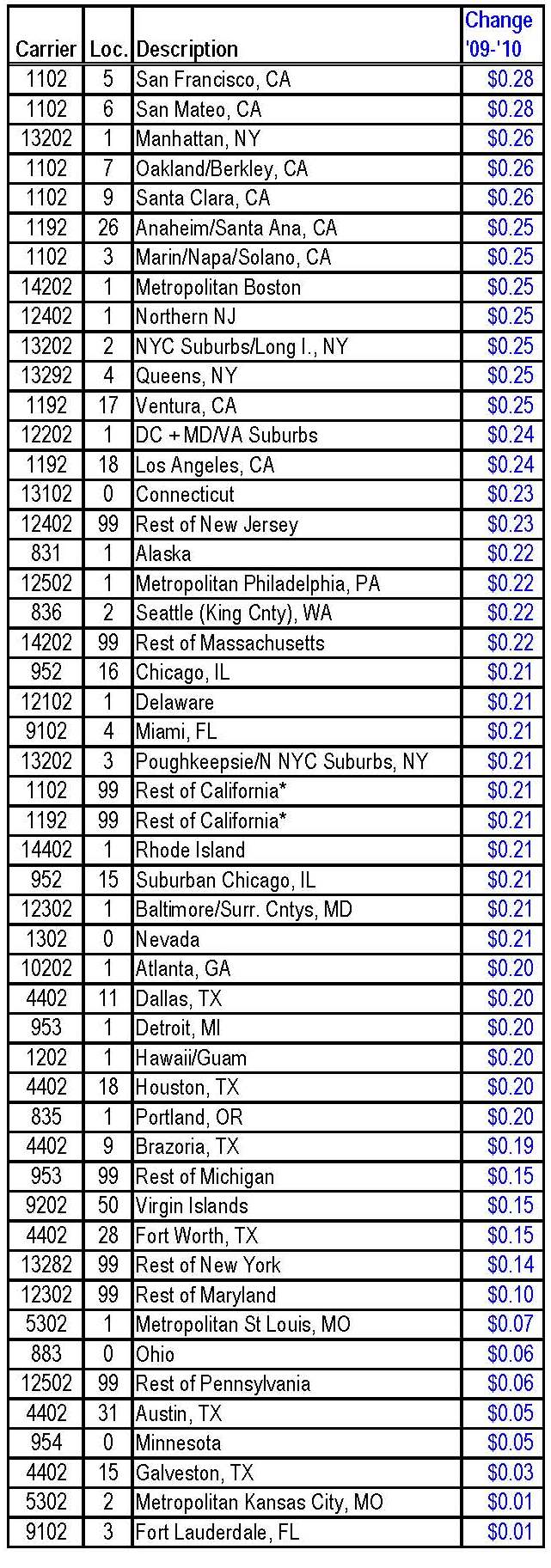
Nine localities will experience conversion factor reductions of more than $0.50, if the SGR effect is not blocked by legislation before March 1st. Seven will see cuts of less than $0.10 (0.05% to 0.3%). The greatest projected increase, as shown in Table 3, is $0.28 in San Francisco (1.26%) and nearby San Mateo (1.25%). This brings us to the second general observation: the GPCI changes translate to payment reductions in more rural areas and to increases in metropolitan localities. Such a shift will not tend to attract more anesthesia providers to rural area, where they are in the relatively shortest supply.
Table 3. Localities in Order of Increase
The third conclusion, looking at Table 1 above and at Column I in particular, is that most anesthesiologists will still be ahead of where they stood, in terms of the Medicare conversion factor, 13 months ago. Indiana, for example, will have gone from $19.03 in 2008 to $20.10 in 2010. What this would mean, of course, is that the large adjustment to anesthesia work values to which the Relative Value Update Committee (RUC) and CMS finally agreed effective January 1, 2008, will be essentially nullified by this year’s SGR reduction – if that reduction is implemented.
Many of you have contacted your Senators and Congressmen repeatedly to urge them to support repeal of the SGR. It is vitally important that you do so again now. Remember that CMS estimates that continued reductions of 5 percent to 6.5 percent each year, on top of the 21.2 percent cut, will take place over the next several years unless Congress repeals or changes the sustainable growth rate formula. If Ms. Coakley loses today’s special election for the late Senator Kennedy’s seat, as most polls are indicating that she will, passage of health system reform becomes even more difficult. Let your representatives hear from you that they must adopt legislation fixing the SGR problem once and for all. You may contact them through the Capitol Switchboard at (202) 225-3121.
With best wishes,
Tony Mira
President and CEO