eAlerts
-
The More Things Change...
Welcome to the post-Covid era. Do we even know what that means? Vaccines were supposed to bring an end to the worldwide pandemic, but now the Delta variant has ushered in a new wave of infections. Now we are all talking about breakthrough cases and boosters. It appears Covid is here to stay. In many ways, this is a metaphor for the challenges we face in managing anesthesia practices. As the French always say, “Plus ça change, plus c’est la même chose.” The more things change, the more they stay the same. We constantly bounce back from the general to the specific.
With this issue of the Communiqué, we have striven to poll some of the most respected industry experts for their take on today’s challenges and opportunities. As always, we hope their insights and perspectives will help you craft a productive strategy for your practice.
We begin with our team’s update and advisory for what you can expect from the MIPS program next year. You will note that even though MIPS is scheduled to be phased out in five years, like Covid, it won’t end. We are all eager to learn what the MIPS Value Pathway will entail.
No one is better qualified to sort out the issues related to the buy-versus-make decision than our very own Bellinger Moody. His is a very enlightening discussion of in-house billing options versus outsourcing. It is very important to follow his logic to appreciate why outsourcing will better allow you to manage the cost, minimize the risks and maintain control of your practice.
 As an experienced healthcare attorney, Mark Weiss provides an interesting perspective on the challenge of the disruptive physician. It is a useful reminder of the importance of collaboration and teamwork. Kelly Dennis shares some of the insights from her years of experience as an auditor in an interesting piece that reinforces for us just how important good clinical documentation and accurate coding are in revenue cycle management. Her piece has some very appropriate reminders for all of us, including just how tricky anesthesia billing can be.
As an experienced healthcare attorney, Mark Weiss provides an interesting perspective on the challenge of the disruptive physician. It is a useful reminder of the importance of collaboration and teamwork. Kelly Dennis shares some of the insights from her years of experience as an auditor in an interesting piece that reinforces for us just how important good clinical documentation and accurate coding are in revenue cycle management. Her piece has some very appropriate reminders for all of us, including just how tricky anesthesia billing can be.Our own Jody Locke pulls the lens back to put some of the specialty’s recent developments in perspective. His historical perspective is good salve for the challenge of change. Too often, our sacred cows become our greatest impediment to survival.
Finally, we tap into the vast repertoire of experience that Will Latham brings to the table. Test yourselves: how many of Will’s boxes of success do you check in your practice? It is always good to learn from experts. As always, we welcome your comments and thoughts on our selection of topics. Feel free to let us know what are the hot topics in your world. We always strive to make this as productive a dialogue as possible.
With best wishes,
Tony Mira
President and CEO -
In-House or Outsource? The Proverbial Quandary
Compelling Considerations for OutsourcingBellinger Moody, RHIA, CPC
Chief Compliance Officer, MiraMed Global Services, Inc., N. Augusta, SCThe question of whether to outsource your anesthesia billing and revenue cycle management (RCM) operations or keep the processes in-house is one pondered by many anesthesia providers and practice managers. Approximately ten years ago, the decision-making process to keep your billing in-house would not have required anywhere near the considerable process analysis, risk assessment and thought that must be considered in today’s anesthesia billing environment. The right answer as to whether or not to outsource is contingent upon many factors: (1) cost; (2) risk/liability; (3) control; (4) return on investment; (5) size of local labor market; (6) state of your practice’s financials; and, in some instances, (7) age of your business. Consequently, the three most heavily weighed factors are cost, risk/liability, and control. As a result, the focus of this article will be on those three factors.
Cost
It is common knowledge that in-house billing expenses associated with recruiting, training and retaining quality anesthesia billers and coders, paying their salaries, covering their benefits, as well as leasing or purchasing billing software platforms, are higher than those associated with outsourcing to a third-party billing company. Typical anesthesia billing and revenue cycle management costs include:
- Labor/Anesthesia Billing Staff: annual costs include median salary, healthcare, federal and state taxes, training to keep updated on anesthesia billing industry changes
- Office Space & Supplies: monthly costs for office space, statement paper, general office supplies, office hardware and other miscellaneous costs
- Software and Hardware: upfront cost and/or monthly leasing cost of software system for billing, practice management software, and computer and printer hardware costs
- Direct Claim Processing: monthly clearing house fees
Most national anesthesia billing companies have their own proprietary software platforms (for which costs are lower due to the fact that many have been in place for some time and the only common costs are maintenance and updates, over which they have control). In addition, the volume of claims processed by national anesthesia billing companies is usually considerably higher than a practice that performs its own billing. Consider also that many vendors such as clearing houses, statement companies, office supply companies, healthcare insurers, etc., provide discounted rates to large national RCM firms, which typically translates into lower overall business costs. Based on a five-year data sample obtained from practices that have transitioned from in-house billing to MiraMed subsidiary Medac, anesthesia practices spend between 6.5 percent to 11 percent of their collections to perform their own in-house billing. Outsourcing anesthesia billing reduces that cost—often significantly—as there is no need for billing staff or space for a billing department.Another significant cost consideration is that of compliance. With frequently changing regulations and new laws enacted on at least an annual basis, compliance costs have increased exponentially. The most significant contributor to increased compliance cost is data security. As evidenced by the recent data breach experienced by insurance giant Anthem (previously Wellpoint) in February 2015, security of PHI (personal health information) is a significant challenge for all covered healthcare entities. Another contributor to increased compliance cost is security and protection of patient credit card information. The major threat of data breaches posed by hackers (cybercrime) has created these increased costs, which include: hardware, software, ongoing education and training, policy implementation for internal controls, and testing.
Risk/Liability = Compliance
The last 15 years have seen the most significant changes in healthcare law. With new or enhanced healthcare legislation such as: (1) Information Transparency and Personal Data Control Act (ITPDCA); (2) 21st Century Cures Act Information Blocking Rule; (3) ACA (Affordable Care Act), Enforcement of HIPAA’s Administration Simplification Portion; (4) HITECH Act (Health Information Technology for Economic and Clinical Health Act); (5) TCPA (Telephone Consumer Protection Act); (6) FERA (Fraud Enforcement Recovery Act); (7) MMA (Medicare Modernization Act Section 306); (8) DRA 2005 (Deficit Reduction Act of 2005); (9) TRHA Section 302 (Tax Relief and Health Care Act Section 302); as well as (10) the expansion and creation of new government agencies and contractors such as RACs (Recovery Audit Contractors), MICs (Medicaid Integrity Contractors), and ZPICs (Zone Program Integrity Contractors). The cost involved with doing your own anesthesia billing has skyrocketed, and the compliance risks have more than tripled.
Although cost and control are significant factors to consider when weighing in-house billing vs outsourcing, the single biggest threat for billing entities today is compliance. Healthcare fraud and abuse enforcement is still at center stage as a huge money-maker for the government. The 2014 HCFAC (Health Care Fraud and Abuse Control Program) Report revealed that the government is making $7.7 for every dollar they spend in this area. As such, it should come as no surprise that the Department of Justice (DOJ) issued an Interim Final Rule on June 30, 2016 that doubles the amount of penalties under the False Claims Act (FCA) and the Anti-Kickback Statute (AKS).
The current penalties range from $5,500 – $11,000 per false claim. However, effective August 1, 2016, FCA penalties increased from a minimum of $10,781 per claim to a maximum of $21,563 per claim and the AKS penalties increased to $21,563 per occurrence. The DOJ allowed a comment period that ended on August 29, 2016; however, due to abstinence by congress, these penalties under the FCA and AKS have doubled.
