Anesthesia Industry eAlerts
Sent to subscribers every Monday morning, our eAlerts deliver timely updates on regulatory, legislative and practice management developments of interest to anesthesia professionals.
Complete the simple form below to subscribe.
2021 CPT Coding Changes: Relevance for Anesthesia and Chronic Pain
There are changes every year to the coding guidelines as found in the CPT manual. For 2021, the primary changes will revolve around certain evaluation and management services.
January 4, 2021
With every new year, there arises within us the hope of better days ahead—a certain optimism fostered by a clean slate and a wide-ranging set of possibilities. New Year is a time of change. That holds true for the individual who resolves to make improvements in diet or lifestyle, and it’s often true in areas of business and government. New laws or policies go into effect with the coming of every January 1, and thus we are all programmed to prepare for annual change.
One thing we can always count on to change with the start of a new year is the content of the CPT coding manual. Each year, the American Medical Association (AMA) makes changes to this resource in terms of added, deleted or revised codes/descriptors in addition to making other important modifications. We keep track of these changes as they directly impact the coding, billing and documentation rules we and our clients must follow. The purpose of this alert is to provide our readers with a summary of the major coding, utilization and documentation changes found in the 2021 CPT manual that are most relevant to the practice of anesthesia and pain management.
General Changes
The following provides a general summation of CPT changes, along with a few examples that might apply to some of our readers.
The 2021 CPT edition includes 206 new codes, 69 revised codes and 54 deleted codes. The greater part of these changes do not affect anesthesia, though there are significant changes for Office and Outpatient evaluation and management (E/M) visits.
The majority of the CPT changes for 2021 involved codes found in the Surgery Section, Pathology/Laboratory Section and Category III Section of the CPT manual. One example involves CPT code 55880, which was created for the High Intensity Focused Ultrasound (HIFU) that is used for ablation of malignant prostate tissue. Though this code was approved by the FDA, many current carrier policies include verbiage stating this procedure is considered experimental and not approved for reimbursement. The policies will need to be reviewed for any updates in reimbursement status.
In the Pain Management section, the current codes for Transforaminal Injections under ultrasound guidance were deleted (CPT codes 0228T- 0231T), with these services now being reported with the unlisted code 64999.
E/M Changes
As expected, there were major changes to the E/M coding guidelines related to Office and Outpatient visits (CPT 99202-99215). For example, CPT 99201 has been deleted. In addition, Office and Outpatient visits that were previously coded based on one of two ways [(a) the 1995 or 1997 CMS guidelines, or (b) time spent on coordinating and counseling care] are now to be coded based on one of the two ways listed below.
1. Total Time on the same calendar day of visit. NOTE: Clinical staff time does not count toward total time, and two billable providers cannot count the same time.
Time that can be counted on the same day:
Preparing to see the patient (e.g., reviewing tests)
Obtaining and/or reviewing separately obtained history
Performing a medically appropriate examination and/or evaluation
Counseling and educating the patient/family/caregiver
Documenting clinical information in the medical record
Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver
Care coordination (not separately reported)


