May 23, 2016
Patients are directly responsible for larger and larger healthcare bills as cost-sharing increases. Demand for price transparency and certainty is increasing. Surgery centers, along with aggregator websites offering comparative information, are beginning to meet that demand.
“Transparency” is a word that you will encounter more and more frequently in health policy articles, including ABC’s publications. Information transparency is a key for enabling healthcare purchasers to make value-based decisions concerning the quality and price of services. Those data are slowly becoming more available, but they remain largely inaccessible to most potential users.
CMS recently released the third year of information from the Medicare Provider Utilization and Payment Data: Physician and Other Supplier database. The database is comprehensive and offers the following information for every physician or Part B supplier who submitted claims in 2014: name, address, gender, specialty, procedure (by HCPCS/CPT™ code), place of service, number of services, number of Medicare beneficiaries, average payment amount, average allowed charge and average submitted charge. What is missing is any information on patients or on outcomes. This being a Medicare database, it excludes the two-thirds of patients who are not in the Medicare fee-for-service program. Its greatest utility is in revealing what an individual physician collected from Medicare for a given service or procedure, and how often he or she performed it.
There is a growing effort to making prices transparent to patients up front, before they obtain medical services. To many observers, this only makes sense. Marty Makary, MD, in an interview entitled Get Ready for Surgical Price Transparency posted on the website of the ORExcellence conference that will take place in October 2016 conference, said:
We wouldn’t consider the current business model acceptable in any other setting. Take the supermarket. Imagine that you couldn’t see the prices at the store until after the cashier charged you, and you weren’t allowed to ask for a refund or take items back. And when the products were rung up, you would see that items like oranges had a 4- or 6-fold markup. You would be shocked, and probably consider it an incompetent marketplace with tremendous waste. Essentially, that’s what we have in healthcare right now with nontransparent markets.
Medical and hospital charges continue to increase at rates that outpace inflation. Health insurance deductibles and co-payments are growing even faster. From 2010 to 2015, the proportion of insured workers covered by high deductible health plans increased from 13 percent to 24 percent, according to the Kaiser Family Foundation. Consumers who are now paying large sums out of pocket want to know what healthcare services they are buying and at what price.
Malcolm Bird, a nervous first-time parent, took his one year old to the local emergency department (ED) for a cut on her finger. The ED physician washed the child’s hand and put a Band-Aid on her finger. Bird was shocked to receive a bill for $629.00. The amount for which he was actually liable under his health plan, not yet having met his annual deductible, was $440.30. When questioned by a reporter about how the hospital calculated its ED facility charge, the hospital wrote off the entire bill, which it had refused to do when Bird had protested. According to the reporter, a simple “solution might be transparency—requiring hospitals to post their facility fees on the door so that patients have a sense of what the base price is for entry. Bird says that would have helped in his situation; if he’d seen the typical charges, he probably would have just called a friend who was a doctor.” (Kliff S. The case of the $629 Band-Aid—and what it reveals about American healthcare. Vox Science & Health, May 13, 2016).
It is very difficult for most consumers to ascertain ED charges because facility fees vary hugely and apparently arbitrarily—Kliff cites a study showing that ED bills for common procedures can vary from $15 to $17,797—and because hospitals rarely make them public. When hospitals do make price information available, it is usually presented as an average figure, with predictable disclaimers about possible variation based on “complexity,” e.g., MetroHealth in the Grand Rapids, MI area.
A very few ambulatory surgery centers (ASCs) have opted to post fixed prices for certain procedures—beyond the self-paid cosmetic and LASIK procedures that started the trend. In our eAlert of January 27, 2014 (Payments for Anesthesia Services in the Sunshine), we noted that the six-O.R. Surgery Center of Oklahoma in Oklahoma City, founded and managed by two anesthesiologists, listed more than 100 procedures on its website, each with an all-inclusive price covering the facility fee, the surgeon’s fee and anesthesia (but not hardware and implants). The Center kept its prices relatively low in part by requiring up-front payments from self-pay patients, and by not participating with Medicare or most private payers. The 47 surgeons who performed between 600 and 700 cases per month were all financially invested in the facility and thus have a shared interest in maintaining high quality. The Center had attracted the attention not just of patients with no insurance or with high deductibles, but also of self-insured employers, and even of a neighboring full-service hospital, to which the Center sent patients needing “another day or 2 to sleep it off after their surgery” for a predetermined per-day price. (Burger J. Is Surgery Ready for Price Transparency? Outpatient Surgery Magazine Online, September 2013.)