Clearly, healthcare fraud and abuse are still major compliance risk areas; however, we no longer exist in a billing environment where regulatory billing compliance is the only major compliance risk factor. The days of anesthesia compliance professionals worrying mostly about whether anesthesia services were appropriately documented, coded, billed and collected (in accordance with OIG, DHHS, federal payer and third-party payer policies and guidelines) are long gone. Healthcare compliance professionals have identified data security as the single most formidable compliance risk area for healthcare organizations, healthcare providers, payers and billing entities. The two major data security risk areas:
- PHI (Personal Health Information) Data Security/Compliance: With cybercrime and hacking at all-time highs, data security is now considered to be the single most critical compliance risk area by healthcare compliance professionals. In fact, the current cybercrime environment has created the justifiable need for a totally new senior level executive position — CISO (chief information security officer). The CISO is a senior-level executive responsible for aligning security initiatives with enterprise programs and business objectives, ensuring that information assets and technologies are adequately protected. Salary.Com reports that the median annual chief information security officer salary is $196,027, as of August 29, 2016, with a range usually between $164,816-$237,026. However, this can vary widely depending on a variety of factors. The question you may now be pondering is “can I really afford a CISO?” The real question you should be pondering is “can I afford NOT to have a CISO?” The HITECH Act sets federal penalties on healthcare companies that leak data on 500 patients or more as high as $1.5 million per incident. For all other industries, the Health Insurance Portability and Accountability Act imposes stiff civil and even criminal penalties for those responsible for data breaches. So, why are these penalties for breaches of personal health information so high? According to a September 24, 2014 article published in Technology News, by Caroline Humer and Jim Finkle, “your medical information is worth 10 times more than your credit card number on the black market.” Personal health information contains names, birthdates, policy numbers and medical record numbers that may contain social security numbers as a part of their nomenclatures. The bottom line is that fraudsters are much more attracted to PHI than financial information because of the opportunity for identity theft. Why steal credit card information when they can steal your identity? Cybercriminals are selling this information on the black market at a rate of $50 per patient chart. The question most anesthesia in-house billing operations must now also weigh is whether they want to take on the added risks and costs associated with maintaining and securing PHI or pass the overwhelming majority of that risk on to an outsourced billing business partner that has the infrastructure, resources and controls to better assume these risks.
- Payment Card Industry Data Security Standard Compliance: The Payment Card Industry Data Security Standard (PCI DSS) is a proprietary information security standard for organizations that handle branded credit cards from the major card companies including Visa, MasterCard, American Express, Discover and JCB. The PCI Standard is mandated by the card brands and administered by the Payment Card Industry Security Standards Council. The standard was created to increase controls around cardholder data to reduce credit card fraud. Validation of compliance is performed annually, either by an external qualified security assessor (QSA) or by a firm-specific internal security assessor (ISA) that creates a Report on Compliance (ROC) for organizations handling large volumes of transactions, or by a Self-Assessment Questionnaire (SAQ) for companies handling smaller volumes. Validation of PCI DSS compliance is an area that many in-house and smaller billing entities neglect; however, if a credit card breach occurs (e.g., by hacking or a dishonest employee), this validation could mean the difference between hundreds of dollars in fines, millions of dollars in penalties and damages, or even prison time. Once again, this is now another major compliance risk area that must be weighed when deciding whether to keep the billing in-house or outsource.
Control
Many providers and administrators like having hands-on control of financial operations through in-house billing. Much of the anxiety about relinquishing control centers around five key areas: (1) collections performance; (2) compliance; (3) appropriate staffing; (4) accessibility/proximity; and (5) A/R management. All of these anxieties may be addressed contractually with collections performance and A/R management guarantees and clauses, staffing guarantees, as well as auditing requirements to ensure compliance. Some billing companies are even willing to reduce your monthly fee and reallocate the funds toward an external auditor of your choice. Additionally, as with most outsourced billing agreements, billing companies are contractually obligated to follow up on all unpaid and denied claims.Due to rapid advancements in technology, accessibility and/or proximity fears have become less and less significant in the decision-making process. Many national outsourced anesthesia billing companies supply you with comprehensive performance reports—on demand—via web portal, and/or upon request. This capability provides unparalleled visibility into your billing operations without requiring you to micromanage—or even oversee—any staffers. Comprehensive reports are wonderful; however, having access to information and images all the way down the individual patient account level is absolutely vital. Specifically, having individual patient account web-portal access to view: (1) images (i.e., EOB, anesthesia record, patient demographic, claim form); (2) billing and coding information (i.e., patient name, insurance company name, CPT codes, anesthesia start and end time entered in the system, etc.); (3) line item account transactions and postings (i.e., payments, adjustments, credits, etc.); (4) unpaid and underpaid claims follow-up activity notes; (5) unpaid patient balance follow-up activity/notes; and (6) patient statement activity/notes provides you with total transparency. You now have all the necessary tool to instantly audit your outsourced billing company. Total patient account transparency is one of the most important considerations in the decision-making process when weighing the control factor. Last, but not least, proximity issues may be contractually addressed by requiring billing company presence at monthly or quarterly group meetings.
Conclusion
As previously mentioned, cost, liability and control are commonly the most heavily weighed factors when deciding whether to outsource your anesthesia billing operations. Aside from clinical services, billing and revenue cycle management are the most important processes of your practice. Your cash flow depends on them, so the decision of how to handle these services should not be taken lightly. You should do assessments of your practice’s costs, risks, staffing and volume metrics to determine what is right for you.Although cost and control are two primary factors that must be carefully assessed, in the current healthcare fraud and abuse/cybercrime environment, I cannot emphasize enough how absolutely critical it is—now more than any other time in your practice’s history—that you more thoroughly assess your practices’ liability/risk (in relation to these two areas) in weighing your decision to outsource.
Finally, it is important for anesthesia practices/providers to factor in their individual costs and preferences when deciding whether or not to outsource. In an apples-to-apples comparison, most are now determining that outsourcing is their best option from a cost perspective. However, as stated throughout this article, cost is NOT the only issue anesthesia practices should consider. There are many other factors involved in this business decision that may be as important as cost. You must weigh all factors to determine which option is best for your practice.
Bellinger Moody, RHIA, CPC is Chief Compliance Officer for MiraMed Global Services. With over 30 years of experience in the healthcare industry and 25 years of experience in anesthesia and pain management billing, coding, reimbursement, education and management, Mr. Moody is a nationally recognized expert in the industry. Prior to this position with parent company, MiraMed Global Services, Moody served as Chief Compliance Officer, CEO and President of MiraMed subsidiary Medac. Mr. Moody has a Bachelor of Science in Business Administration from Morehouse College. He is a nationally Registered Health Information Administrator (RHIA) through the American Health Information Management Association (AHIMA), a nationally Certified Professional Coder (CPC) through the American Academy of Professional Coders (AAPC), a nationally Certified Compliance Professional (CCP) through the Healthcare Fraud & Abuse Compliance Institute, an AAPC Approved Professional Medical Coding Curriculum (PMCC) Coding Instructor and a member of the Medical Group Management Association (MGMA). He can be reached at bellinger.moody@miramedgs.com.
-
Both New and Seasoned Coders Should Know the Many Risk Areas in Anesthesia Coding
Kelly Dennis, MBA, ACS-AN, CANPC, CHCA, CPMA, CPC, CPC-I
Perfect Office Solutions, Inc., Leesburg, FLThe American Medical Association’s (AMA’s) 2021 CPT® codebook will likely be released without specific anesthesia-related code changes for the coming year, although coders will need to be aware that 2023 may bring substantial changes to the way postoperative pain management is reported. As there are no anesthesia-specific coding changes to consider for 2022, it is always a suitable time to review anesthesia coding basics and frequent coding problem areas.Anesthesia services represent a small portion of CPT, but correct anesthesia coding requires complete comprehension of various anesthesia guidelines. Services reported by anesthesia providers are not limited to anesthesia codes 00100-01999; and instructions found in the CPT Anesthesia Guidelines do not cover many of the coding nuances specific to anesthesia billing [for instance, coding for the services of a Certified Registered Nurse Anesthetist (CRNA) or an Anesthesia Assistant (AA), which may also be referred to as a Certified Anesthesia Assistant (CAAs)]. Additional coding resources are required to gain a better understanding of anesthesia coding.
