Winter 2023
Cooperation Without Trust
Will Latham, MBA, President
Latham Consulting Group, Inc., Chattanooga, TN
 Wouldn’t it be great if all the physicians in your group fully trusted each other at all times on all issues? If that’s how it works in your group, count your blessings.
Wouldn’t it be great if all the physicians in your group fully trusted each other at all times on all issues? If that’s how it works in your group, count your blessings.
In most cases, however, there is at least some distrust among members of anesthesiology groups. This is the result of differing opinions, differing goals (often due to age and financial situation), and what we have found to be a naturally forming level of paranoia.
This issue is complicated by the fact that most, (but not all) anesthesiologists are conflict avoiders. They would rather avoid a situation than confront their partners on issues.
Yet, even without full trust and conflict avoidance among group members, anesthesiology groups need to move forward. And to move forward, they must decide which direction they will move.
Here are four methods we have seen groups use to make decisions and move forward.
1. Commit to Support Group Decisions
There is an adage that erroneously gets credence: individual physicians believe that “if I didn’t vote for it, or I don’t agree with it, then I don’t have to do it.”
If this is the normative behavior of your group, you will always be troubled in making real decisions and moving forward. To improve the situation, your group needs to ask and answer three key questions:
- How will we make decisions as a group? Typically, this is through discussion and a vote.
- What is expected of each physician once the group has decided on an issue? The shareholders should pre-commit to support it, do it and not sabotage it.
- What are a physician’s options if they don’t like the decision? The shareholders should commit that they will follow ONLY one of the following options:
- Do it anyway, that’s group practice.
- Try to get it changed in the appropriate forum, such as a group meeting, but keep supporting or doing it until changed.
- Self-select yourself out of the group.
2. Can Three by Five Cards Really Save Us?
 When the members of an anesthesiology group meet, at either shareholders or board meetings, they typically deal with issues that require a decision. Unfortunately, voting doesn’t work very well in many medical groups for the following reasons:
When the members of an anesthesiology group meet, at either shareholders or board meetings, they typically deal with issues that require a decision. Unfortunately, voting doesn’t work very well in many medical groups for the following reasons:
- Some group members believe the idea of actually voting is too “formal.”
- Some groups think they have consensus because no one speaks up (or only a few speak up and the thought is the rest are willing to go along). These groups are fooling themselves because, when people don’t speak up, it typically means they disagree. In addition, if you think you have consensus, why not vote to make sure you do?
- Because many physicians are conflict avoiders. Sometimes discussions go on and on because people don’t want to raise their hands to vote and possibly enter into conflict with those that don’t agree with them. This can make meetings last much longer than they need to.
In my opinion, it’s best to formally vote on issues to make sure the group has the needed majority or super-majority vote. This assumes that the group has gone through a process where the group members agree to support group decisions as noted above.
To deal with conflict avoidance, I am seeing more and more groups move to using “secret ballots” for their voting process. Most groups use secret ballots for electing their board and officers, but some groups use them when they need to vote on controversial issues, or in more and more cases, on all issues. Why are secret ballots useful?
- They allow the individuals to “vote their conscience” with less fear of retribution.
- They avoid one physician “bullying” another physician into changing their vote.
- They often speed up a meeting because people don’t delay voting to put off conflict.
There are several ways to implement secret ballots—here are two:
- Use three-by-five cards as the secret ballots.
- We have observed some groups starting to use “audience response systems.” One medical group president recently told us that his group has begun using such a voting system for all issues and that they had cut about 25 percent off the time of every meeting by using the system.
Groups that use secret ballots for all their issues have told us that there is only one potentially negative outcome—that people will push too quickly for a vote. Therefore, it is up to the meeting manager to make sure that the group has had a full discussion of the issue prior to voting.
3. Fair Elections
 If elections are not conducted in a fair and reasonable method, it taints a group’s governance and reduces physicians’ adherence to group decisions. So naturally, election voting should allow for people to be nominated, and then secret ballot used for the actual vote.
If elections are not conducted in a fair and reasonable method, it taints a group’s governance and reduces physicians’ adherence to group decisions. So naturally, election voting should allow for people to be nominated, and then secret ballot used for the actual vote.
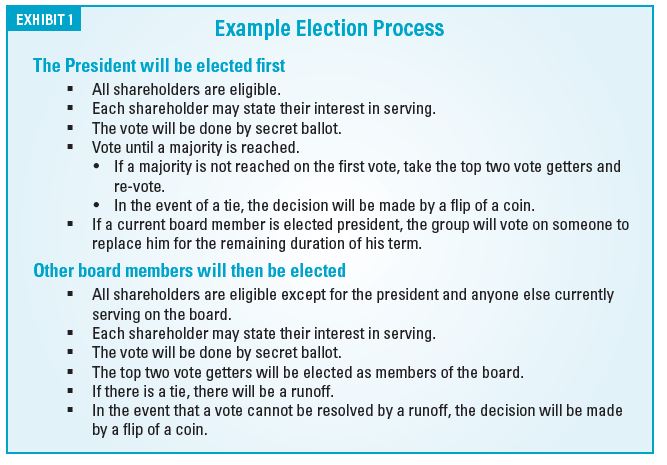
But sometimes it’s difficult to make a change when one is needed. This is another result of conflict avoidance. If someone in power doesn't want to lose their position, it is difficult for other shareholders to challenge them. This can result in the group not electing the people believed best to lead, and a feeling that the whole process is unfair and thus tainted.
One way out of this conundrum is to alter the election process to that as shown in Exhibit 1. By using this method, no one has to stand up and challenge the current leaders.
4. Revisiting Issues
 Many medical groups make a decision and then revisit it over and over again.
Many medical groups make a decision and then revisit it over and over again.
This situation comes about when a few members of the group do not get their way in the first vote. They then use this strategy to either torture the group into changing the decision, or to paralyze the group.
When other group members state their frustration about the problems revisiting an issue will cause, the physicians who want to revisit the issue typically respond that additional information has come to light which they believe should be considered in making the decision. This can go on ad infinitum and the ability to pursue key opportunities (or the ability to avoid key threats) can be lost.
Many organizations suffer from this problem, but the situation is more challenging for medical groups where the shareholder physicians are usually equal owners of the practice. Some physician shareholders believe that equal ownership gives them the right to have a say about every issue at any time they want (and often waste precious group meeting time). And they use this right as a torture technique to get what they want.
One way to reduce the use of this torture technique (revisiting issues over and over again) is to put a “speed bump” for items to return to the agenda for discussion.
For example, the group could implement a policy that requires 30 percent of the shareholders to sign a document asking to bring an item back to the floor for re-discussion once a decision has been made (it is important that they sign a document, rather than someone say “I had 30 percent of the people say they’d like to re-discuss this issue”).
This policy doesn’t close the door to re-discussing an issue (if more than 30 percent want to re-discuss an issue, the group probably should). However, it will typically reduce the number of times this torture technique is used.
Some will Fight This
Let’s be realistic: there will be those in the group who will fight the implementation of the above ideas. But let’s also be truthful: the reason they will fight it is that they are getting something out of the current state of dysfunction.
So, don’t let the few prevent the group from making good changes that will benefit the entire group, rather than the individual.
 For more than 30 years, Will Latham has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 135 medical practices representing over 1,300 physicians. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at wlatham@lathamconsulting.com.
For more than 30 years, Will Latham has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 135 medical practices representing over 1,300 physicians. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at wlatham@lathamconsulting.com.