The St. George Surgery Center in southern Utah goes farther in what it includes in the current total of 210 package prices available through drop-down menus on the opening screen of the ASC’s website. The prices cover implants, hardware and a stay of up to 23 hours in addition to the surgeons’ and anesthetists’ fees. One pre-op and one post-op visit are included, but diagnostic tests and imaging are not; nor is the treatment of complications.
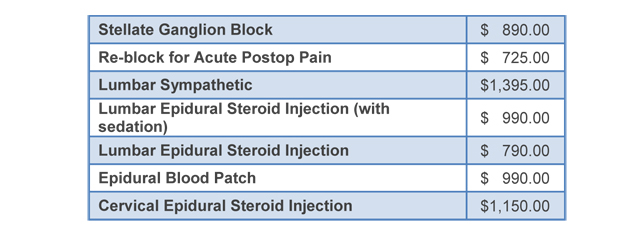
St. George spent months determining exactly what they spent on each procedure, gathering “surgical nurses, personnel in charge of buying supplies and the staff who manage our current supply inventory, combing through surgeons’ preference cards and used data management software to look up how much we spend on the 50 to 100 items used by each surgeon for every case.” (Hadlock J. Shopping for Surgery: How to Make the Self-Pay Model Work for You and Your Patients. Outpatient Surgery Magazine Online, June 2015.) The ASC negotiated fixed fees with its surgeons. Below are the package prices listed under “Pain Procedures:”
The Oklahoma City and St. George ASCs offer a clear attraction to self-pay patients—but only to self-pay patients. Their prices may be a fraction of what patients expect to pay elsewhere. The ASCs save considerable billing and collection costs by requiring direct payment at the time of scheduling.
Patients with insurance, and the employers who purchase the insurance, have a growing number of innovative options for comparison shopping and limiting their financial exposure for healthcare services. Among these are:
- Healthcare Bluebook. A website that asks the user to enter a city or zip code and a procedure, test or service, for which it then produces a “fair price.” As an example, the fair price for an anterior cruciate ligament repair in Arlington, VA is $9,388, broken down as follows:
- Outpatient facility services $6,144
- Surgeon fee for procedure and routine post-op care $2,195
- Anesthesia (average surgery time; may vary) $999
- For each of these components, the Healthcare Bluebook offers a downloadable, printable detailed pricing agreement that patients may use to negotiate with the service provider.
- clearhealthcosts.com. A search engine that uses reported pricing from patients and providers to relay the cost of procedures performed in New York City and its suburbs, San Francisco, Los Angeles, Houston, Dallas, San Antonio and Philadelphia, with more cities being added.
- pratter.us. A secure portal where hospitals and surgery centers upload their prices for procedures, providing access to self-pay patients. The portal provides links to participating facilities’ homepages to direct interested individuals whose employers have contracted with the service.
- medibid.com. Gives elective surgery patients who are willing to pay out of pocket the ability to choose from a range of physicians and hospitals bidding, eBay-style, to provide the surgery.
Although there are only a few ASCs or hospitals that make it easy for the public to determine prices in advance of receiving healthcare services, and a very limited number of services that provide comparative information today, the handwriting is on the wall. Consumers who are going to pay thousands of dollars for their care are going to be shopping for the best value. “Value” includes quality, and although the medical professions and hospital administrators may challenge the validity of current quality metrics, consumers are going to use the performance measures that are made available. The St. George Surgery Center, for example, provides and explains its surgical infection rate as well as patient satisfaction scores.
Anesthesiologists need to understand the costs of their services, to measure “quality” using standard metrics and to prepare to negotiate on the basis of transparency.
With best wishes,
Tony Mira
President and CEO