CMS and NCCI Offer Anesthesia Resources
The Centers for Medicare & Medicaid Services (CMS) and the National Correct Coding Initiative (NCCI) each publish information regarding anesthesia coding regulations. Although not all insurance companies follow CMS and/or NCCI guidelines, many use interpretations of both guidelines. Both publications are available through the Anesthesiologist Center of the CMS website, resourced at the end of this article.
The CMS Internet-Only Manual (IOM) provides guidelines for both anesthesiologists (Section 50 – Payment for Anesthesiology Services) and CRNAs (Section 140 – CRNA Services). Although CAAs are not specifically mentioned in the chapter heading under CRNA, the guidelines were revised more than 19 years ago (in 2002) to include anesthesia assistants. CMS recognizes both CRNAs and CAAs as non-physician practitioners (NPPs) and other insurances or resources may recognize these providers as a Qualified Health Professional (QHP). Commercial insurances typically do not make a distinction between the two anesthetist types with regard to payment for services provided under medical direction of an anesthesiologist. Coders may also find that insurances do not separately recognize these types of anesthesia clinical staff. It is enough to keep practices on their toes!
Although many practices are familiar with the care team approach which includes anesthesiologists and CRNAs, fewer may be familiar with CAAs. As of June 2019, CAAs are licensed in fourteen states with delegatory authority in two additional states and also are recognized under the TRICARE system. One important distinction between CRNAs and CAAs (depending on state scope of practice, delineation of privileges by the facility and individual malpractice carrier requirements), is that CRNAs may be allowed to practice as nonmedically directed, whereas a CAA must be medically directed.The most up-to-date version of the NCCI (as of this writing) is 27.2, which became effective July 1, 2021. Anesthesia guidelines are found in Chapter Two. These guidelines for anesthesia coding are much more in-depth than CPT guidelines and include an introduction to correct coding for anesthesia and information regarding which services are bundled. For example, time spent during the usual pre- and post-operative visits, patient monitoring and various other activities are bundled into the base value of anesthesia services.
NCCI also discusses which services are billable separately. Separate procedure services, such as insertion of an arterial line [36620 Arterial catheterization or cannulation for sampling, monitoring or transfusion (separate procedure); percutaneous], Swan-Ganz catheter [93503 Insertion and placement of flow directed catheter (e.g., Swan-Ganz) for monitoring purposes], and a central venous pressure line (36555 Insertion of non-tunneled centrally inserted central venous catheter; younger than 5 years of age and 36556 Insertion of non-tunneled centrally inserted central venous catheter; age 5 years or older) are payable separately to anesthesiologists, as well as to CRNAs/ CAAs if these procedures are furnished within the parameters of state licensing laws. The NCCI also provides examples of coding scenarios regarding postoperative pain management, ventilation management, and discontinuous time. The postoperative pain management example explains factors to help coders determine when postop pain is considered outside of the global surgical package. According to the CPT Editorial Summary of Panel Actions, May 2021, coders should expect “Accepted revision of codes 64415, 64416, 64417, 64445, 64446, 66447, and 64448 to include ultrasound guidance, when performed” to become effective in January 2023.
Armed with the knowledge gleaned from these published anesthesia resources, you can gain valuable insight into information available to insurance companies. Keep in mind, however, that it is up to individual payers to determine which guidelines to follow. For example, many payers follow guidelines set forth in the American Society of Anesthesiologists (ASA) Relative Value Guide® (RVG).
Be Watchful of Payer-Specific Guidelines
Anesthesia coders should understand that anesthesia coding and billing guidelines will change from state to state and from payer to payer. Although CMS loosely follows the same IOM guidelines across all states, each Medicare administrative contractor (MAC) has its own idiosyncratic payer rules. This also is true for Medicaid, Blue Cross/Blue Shield (BCBS) and worker’s compensation. Individual payer contracts often include verbiage indicating their specific billing policies should be followed, yet they may or may not provide a copy of their coding/ billing policy. The best rule of thumb when there is not a policy is to follow the ASA RVG guidelines and use this resource in the event an appeal is necessary.One of the best ways to ensure your practice is following individual state- and payer-specific anesthesia guidelines is to research which guidelines are available from your practice’s payers. The internet has made it easy to access information, although other sites may require provider login information (e.g., Blue Shield of California). If the information is not provided or accessible, it should be requested and reviewed on an annual basis, at a minimum. The onus for keeping up to date with changing regulations is placed solely on the anesthesia provider— who, in turn, typically relies on his or her coding and billing staff to know when changes occur.
Communicate Potential Risk Areas wit h Clinical Staff
Risk areas for anesthesia providers usually are understood by the coding and billing staff yet are not always relayed to the clinical staff. Coders understand the doctrine, “If it wasn’t documented, it didn’t happen.” With anesthesia records, however, sometimes it is very difficult to determine the exact diagnosis and procedure code and/or who actually provided services.
For example, if the anesthesia record has a check box for placement of an arterial or central venous pressure (CVP) line, and both an anesthesiologist and CRNA or CAA are involved in the case, a check mark doesn’t indicate clearly who placed the arterial line or CVP. Because some carriers may require services to be filed under the name of the provider who performed the service, the service may go unbilled unless clear procedure notes are documented either in the Remarks or Comments section or provided on a separate procedure form.
Another risk area is medical direction criteria. Many anesthesiologists fail to sign or initial their participation appropriately with a teaching or a medically directed case and may consider their signature as sufficient documentation of involvement. CMS and other payers require documentation during the most demanding procedures in the anesthesia plan, which includes induction and emergence, when applicable. Unless a monitored anesthesia care (MAC) case converts to general, induction and emergence are not applicable in such cases. Similarly, there is not an induction or emergence period associated with regional anesthesia.Time Really Can Be Relative
Time reporting on claims may vary, and there is no national guidance that may be applied to all payers. According to the CPT Anesthesia Guidelines, time units are reported as is “customary in the local area.” Although Medicare requires exact time reporting, other payers may request either rounded time, or time in units, rather than minutes. Anesthesia providers always should provide exact start and stop times on the anesthesia record that, according to the ASA, correlate with their definition, last updated in 2019, as follows:
“Anesthesia time is defined as the period during which an anesthesia practitioner is present with the patient. It starts when the anesthesia practitioner begins to prepare the patient for anesthesia services in the operating room or an equivalent area and ends when the anesthesia practitioner is no longer furnishing anesthesia services to the patient, that is, when the patient is safely placed under postoperative care. Anesthesia time is a continuous time period from the start of anesthesia to the end of an anesthesia service. In counting anesthesia time for services furnished, the anesthesia practitioner can add blocks of time around an interruption in anesthesia time as long as the anesthesia practitioner is furnishing continuous anesthesia care within the time periods around the interruption.”
Coders should not expect to see large or unexplained gaps of anesthesia time around either the start or stop times, or times that routinely end with a “0” or “5.” Internal reviews of anesthesia times should be performed periodically to ensure your practice is checking this compliance risk area at a minimum! Because there are so many risk areas in anesthesia coding, it is necessary to understand the importance of following payer guidelines and keeping up to date with changes regularly.
