Summer 2022
Surgical Services on the Move
Bart Edwards, MHS, MBA
Executive Vice President of Client Services Anesthesia Business Consultants, LLC, Jackson, MI
Medical care has been shifting out of inpatient venues and into outpatient and ambulatory sites. Advances in clinical approaches and technology, including new developments in anesthesia and pain control as well as minimally invasive surgical procedures, have enabled numerous procedures to migrate into outpatient and ambulatory settings.
Patients increasingly express a preference for hospital outpatient and ambulatory service center (ASC) venues for surgical care. As consumers, patients are more satisfied with the faster access, shorter stays and better service, versus inpatient stays. Given the option, most patients have an understandable desire to recover outside of the inpatient environment. Patients may appreciate an ASC’s more intimate environment to the hospital, giving them a greater sense of personalized care and contact with their care team. These underlying consumer preferences have only been reinforced by COVID-19, as patients and even some providers are significantly less comfortable returning with inpatient stays in light of the pandemic.
 With the rise in narrow networks and high-deductible health plans, consumers are increasingly cost-conscious in their medical choices. Lower overall costs for outpatient and ASC services can provide an added benefit in the form of reduced deductible, copay and coinsurance to the patient.
With the rise in narrow networks and high-deductible health plans, consumers are increasingly cost-conscious in their medical choices. Lower overall costs for outpatient and ASC services can provide an added benefit in the form of reduced deductible, copay and coinsurance to the patient.
In addition to hospital outpatient settings, physicians often also prefer ambulatory surgery center operations because they can see patients in more service-oriented settings. Costs can be significantly less at ASCs, as they are often configured at a lower cost base across staffing, space and some types of supplies. In addition, there are a number of ASC financial models that convey financial alignment with physicians, including ownership.
Procedures have been excluded from outpatient and ASC locations via the CMS Inpatient Only (IPO) list, a list of services that, due to their medical complexity, Medicare will only pay when performed in the inpatient setting. In its 2021 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System Final Rule, CMS proposed elimination of the IPO list over a three-year period and immediately removed the restriction on 298 services. The rule also revised the long-standing criteria that were historically used to add covered surgical procedures to the ASC Covered Procedures List (ASC CPL). As a result, 267 new procedures moved onto the ASC CPL.
To get a sense of the impact on anesthesia services, a sample of surgical data from 15 large client practices, billed by Anesthesia Business Consultants, who are providing services across inpatient, outpatient, and ASC place-of-service codes were reviewed for calendar years 2018 through 2021. The data showed some interesting trends overall, and specifically related to the 2021 revisions to the regulatory controls on where procedures were allowed.
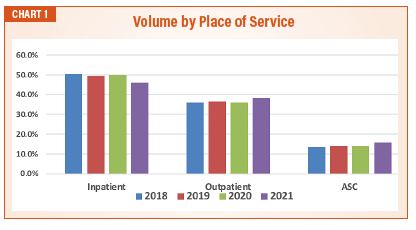
Consistent with the national conversation regarding the move toward outpatient and ASC services, our clients saw a gently decreasing trend in the inpatient volume, and a corresponding increase in outpatient and ASC services as percentage of total volume. Excluded from this data due to its relative size, there was also an increase in office-based anesthesia services for this sample of practices—but the volume was less than one percent of the sample (See Chart 1).
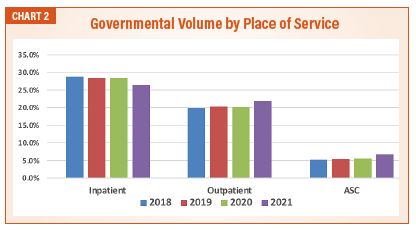
Drilling down to governmental payers helped illuminate how much of the shift is due to the change in regulation. An overall increase in procedures permitted in outpatient and ASC places of services for Medicare patients resulted in the expected shift in service locations. The volume of inpatient services decreased as 26.4 percent in 2021. This is particularly concerning for anesthesia, as the differential between commercial and governmental rates is more material than most specialties (See Chart 2).
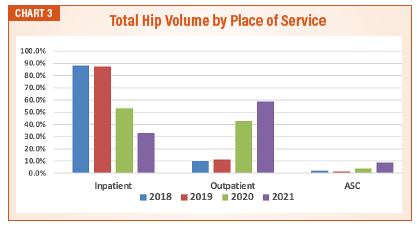
Further focusing on a specific procedure; total hip arthroplasty was moved off the IPO list in 2020, and then moved onto the ASC CPL in 2021. A review of overall volume for that procedure by place of service shows the immediate and dramatic impact of each regulatory release. Note the marked increase in the percentage of services moved to the outpatient venue in 2020, and continued growth in 2021. ASC’s were also quick to respond to the 2021 addition of these procedures to their CPL with an immediate increase in volume (See Chart 3).