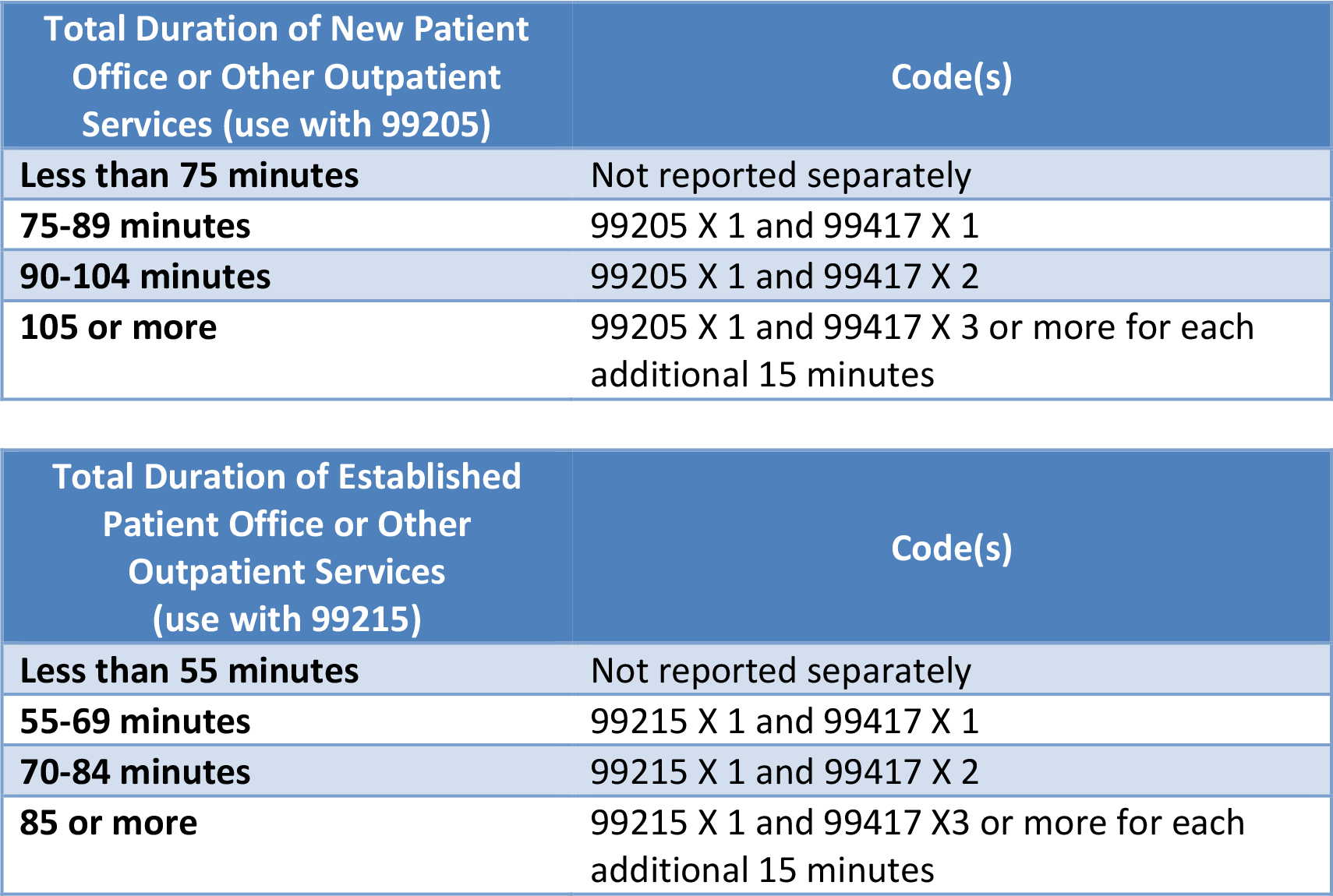
CPT code 99417 was created to report prolonged office or other outpatient evaluation and management services beyond the minimum required time of the primary procedure, and would be used as follows:

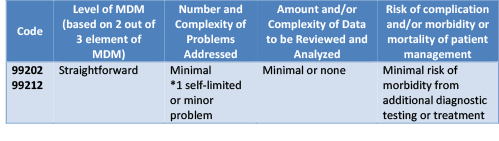
2. Medical Decision Making (MDM). NOTE: You are still required to document a “medically appropriate” history and/or examination. Your code level will be based on the extent to which you meet the documentation elements listed in the below charts.



Remember that total time should be documented on all office and other outpatient visits. This allows code level determination to be based on the methodology that will best benefit the provider/group.
More information pertaining to anesthesia-specific coding changes will be forthcoming in a future article as soon as publications, such as the ASA Crosswalk and the Relative Value Guide, become available for review. If you have questions about the changes discussed herein, please contact your account executive or reach out to us at info@anesthesiallc.com.
With best wishes,
Tony Mira
President and CEO