If you see risk areas in your practice, work closely with your anesthesia clinical staff to ensure correct coding, documentation and billing. Keep in mind that although there may not be expected anesthesia specific code changes this year, the RVG may contain changes to either parenthetical notes or other information. Make sure you check the Summary of Changes found at the beginning of the book when you receive your 2022 RVG.
Resources:
https://www.ama-assn.org/about/cpt-editorial-panel/summary-panel-actions
https://www.cms.gov/Center/Provider-Type/Anesthesiologists-Center?redirect=/center/anesth.asp
https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf
https://aaaa.memberclicks.net/assets/AAAA%20Work%20States%20Map%20June%202019.pdf
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I has over 36 years of experience in anesthesia coding and billing and speaks about anesthesia issues nationally. She has a Masters Degree in Business Administration and is a certified coder and instructor through the American Academy of Professional Coders. Kelly is an Advanced Coding Specialist through the Board of Medical Specialty Coding and served as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November 2001. She can be reached at kellyddennis@attglobal.net.
-
Popularity Contests and Disruptive Physicians: Avoiding the Death of Your Anesthesia Group
Mark F. Weiss, JD
The Mark F. Weiss Law Firm, Dallas, TX, Los Angeles and Santa Barbara, CAAs humans, we’re primed by evolutionary forces to fear the loss of something much more than we value an equivalent gain.That’s why many anesthesia group leaders are concerned that market and other pressures will have a significantly negative impact on their group. From competition from other groups, to the failure of the hospital, to the difficulty to recruit and retain, these and other concerns actually do keep you up at night.
But while medical group leaders are keenly focused on the dangers from the outside, there are dangers lurking inside groups, as well, just as dangerous, or maybe even more so.
Dr. Stacy
You recruit Dr. Stacy because of the sterling CV. College in Cambridge, medical school in Cambridge (the other one), and trained at an even more famous place at the elbow of a Nobel laureate.
And then six months later, you learn that Stacy might just be a pathological a-hole. Stacy badmouths your group to the hospital CEO. Stacy questions your leadership abilities in the cafeteria, but never in a conference room with you present. Stacy works with your competitor to undermine your group. Stacy screams at nurses. Yes, these are all real-life examples of real-life Stacy, an amalgam of Stacies, of course.
It’s important to distinguish your Stacy, the poster child for disruptive physicians, from a simple nonconformist. Nonconformists aren’t trying to take your group down. Nonconformists aren’t conspiring against your leadership or the group’s future. As they say, they simply march to the beat of a different drummer.
Perhaps they’re a little bit challenged as to the concept of personal space. Perhaps they’re not exactly politically correct. Perhaps they never stop challenging how and why things are done; and, when you tell them, they question the “why” underlying that. Responses such as “it’s always done that way,” or “because it’s a ‘best-practice,’” aren’t ultimate “whys.” Sometimes there is no ultimate “why,” or, at least, one that makes any real sense.Despite their ability to drain, nonconformists can easily be contained and even harnessed to the group’s benefit. Seen for what it can truly be, nonconformity is an asset, a cross-pollinator of ideas and of ways to think. It’s a Darwinian stressor. Yes, some extra supervision might be required to keep the nonconformity positively channeled.
Unfortunately, there’s no blood test or imaging procedure that diagnoses the difference between nonconformist and disruptor. But, fortunately, disruptive physicians leave snail-like trails. Before jumping to the conclusion that your Stacy is a disruptor, pause and question motives while you’re examining evidence. Is it truly disruptive action that should lead to termination, or is it, instead, nonconformity that can be made to be beneficial to your group’s success?
Thirty-Three Strikes and You’re Out
Let’s assume that you’ve gone through that process and determined, wisely in this case, that Stacy is a disruptor. What then?
Benjamin Franklin is said to have quipped that house guests and fish smell after three days. Crappy group members stink a lot faster than that.
Sure, it’s all PC to “counsel” these guys, to tell them how much you love them if only they will toe the line and be good boys or girls and get along with everyone while singing Kumbaya. Go ahead, try it once. But after that, realize that these people just can’t help themselves. In your group they are a rot that will spread. In some other setting, they may be perfectly happy, highly productive good citizens. Do them a favor and get them started on their journey to find their perfect spot: it is somewhere else.
But can you do that? What do your group’s organizational documents and any agreement between the group and Stacy provide? Here’s where double, double, toil and trouble often sets in.
The Popularity Contest or “But, Everyone Likes Dr. Stacy”
Due to the mindset that medical groups are more like clubs of colleagues than business organizations, many groups build club-like protections into their documents, from partnership agreements to employment and independent contractor agreements. They define “for cause” termination narrowly and (and here’s the killer) build in “protections” for the subject physician as opposed to for the group—generally expressed as a required percentage vote of the group’s members before anyone can be expelled.The higher the percentage, the greater the “protection” . . . and the greater the problem. Your Stacy is killing your business, but so many of the group members like Stacy, maybe even love Stacy (or are very afraid of Stacy), that it’s impossible to get the required percentage vote. Protecting your group is not supposed to be, and should not be, a popularity contest. Accordingly, protecting your group from a disruptive physician starts well before you have one. It begins with an analysis, and perhaps a restructuring, of your group’s organizational and employment-related documents.
Are all member vote requirements themselves disruptive? No, but they must have limited application or else they end up serving a purpose that was never intended, the destruction of the group as opposed to the preservation of a single physician’s future with the group.
We can look at this one last way. Empower those selected to lead the group to actually lead the group. If you don’t like their leadership, remove them from office, but don’t tie their hands while they are in office because, in the end, you might just be binding the hands of your own future.
Mark F. Weiss, JD is an attorney specializing in the business and legal issues affecting physician groups and healthcare facilities on a national basis, practicing at The Mark F. Weiss Law Firm, with offices in Dallas, Texas and Los Angeles and Santa Barbara, California. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine. He can be reached by email at markweiss@weisspc.com.
-
The Ebb and Flow of Anesthesia Practices
Jody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services
Anesthesia Business Consultants, LLC, Jackson, MIEmpires come and go. None last forever. The story of the twentieth century has been the unraveling of the British Empire. When the century began, the United Kingdom presided over India, and now India is the largest democracy in the world, while Britain is a pale shadow of its former self. Germany once represented itself as the Third Reich under Adolf Hitler; but, ironically, today’s unified Germany under Angela Merkel is even more powerful and sustainable. History is the study of organizations struggling to fit their political, economic and social context. It is an ever-evolving process, but it is not limited to countries and governments. The aggregation of American medicine is following some very traditional patterns. Once prominent and powerful entities often succumb to a new market order.Why should this be any different in the world of anesthesiology? The past forty years have seen a dramatic transformation of the specialty as individual providers have banded together into group practices and then sought to grow their empires into even larger regional or national provider organizations. Sheridan Anesthesia was once a private anesthesia practice in south Florida before it became the national organization. Now it has merged with Emcare to become Envision. Who can know what its next metamorphosis will be?
If there is one thing that has changed over the past forty years it is the impact of market forces on the specialty. Amr Abouleish, MD often reminded his audiences that . . .
Healing is an art Medicine is a science Healthcare is a business.
As Nikita Khrushchev once said: “Economics is a discipline that does not respect one’s wishes.” And so we see the same struggle in the specialty of anesthesia to find organizational structures that will meet the needs of the local market.There is a tendency to refer to practices that go out of business as failed practices, but this is neither fair nor accurate. Hospitals with operating rooms cannot function without anesthesia providers. Even if a group practice cannot meet the needs of the facility in its current form, the facility must ultimately figure out another solution. However traumatic this transition may be, it is just that—a transition.
Sometimes what is perceived as a traumatic juncture in the lifecycle of an anesthesia practice is simply a failure of imagination and an unwillingness to metamorphose into an entity that meets the new market realities. Too often this is an unwillingness to let go of long-held sacred cows. We often say that the only constant in American medicine is change. When it comes to the practice of anesthesia this is the reality.
