Many pain medicine procedures, and, increasingly, perioperative and critical care procedures such as central venous access are performed using ultrasound guidance (U/S). Indeed, U/S is an integral part of many CPT® codes, e.g., 20604 [Arthrocentesis, aspiration and/or injection, small joint or bursa, (e.g., fingers, toes), with ultrasound guidance, with permanent recording and reporting]. When and where, and by whom, must those permanent images be stored? What if another entity, such as a hospital, is responsible for storing them? According to Sonosite,
All diagnostic ultrasound examinations, including those when ultrasound is used to guide a procedure, require that permanently recorded images be maintained in the patient record. The images can be kept in the patient record or some other archive--they do not need to be submitted with the claim. Images can be stored as printed images, on a tape or electronic medium. Documentation of the study must be available to the insurer...
2921 Hits
 One important voice sounding a warning or at least a heads-up about what is coming is that of Mark Weiss, Esq. The title of Mr. Weiss’s article— Impending Death of Hospitals: Will Your Anesthesia Practice Survive?—which is also the title of his forthcoming book—is intentionally provocative. He lays out several of the major threats confronting hospitals, starting with health system growth, through mergers and acquisitions, acquisition of physician practices and investments in integrated delivery networks. Others have predicted that the Federal Trade Commission will place a damper on hospital merger activity in 2016, but the quest for greater scale and scope is going to continue. Anesthesiologists may want to consider the wisdom of relying on the ongoing health of just one or two hospitals. This is especially true in light of the ability of physician-owned facilities, notably ambulatory surgery centers, and new technologies (think telemedicine) to disrupt hospitals’ traditional business. Mr....
One important voice sounding a warning or at least a heads-up about what is coming is that of Mark Weiss, Esq. The title of Mr. Weiss’s article— Impending Death of Hospitals: Will Your Anesthesia Practice Survive?—which is also the title of his forthcoming book—is intentionally provocative. He lays out several of the major threats confronting hospitals, starting with health system growth, through mergers and acquisitions, acquisition of physician practices and investments in integrated delivery networks. Others have predicted that the Federal Trade Commission will place a damper on hospital merger activity in 2016, but the quest for greater scale and scope is going to continue. Anesthesiologists may want to consider the wisdom of relying on the ongoing health of just one or two hospitals. This is especially true in light of the ability of physician-owned facilities, notably ambulatory surgery centers, and new technologies (think telemedicine) to disrupt hospitals’ traditional business. Mr....
2589 Hits
The anesthesia record, like medical records in general, should be complete and accurate at the time when the physician signs it—ideally. In practice, it occasionally requires amendment. Given the huge role that accurate documentation plays in our medical payment system, compliance with the rules and regulations governing medical record amendments is important. Altered medical records have great potential for fraud, especially if the added information helps to raise the level of a billable service, and no one should be surprised if auditors look at any changes closely.
One basic principle was added to the first paragraph of the provision that regulates amendments in Chapter 3 of the Medicare Program Integrity Manual, Section 3.3.2.5, when that provision was updated effective October 2, 2015. The intent of the new paragraph is to make it clear that amendment should be the exception.
All services provided to beneficiaries are expected to be documented in the...
3316 Hits
Recent media coverage of surgeons operating in two concurrent cases raises three issues: (1) patient safety, (2) compliance with the Medicare teaching physician billing rules and (3) transparency vis-à-vis patients.
The Safety Controversy
The question whether it is right or safe for surgeons to run two operations at once erupted publicly last year when the Boston Globe published a detailed report (Clash in the Name of Care) focusing on events that had occurred at Massachusetts General Hospital (MGH) in August 2012. A 41-year old patient had undergone complicated spinal surgery from which he emerged a quadriplegic, and it revealed itself that his surgeon had been in and out of the operating room, attending to a patient undergoing spinal fusion in another OR for seven of the eleven hours that the first case took to complete.
A controversy among MGH surgeons and anesthesiologists over concurrent surgeries had been years in the making. ...
4073 Hits
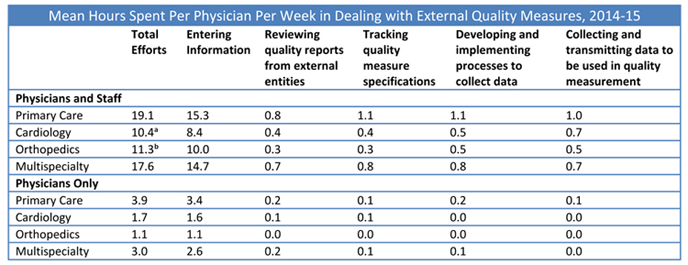 Donald Berwick, MD, senior fellow at the Institute for Healthcare Improvement (IHI) (and a former CMS administrator) described nine steps to advance healthcare into “the moral era” at an IHI forum in December, 2015. One of those steps was to “stop excessive measurement.” Dr. Berwick said:
I don’t mean that we should stop measuring. Indeed, I celebrate transparency in every form. How else can you learn? But we need to tame measurement. It has gone crazy. Far from showing us our way, these searchlights training on us, they blind us. ... I vote for a 50 percent reduction in all metrics currently being used.
Many anesthesiologists and pain physicians will agree that quality measurement has gone over the edge. The ASA’s Anesthesia Quality Institute (AQI) has adopted 22 measures and has identified 26 official Physician Quality Reporting System (PQRS) measures that can be reported by anesthesiologists and/or pain physicians. In proposing 48...
Donald Berwick, MD, senior fellow at the Institute for Healthcare Improvement (IHI) (and a former CMS administrator) described nine steps to advance healthcare into “the moral era” at an IHI forum in December, 2015. One of those steps was to “stop excessive measurement.” Dr. Berwick said:
I don’t mean that we should stop measuring. Indeed, I celebrate transparency in every form. How else can you learn? But we need to tame measurement. It has gone crazy. Far from showing us our way, these searchlights training on us, they blind us. ... I vote for a 50 percent reduction in all metrics currently being used.
Many anesthesiologists and pain physicians will agree that quality measurement has gone over the edge. The ASA’s Anesthesia Quality Institute (AQI) has adopted 22 measures and has identified 26 official Physician Quality Reporting System (PQRS) measures that can be reported by anesthesiologists and/or pain physicians. In proposing 48...
2650 Hits