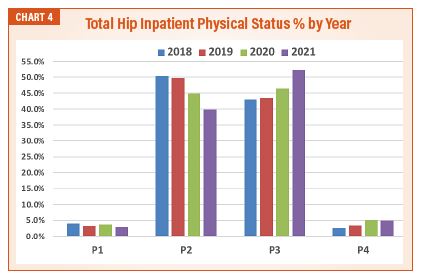
A review of the average ASA physical status classification for 2021 total hip replacement patients from our practices suggests that physicians guide patients to the place of service that is consistent with their risk profile. The lowest average ASA physical status value was for patients with services in ASCs. The patients with highest average ASA classifications were served in an inpatient setting, due to the potential need for complex anesthesia or increased clinical backup. With the expansion of potential venues, the graph (See Chart 4) shows the reduction of less-risky (lower ASA physical status rated) patients from the inpatient place of service.
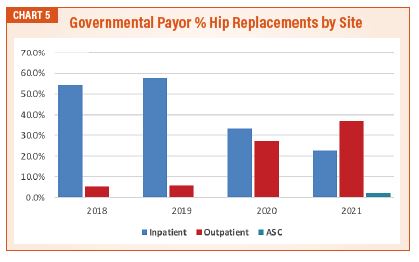
Independent of the clinical and service-related benefits of this opportunity, the impact on anesthesia practices should be discussed. One result of this regulatory change may be reduced utilization in hospitals, and poorer reimbursement in ASCs. The redirection of cases out of hospitals reduces the total revenue potential, but does nothing to relieve the burden of coverage for off-hour surgeries and call. Most hospitals are already providing a subsidy to finance these coverage requirements, the additional stress from reduced volume will exacerbate an already demanding financial scenario. Outpatient services (and ASCs in particular) historically benefitted from a favorable payor mix. The addition of governmental payor cases at ASC’s will make those sites less favorable from a reimbursement standpoint. In addition, the horizontal expansion of anesthetizing locations may create additional coverage challenges in an employment environment already experiencing provider shortage (See Chart 5).
Recent policy changes in the 2022 Outpatient Prospective Payment System Final Rule will make 2021 a unique window into the impact of the healthcare regulatory environment on this trend. After beginning the planned three-year transition to eliminate the IPO List in 2021, CMS reversed course in 2022 and reinstated most of the procedures eliminated in 2021. The agency also withdrew 258 of the 267 procedures newly added to the ASC CPL in 2021 as part of its revised procedure nomination process.
 CMS will reassess how it evaluates procedures for removal and its longer-term plan for the IPO and ASC CPL. As seen by the regulatory changes in 2021, surgeons and patients have taken advantage of the flexibility to select the most desirable clinically appropriate venue for services based on individualized patient plans. The movement driven by changes in the Inpatient Only list and ASC Covered Procedures list demonstrates the impact of the agency’s regulations on the site of service selection. When released from regulatory controls, the market has shown a preference for outpatient and ASC services versus the traditional hospital inpatient experience. While this may be a positive development for patients and overall system costs, it presents challenges to anesthesia practices that will require deliberate planning and adjustment to financial and staffing models. The reversal on the IPO and ASA CPL changes provides a temporary reprieve during which anesthesia practices can consider the best course of action to address the coming inpatient exodus.
CMS will reassess how it evaluates procedures for removal and its longer-term plan for the IPO and ASC CPL. As seen by the regulatory changes in 2021, surgeons and patients have taken advantage of the flexibility to select the most desirable clinically appropriate venue for services based on individualized patient plans. The movement driven by changes in the Inpatient Only list and ASC Covered Procedures list demonstrates the impact of the agency’s regulations on the site of service selection. When released from regulatory controls, the market has shown a preference for outpatient and ASC services versus the traditional hospital inpatient experience. While this may be a positive development for patients and overall system costs, it presents challenges to anesthesia practices that will require deliberate planning and adjustment to financial and staffing models. The reversal on the IPO and ASA CPL changes provides a temporary reprieve during which anesthesia practices can consider the best course of action to address the coming inpatient exodus.

Bart Edwards, MHS, MBA serves as an Executive Vice President of Client Services for Anesthesia Business Consultants. Bart directs a team of Analysts, Managers, Directors and Vice Presidents who are the liaison between clients and all the resources, skill and experience that ABC offers. Bart can be reached at Bart.Edwards@anesthesiallc.com.