Let us consider three of the most common sacred cows that have ultimately undone many anesthesia practices.
- Anesthesia providers only create value when they are giving anesthesia. Many practices are still coming to realize the value of professional management.
- Physician-only anesthesia is preferable to a careteam model. Even though 75 percent of all anesthetics are administered by a team of physicians and CRNAs, many practices—especially in the west—continue to cling to a physician-only model.
- The success or failure of an anesthesia practice is a function of the quality of care provided. The reality is that quality of care is a given, what matters most is the quality of service provided to the customer.
Political Realities
Not only has the pharmacology of anesthesia evolved significantly, and not only has the scope of the typical practice continued to change dramatically, but the very nature of anesthesia practice has undergone a paradigm shift. The majority of today’s group practices are less than 40 years old. Many practices were effectively shotgun marriages intended to meet the contractual requirements of hospitals and payers. Ultimately, some practices were organized on tighter and more unified models than others. For many, though, especially those with complicated internal productivity compensation plans, the new entities remain more confederations of competing providers than truly integrated business entities.It used to be that if anesthesia providers were clinically busy and the payer mix was adequate, they could generate sufficient professional fee income to maintain their independence. It was commonly thought that if a provider could consistently bill 50 ASA units per location day there was no need for financial support. Over the past ten years, the specialty has experienced a tectonic shift that is the result of three main factors: a proliferation of anesthetizing locations as cases have migrated from traditional inpatient venues to all manner of outpatient venues; a resulting decline in provider productivity as measured in average units generated per location day; and a gradual, but inexorable, erosion of the average yield per billed unit as Medicare and Medicaid represent an ever larger percentage of the payer mix. Given these powerful factors, it has become increasingly challenging to meet the income expectations of providers. The greatest challenge of most of today’s anesthesia practice is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the service requirements of the facilities they serve. The current perception is that there is a shortage of providers.
All of this has changed the politics of anesthesia. When anesthesia was a free good to the hospital, contractual relationships with facilities were much simpler. When an anesthesia group evolves from a no-subsidy practice to a subsidy practice, it changes the very nature of the relationship. The request for financial support now focuses on the value proposition being negotiated. Where once a group president could sit down with the CEO of the hospital and hammer out a deal, now the process often involves an extensive and expensive process that frequently requires consultants to evaluate the fair market value (FMV) of the practice.
The complexity of such negotiations has inevitably resulted in a much more political process. It used to be that hospital administrators were more willing to accept quirky anesthesia practice behaviors long as patients were treated well and had good outcomes. Most administrators never really gave much thought to other anesthesia service options. The new reality is completely different. It is the reality of the RFP (request for proposal). No three letters evoke such fear in the minds of anesthesia providers. The advent of a proliferation of RFPs means that administrators are now evaluating the current solution as compared to market options.
Anesthesia departments were typically staffed by providers who chose to live in a particular community. Groups were often comprised of like-minded providers who had been recruited to be part of a team. In most situations the hospital communicated with a group president who enjoyed the respect of the members. Many of these leaders enjoyed long tenures as the leader. So what changed? Anesthesia practices started to grow and merge. Many sought experienced anesthesia administrators. In 1994, the American Society of Anesthesiologists (ASA) held its first Practice Management conference in Phoenix, a fact that demonstrated a growing concern for the management challenges facing the specialty. Increasingly, it became clear that it would take more than good care and consistent outcomes to ensure the success of an anesthesia practice. Hospital and managed care contracting were becoming the hot topics of the day.This growing awareness of the practice management challenges facing the specialty and a desire to exert leverage in their contract negotiations was not always well received by hospital administrators. The politics of medicine started to play itself out. Some practices were astute in managing their relationship with administration, others were not. It is often said that managing a suite of operating rooms effectively is like sitting on a three legged stool where anesthesia is one leg, the surgeons are another leg and administration is the third leg. Historically, hospitals have aligned themselves with the surgeons and done everything possible to encourage their loyalty, which has resulted in some very unprofitable coverage requirements for anesthesia. Anesthesia has more and better data about what happens in the operating rooms. Many in the anesthesia community started suggesting that anesthesia should play a much more significant role in managing the operating rooms and enhancing the profitability of hospitals. Although the potential of this advantage has yet to be fully realized, it is a card that practices are starting to play to align themselves with administration.
Every anesthesia practice has its challenges. Practices that can align themselves with administration in a collaborative problem-solving mode enjoy far more support from administration. Unfortunately, many are not so savvy. Money is often the straw that broke the camel’s back. If administration does not view the anesthesia practice as a reasonable business partner, the relationship is doomed. The list of anesthesia practices that have succumbed is growing. The irony of this situation is that while the current group may have gone out of business, the hospital still needs anesthesia providers.
Economic Realities
Anesthesia is an increasingly expensive service to provide. The burdened cost of a physician anesthesiologist can be as much as $500,000 per year. Many CRNAs get paid at least half that. There is no such thing as a local market any more. Anesthesia providers tend to migrate to practices with the best compensation and the most reasonable call requirements, no matter where they are located. It is a provider’s market. The migration of cases to ambulatory facilities has only exacerbated the challenge as anesthesiologists move from traditional hospital practices with a full call requirement to ambulatory centers where they only have to work Monday through Friday, with no nights or weekends.Unfortunately, too many hospital administrators do not fully appreciate the economics of anesthesia. The profitability of an anesthesia practice is ultimately a function of one thing: the profitability of coverage. There is a cost for each anesthetizing location that must be staffed. It may represent the cost of an anesthesiologist divided by the number of days he or she works a year as in the following example.
If the total cost of a physician is $475,000 and the provider works 227 days a year, then the cost per clinical day is $2,100. The question is how many actual days of work generate $2,100 in collections, net of overhead costs such as billing and management? Some practices can reduce this cost through a leveraged careteam model where a physician may medically direct three or four CRNAs. Even when this can be done successfully, it may not close the gap between the cost and the revenue per location day.
The chart shown below is a representative sample of the actual yields per clinical day of 15 client practices from across the country. It should be noted that none actually generate $2100 per day, which is why all practices must focus on reducing the cost of providing care.
A number of factors make this simple profitability calculation difficult to apply to the entire practice. Some venues are inherently unprofitable. Depending how busy OB is, this is often a particularly unprofitable service for anesthesia. Hospitals often want to launch new service lines that require additional staff, but which provide little additional fee for service income to the practice. Call requirements are particularly onerous. About 75 percent of the revenue generated per anesthetizing location is generated between 7 AM and 3 PM. Requiring a physician or CRNA to remain in house all night is always an expensive requirement. It does not really matter how profitable certain lines of business are if their profitability is diluted by other unprofitable lines.
Most hospitals were designed and built on the assumption that “if you build it, they will come.” The reality is that in the current environment, cases migrate to the most convenient and most cost-effective venues. In fact, what we are seeing is a growing schism between the traditional inpatient venues which have become dumping grounds for the most acute Medicare patients and the ambulatory facilities where generally healthier patients with good commercial insurance go.
Hospital subsidies are supposed to compensate the anesthesia practice for the financial loss they incur meeting hospital coverage requirements. This is not always a straightforward calculation. Changes in case volume, as were experienced in 2020 as a result of Covid-19, or eroding payer mix, often impact the calculation negatively. It is often said that it is easy to calculate the necessary subsidy today, but it will probably be wrong tomorrow. More often than not, hospitals try to put the risk for such fluctuations on the anesthesia practice.
Poor payer mix, i.e., too high a percentage of Medicare and Medicaid patients, and inadequate or eroding case volume are often cited as the reason why practices fail; and, while these factors may be real, it is important to remember that the hospital will still need anesthesia. Consider that perhaps the practice was too wedded to certain preconceived assumptions to explore other options. Many hospitals are now suggesting employment options that are anathema to private practice providers, even though the end result might ensure a more reasonable and predictable level of compensation and a better quality of life. As mentioned at the outset, most anesthesia practices are now facing the same set of economic challenges that impact their ability to recruit and retain qualified providers. While it is true that some practices enjoy more favorable locations than others, the big difference between those that remain viable and those that don’t is their ability to think outside the box and find creative solutions. Why is it that national anesthesia staffing companies such as Envision and NAPA keep growing? They come at the challenges with a different set of assumptions. They may have slicker responses to RFPs and a greater quiver of arrows; but, at the end of the day, their solution is not that much different. It is just delivered with more credibility.
Social Considerations
Anesthesia is unique in so many ways. The calculation of anesthesia charges and payments bears no relationship to that of any other specialty. Anesthesia providers are the only ones who get paid for the time they spend with patients as compared to surgeons who get a flat payment per procedure. Anesthesia groups have used this unique charge calculation to design some very creative compensation schemes. While not all practices pay their providers based on provider productivity, there are many that do, and this continues to be a defining feature of the specialty. Individual providers prefer to feel as though they are getting paid for every service they provide. And while this concept has made it possible for many providers to feel comfortable in a group practice, it is not always perceived as a positive by the rest of the OR staff. An OR nurse once commented that she could always tell how members got paid based on their behavior and their willingness or unwillingness to do certain cases.Clinically, anesthesia has many distinct characteristics. Each case is both art and science. The provider must assess the specific concerns of the patient, the needs of the surgeon, and their own experience with such cases. No two anesthetics for the same surgical procedure are the same. This fact alone encourages a kind of specialty autonomy. Starbucks strives to make every latte the same, no matter who prepares it or where it is delivered. This kind of thinking and what is often derided as “cookbook medicine” is anathema to anesthesia providers. And while groups will proctor new physicians for a short period when they are hired, once they are vetted, there is little or no oversight or guidance unless there are clinical issues. Anesthesia enjoys a long tradition of independent and autonomous clinical decision making that continues to influence how groups practice. A large group in Southern California once held a series of strategic retreats, the result of which was an agreement that the organization would be pre-eminent in matters of billing, contracting and human resource management, but that the individual providers would be completely autonomous in all matters clinical.
A former ASA president, Peter McDermot, MD was once quoted as saying, “Anesthesia group, that is an oxymoron; it is like herding cats.” And this is exactly what makes hospital administrators crazy. They want to know that the group speaks with one voice and that the group has the structure, commitment and tools to deal with outliers. It is no accident that virtually all professional service agreements now include language clarifying group disciplinary procedures and what it takes to remove problem providers.
This is one of the greatest challenges most groups face: disciplining their own. It has often been noted that most anesthesia practices are truly not business entities because they operate more as medical professional fraternities. The real problem is that, as American medicine becomes more competitive and as the cost of care becomes the primary focus of hospital administrations, it becomes increasingly important that business partners, such as the anesthesia groups, mirror the goals and objectives of the facility. Many an anesthesia group has lost its contract simply because it lacked effective and professional management. In fact, this has become one of the appeals of the large national anesthesia staffing companies. The perception is that they are run as professional entities.
One may also ask why so many hospital administrations are seriously considering employment models for their anesthesia providers even though this may ultimately result in a more expensive solution? The argument given is that employment equals control. This is no doubt a reaction to the perception that they simply need to find a different way to herd the cats.
There is a certain irony here. Ultimately, everyone wants control. Anesthesia providers want control of their own income and lifestyle. Hospital administrators want control of the anesthesia service so that it acts in concert with the other lines of business they manage. The reality is that all parties are at the mercy of market factors beyond their control. The truth is that no one actually has control. Anesthesia is a quintessential service specialty and must be prepared to respond to whatever volume and kinds of cases the surgeons bring to the facility. Let us just consider the impact of endoscopy, which now represents about 30 percent of most practice activity. The revenue potential of a practice is a function of OR utilization, payer mix, coding and billing policy changes, and payer pushback on what is starting to be deemed an over-used service. In the end, no one really has any control at all.
What it All Means
We have a saying at Anesthesia Business Consultants that “if you have seen one anesthesia group, you have seen one anesthesia group.” Each is a unique product of its history, the culture of the medical community and the specific requirements of the institution. Because of this, it is often perilous to generalize about the state of the specialty or its future. Historians like to remind us that history unfolds from the general to the specific. The issues identified above represent the general themes that have marked the evolution of the specialty. Each may play itself out to varying degrees in the context of a particular practice. Some practices inevitably are fortunate or savvy enough to avoid any of the downsides as they navigate the changes in the industry. The practices that fail or morph into some other format do so because the stakeholders were simply not the ones with a better solution.Each practice that ends up changing provides a useful case study and insight as to how and why the current approach and strategy did not sustain the practice. More often than not, the beliefs and strategies that got us to where we are today will not get us to where we want to be tomorrow. The best managers are serious students of the specialty. This is the lesson we must all take to heart. After all, anyone who suggests that managing an anesthesia practice is easy is a terrible liar or a terrible manager.
Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.
 As an experienced healthcare attorney, Mark Weiss provides an interesting perspective on the challenge of the disruptive physician. It is a useful reminder of the importance of collaboration and teamwork. Kelly Dennis shares some of the insights from her years of experience as an auditor in an interesting piece that reinforces for us just how important good clinical documentation and accurate coding are in revenue cycle management. Her piece has some very appropriate reminders for all of us, including just how tricky anesthesia billing can be.
As an experienced healthcare attorney, Mark Weiss provides an interesting perspective on the challenge of the disruptive physician. It is a useful reminder of the importance of collaboration and teamwork. Kelly Dennis shares some of the insights from her years of experience as an auditor in an interesting piece that reinforces for us just how important good clinical documentation and accurate coding are in revenue cycle management. Her piece has some very appropriate reminders for all of us, including just how tricky anesthesia billing can be. Most national anesthesia billing companies have their own proprietary software platforms (for which costs are lower due to the fact that many have been in place for some time and the only common costs are maintenance and updates, over which they have control). In addition, the volume of claims processed by national anesthesia billing companies is usually considerably higher than a practice that performs its own billing. Consider also that many vendors such as clearing houses, statement companies, office supply companies, healthcare insurers, etc., provide discounted rates to large national RCM firms, which typically translates into lower overall business costs. Based on a five-year data sample obtained from practices that have transitioned from in-house billing to MiraMed subsidiary Medac, anesthesia practices spend between 6.5 percent to 11 percent of their collections to perform their own in-house billing. Outsourcing anesthesia billing reduces that cost—often significantly—as there is no need for billing staff or space for a billing department.
Most national anesthesia billing companies have their own proprietary software platforms (for which costs are lower due to the fact that many have been in place for some time and the only common costs are maintenance and updates, over which they have control). In addition, the volume of claims processed by national anesthesia billing companies is usually considerably higher than a practice that performs its own billing. Consider also that many vendors such as clearing houses, statement companies, office supply companies, healthcare insurers, etc., provide discounted rates to large national RCM firms, which typically translates into lower overall business costs. Based on a five-year data sample obtained from practices that have transitioned from in-house billing to MiraMed subsidiary Medac, anesthesia practices spend between 6.5 percent to 11 percent of their collections to perform their own in-house billing. Outsourcing anesthesia billing reduces that cost—often significantly—as there is no need for billing staff or space for a billing department. Many providers and administrators like having hands-on control of financial operations through in-house billing. Much of the anxiety about relinquishing control centers around five key areas: (1) collections performance; (2) compliance; (3) appropriate staffing; (4) accessibility/proximity; and (5) A/R management. All of these anxieties may be addressed contractually with collections performance and A/R management guarantees and clauses, staffing guarantees, as well as auditing requirements to ensure compliance. Some billing companies are even willing to reduce your monthly fee and reallocate the funds toward an external auditor of your choice. Additionally, as with most outsourced billing agreements, billing companies are contractually obligated to follow up on all unpaid and denied claims.
Many providers and administrators like having hands-on control of financial operations through in-house billing. Much of the anxiety about relinquishing control centers around five key areas: (1) collections performance; (2) compliance; (3) appropriate staffing; (4) accessibility/proximity; and (5) A/R management. All of these anxieties may be addressed contractually with collections performance and A/R management guarantees and clauses, staffing guarantees, as well as auditing requirements to ensure compliance. Some billing companies are even willing to reduce your monthly fee and reallocate the funds toward an external auditor of your choice. Additionally, as with most outsourced billing agreements, billing companies are contractually obligated to follow up on all unpaid and denied claims. As previously mentioned, cost, liability and control are commonly the most heavily weighed factors when deciding whether to outsource your anesthesia billing operations. Aside from clinical services, billing and revenue cycle management are the most important processes of your practice. Your cash flow depends on them, so the decision of how to handle these services should not be taken lightly. You should do assessments of your practice’s costs, risks, staffing and volume metrics to determine what is right for you.
As previously mentioned, cost, liability and control are commonly the most heavily weighed factors when deciding whether to outsource your anesthesia billing operations. Aside from clinical services, billing and revenue cycle management are the most important processes of your practice. Your cash flow depends on them, so the decision of how to handle these services should not be taken lightly. You should do assessments of your practice’s costs, risks, staffing and volume metrics to determine what is right for you.
 The American Medical Association’s (AMA’s) 2021 CPT® codebook will likely be released without specific anesthesia-related code changes for the coming year, although coders will need to be aware that 2023 may bring substantial changes to the way postoperative pain management is reported. As there are no anesthesia-specific coding changes to consider for 2022, it is always a suitable time to review anesthesia coding basics and frequent coding problem areas.
The American Medical Association’s (AMA’s) 2021 CPT® codebook will likely be released without specific anesthesia-related code changes for the coming year, although coders will need to be aware that 2023 may bring substantial changes to the way postoperative pain management is reported. As there are no anesthesia-specific coding changes to consider for 2022, it is always a suitable time to review anesthesia coding basics and frequent coding problem areas. Although many practices are familiar with the care team approach which includes anesthesiologists and CRNAs, fewer may be familiar with CAAs. As of June 2019, CAAs are licensed in fourteen states with delegatory authority in two additional states and also are recognized under the TRICARE system. One important distinction between CRNAs and CAAs (depending on state scope of practice, delineation of privileges by the facility and individual malpractice carrier requirements), is that CRNAs may be allowed to practice as nonmedically directed, whereas a CAA must be medically directed.
Although many practices are familiar with the care team approach which includes anesthesiologists and CRNAs, fewer may be familiar with CAAs. As of June 2019, CAAs are licensed in fourteen states with delegatory authority in two additional states and also are recognized under the TRICARE system. One important distinction between CRNAs and CAAs (depending on state scope of practice, delineation of privileges by the facility and individual malpractice carrier requirements), is that CRNAs may be allowed to practice as nonmedically directed, whereas a CAA must be medically directed. Anesthesia coders should understand that anesthesia coding and billing guidelines will change from state to state and from payer to payer. Although CMS loosely follows the same IOM guidelines across all states, each Medicare administrative contractor (MAC) has its own idiosyncratic payer rules. This also is true for Medicaid, Blue Cross/Blue Shield (BCBS) and worker’s compensation. Individual payer contracts often include verbiage indicating their specific billing policies should be followed, yet they may or may not provide a copy of their coding/ billing policy. The best rule of thumb when there is not a policy is to follow the ASA RVG guidelines and use this resource in the event an appeal is necessary.
Anesthesia coders should understand that anesthesia coding and billing guidelines will change from state to state and from payer to payer. Although CMS loosely follows the same IOM guidelines across all states, each Medicare administrative contractor (MAC) has its own idiosyncratic payer rules. This also is true for Medicaid, Blue Cross/Blue Shield (BCBS) and worker’s compensation. Individual payer contracts often include verbiage indicating their specific billing policies should be followed, yet they may or may not provide a copy of their coding/ billing policy. The best rule of thumb when there is not a policy is to follow the ASA RVG guidelines and use this resource in the event an appeal is necessary. Another risk area is medical direction criteria. Many anesthesiologists fail to sign or initial their participation appropriately with a teaching or a medically directed case and may consider their signature as sufficient documentation of involvement. CMS and other payers require documentation during the most demanding procedures in the anesthesia plan, which includes induction and emergence, when applicable. Unless a monitored anesthesia care (MAC) case converts to general, induction and emergence are not applicable in such cases. Similarly, there is not an induction or emergence period associated with regional anesthesia.
Another risk area is medical direction criteria. Many anesthesiologists fail to sign or initial their participation appropriately with a teaching or a medically directed case and may consider their signature as sufficient documentation of involvement. CMS and other payers require documentation during the most demanding procedures in the anesthesia plan, which includes induction and emergence, when applicable. Unless a monitored anesthesia care (MAC) case converts to general, induction and emergence are not applicable in such cases. Similarly, there is not an induction or emergence period associated with regional anesthesia.
 As humans, we’re primed by evolutionary forces to fear the loss of something much more than we value an equivalent gain.
As humans, we’re primed by evolutionary forces to fear the loss of something much more than we value an equivalent gain. Perhaps they’re a little bit challenged as to the concept of personal space. Perhaps they’re not exactly politically correct. Perhaps they never stop challenging how and why things are done; and, when you tell them, they question the “why” underlying that. Responses such as “it’s always done that way,” or “because it’s a ‘best-practice,’” aren’t ultimate “whys.” Sometimes there is no ultimate “why,” or, at least, one that makes any real sense.
Perhaps they’re a little bit challenged as to the concept of personal space. Perhaps they’re not exactly politically correct. Perhaps they never stop challenging how and why things are done; and, when you tell them, they question the “why” underlying that. Responses such as “it’s always done that way,” or “because it’s a ‘best-practice,’” aren’t ultimate “whys.” Sometimes there is no ultimate “why,” or, at least, one that makes any real sense. Due to the mindset that medical groups are more like clubs of colleagues than business organizations, many groups build club-like protections into their documents, from partnership agreements to employment and independent contractor agreements. They define “for cause” termination narrowly and (and here’s the killer) build in “protections” for the subject physician as opposed to for the group—generally expressed as a required percentage vote of the group’s members before anyone can be expelled.
Due to the mindset that medical groups are more like clubs of colleagues than business organizations, many groups build club-like protections into their documents, from partnership agreements to employment and independent contractor agreements. They define “for cause” termination narrowly and (and here’s the killer) build in “protections” for the subject physician as opposed to for the group—generally expressed as a required percentage vote of the group’s members before anyone can be expelled.
 Empires come and go. None last forever. The story of the twentieth century has been the unraveling of the British Empire. When the century began, the United Kingdom presided over India, and now India is the largest democracy in the world, while Britain is a pale shadow of its former self. Germany once represented itself as the Third Reich under Adolf Hitler; but, ironically, today’s unified Germany under Angela Merkel is even more powerful and sustainable. History is the study of organizations struggling to fit their political, economic and social context. It is an ever-evolving process, but it is not limited to countries and governments. The aggregation of American medicine is following some very traditional patterns. Once prominent and powerful entities often succumb to a new market order.
Empires come and go. None last forever. The story of the twentieth century has been the unraveling of the British Empire. When the century began, the United Kingdom presided over India, and now India is the largest democracy in the world, while Britain is a pale shadow of its former self. Germany once represented itself as the Third Reich under Adolf Hitler; but, ironically, today’s unified Germany under Angela Merkel is even more powerful and sustainable. History is the study of organizations struggling to fit their political, economic and social context. It is an ever-evolving process, but it is not limited to countries and governments. The aggregation of American medicine is following some very traditional patterns. Once prominent and powerful entities often succumb to a new market order. As Nikita Khrushchev once said: “Economics is a discipline that does not respect one’s wishes.” And so we see the same struggle in the specialty of anesthesia to find organizational structures that will meet the needs of the local market.
As Nikita Khrushchev once said: “Economics is a discipline that does not respect one’s wishes.” And so we see the same struggle in the specialty of anesthesia to find organizational structures that will meet the needs of the local market. Not only has the pharmacology of anesthesia evolved significantly, and not only has the scope of the typical practice continued to change dramatically, but the very nature of anesthesia practice has undergone a paradigm shift. The majority of today’s group practices are less than 40 years old. Many practices were effectively shotgun marriages intended to meet the contractual requirements of hospitals and payers. Ultimately, some practices were organized on tighter and more unified models than others. For many, though, especially those with complicated internal productivity compensation plans, the new entities remain more confederations of competing providers than truly integrated business entities.
Not only has the pharmacology of anesthesia evolved significantly, and not only has the scope of the typical practice continued to change dramatically, but the very nature of anesthesia practice has undergone a paradigm shift. The majority of today’s group practices are less than 40 years old. Many practices were effectively shotgun marriages intended to meet the contractual requirements of hospitals and payers. Ultimately, some practices were organized on tighter and more unified models than others. For many, though, especially those with complicated internal productivity compensation plans, the new entities remain more confederations of competing providers than truly integrated business entities. Anesthesia departments were typically staffed by providers who chose to live in a particular community. Groups were often comprised of like-minded providers who had been recruited to be part of a team. In most situations the hospital communicated with a group president who enjoyed the respect of the members. Many of these leaders enjoyed long tenures as the leader. So what changed? Anesthesia practices started to grow and merge. Many sought experienced anesthesia administrators. In 1994, the American Society of Anesthesiologists (ASA) held its first Practice Management conference in Phoenix, a fact that demonstrated a growing concern for the management challenges facing the specialty. Increasingly, it became clear that it would take more than good care and consistent outcomes to ensure the success of an anesthesia practice. Hospital and managed care contracting were becoming the hot topics of the day.
Anesthesia departments were typically staffed by providers who chose to live in a particular community. Groups were often comprised of like-minded providers who had been recruited to be part of a team. In most situations the hospital communicated with a group president who enjoyed the respect of the members. Many of these leaders enjoyed long tenures as the leader. So what changed? Anesthesia practices started to grow and merge. Many sought experienced anesthesia administrators. In 1994, the American Society of Anesthesiologists (ASA) held its first Practice Management conference in Phoenix, a fact that demonstrated a growing concern for the management challenges facing the specialty. Increasingly, it became clear that it would take more than good care and consistent outcomes to ensure the success of an anesthesia practice. Hospital and managed care contracting were becoming the hot topics of the day. Anesthesia is an increasingly expensive service to provide. The burdened cost of a physician anesthesiologist can be as much as $500,000 per year. Many CRNAs get paid at least half that. There is no such thing as a local market any more. Anesthesia providers tend to migrate to practices with the best compensation and the most reasonable call requirements, no matter where they are located. It is a provider’s market. The migration of cases to ambulatory facilities has only exacerbated the challenge as anesthesiologists move from traditional hospital practices with a full call requirement to ambulatory centers where they only have to work Monday through Friday, with no nights or weekends.
Anesthesia is an increasingly expensive service to provide. The burdened cost of a physician anesthesiologist can be as much as $500,000 per year. Many CRNAs get paid at least half that. There is no such thing as a local market any more. Anesthesia providers tend to migrate to practices with the best compensation and the most reasonable call requirements, no matter where they are located. It is a provider’s market. The migration of cases to ambulatory facilities has only exacerbated the challenge as anesthesiologists move from traditional hospital practices with a full call requirement to ambulatory centers where they only have to work Monday through Friday, with no nights or weekends.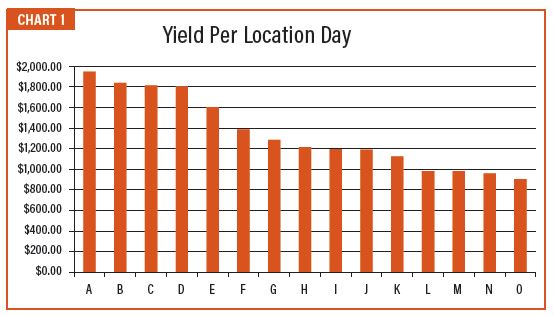
 Anesthesia is unique in so many ways. The calculation of anesthesia charges and payments bears no relationship to that of any other specialty. Anesthesia providers are the only ones who get paid for the time they spend with patients as compared to surgeons who get a flat payment per procedure. Anesthesia groups have used this unique charge calculation to design some very creative compensation schemes. While not all practices pay their providers based on provider productivity, there are many that do, and this continues to be a defining feature of the specialty. Individual providers prefer to feel as though they are getting paid for every service they provide. And while this concept has made it possible for many providers to feel comfortable in a group practice, it is not always perceived as a positive by the rest of the OR staff. An OR nurse once commented that she could always tell how members got paid based on their behavior and their willingness or unwillingness to do certain cases.
Anesthesia is unique in so many ways. The calculation of anesthesia charges and payments bears no relationship to that of any other specialty. Anesthesia providers are the only ones who get paid for the time they spend with patients as compared to surgeons who get a flat payment per procedure. Anesthesia groups have used this unique charge calculation to design some very creative compensation schemes. While not all practices pay their providers based on provider productivity, there are many that do, and this continues to be a defining feature of the specialty. Individual providers prefer to feel as though they are getting paid for every service they provide. And while this concept has made it possible for many providers to feel comfortable in a group practice, it is not always perceived as a positive by the rest of the OR staff. An OR nurse once commented that she could always tell how members got paid based on their behavior and their willingness or unwillingness to do certain cases. We have a saying at Anesthesia Business Consultants that “if you have seen one anesthesia group, you have seen one anesthesia group.” Each is a unique product of its history, the culture of the medical community and the specific requirements of the institution. Because of this, it is often perilous to generalize about the state of the specialty or its future. Historians like to remind us that history unfolds from the general to the specific. The issues identified above represent the general themes that have marked the evolution of the specialty. Each may play itself out to varying degrees in the context of a particular practice. Some practices inevitably are fortunate or savvy enough to avoid any of the downsides as they navigate the changes in the industry. The practices that fail or morph into some other format do so because the stakeholders were simply not the ones with a better solution.
We have a saying at Anesthesia Business Consultants that “if you have seen one anesthesia group, you have seen one anesthesia group.” Each is a unique product of its history, the culture of the medical community and the specific requirements of the institution. Because of this, it is often perilous to generalize about the state of the specialty or its future. Historians like to remind us that history unfolds from the general to the specific. The issues identified above represent the general themes that have marked the evolution of the specialty. Each may play itself out to varying degrees in the context of a particular practice. Some practices inevitably are fortunate or savvy enough to avoid any of the downsides as they navigate the changes in the industry. The practices that fail or morph into some other format do so because the stakeholders were simply not the ones with a better solution.