Fall 2021
The Ebb and Flow of Anesthesia Practices
Jody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services
Anesthesia Business Consultants, LLC, Jackson, MI
 Empires come and go. None last forever. The story of the twentieth century has been the unraveling of the British Empire. When the century began, the United Kingdom presided over India, and now India is the largest democracy in the world, while Britain is a pale shadow of its former self. Germany once represented itself as the Third Reich under Adolf Hitler; but, ironically, today’s unified Germany under Angela Merkel is even more powerful and sustainable. History is the study of organizations struggling to fit their political, economic and social context. It is an ever-evolving process, but it is not limited to countries and governments. The aggregation of American medicine is following some very traditional patterns. Once prominent and powerful entities often succumb to a new market order.
Empires come and go. None last forever. The story of the twentieth century has been the unraveling of the British Empire. When the century began, the United Kingdom presided over India, and now India is the largest democracy in the world, while Britain is a pale shadow of its former self. Germany once represented itself as the Third Reich under Adolf Hitler; but, ironically, today’s unified Germany under Angela Merkel is even more powerful and sustainable. History is the study of organizations struggling to fit their political, economic and social context. It is an ever-evolving process, but it is not limited to countries and governments. The aggregation of American medicine is following some very traditional patterns. Once prominent and powerful entities often succumb to a new market order.
Why should this be any different in the world of anesthesiology? The past forty years have seen a dramatic transformation of the specialty as individual providers have banded together into group practices and then sought to grow their empires into even larger regional or national provider organizations. Sheridan Anesthesia was once a private anesthesia practice in south Florida before it became the national organization. Now it has merged with Emcare to become Envision. Who can know what its next metamorphosis will be?
If there is one thing that has changed over the past forty years it is the impact of market forces on the specialty. Amr Abouleish, MD often reminded his audiences that . . .
Healing is an art Medicine is a science Healthcare is a business.
 As Nikita Khrushchev once said: “Economics is a discipline that does not respect one’s wishes.” And so we see the same struggle in the specialty of anesthesia to find organizational structures that will meet the needs of the local market.
As Nikita Khrushchev once said: “Economics is a discipline that does not respect one’s wishes.” And so we see the same struggle in the specialty of anesthesia to find organizational structures that will meet the needs of the local market.
There is a tendency to refer to practices that go out of business as failed practices, but this is neither fair nor accurate. Hospitals with operating rooms cannot function without anesthesia providers. Even if a group practice cannot meet the needs of the facility in its current form, the facility must ultimately figure out another solution. However traumatic this transition may be, it is just that—a transition.
Sometimes what is perceived as a traumatic juncture in the lifecycle of an anesthesia practice is simply a failure of imagination and an unwillingness to metamorphose into an entity that meets the new market realities. Too often this is an unwillingness to let go of long-held sacred cows. We often say that the only constant in American medicine is change. When it comes to the practice of anesthesia this is the reality.
Let us consider three of the most common sacred cows that have ultimately undone many anesthesia practices.
- Anesthesia providers only create value when they are giving anesthesia. Many practices are still coming to realize the value of professional management.
- Physician-only anesthesia is preferable to a careteam model. Even though 75 percent of all anesthetics are administered by a team of physicians and CRNAs, many practices—especially in the west—continue to cling to a physician-only model.
- The success or failure of an anesthesia practice is a function of the quality of care provided. The reality is that quality of care is a given, what matters most is the quality of service provided to the customer.
Political Realities
 Not only has the pharmacology of anesthesia evolved significantly, and not only has the scope of the typical practice continued to change dramatically, but the very nature of anesthesia practice has undergone a paradigm shift. The majority of today’s group practices are less than 40 years old. Many practices were effectively shotgun marriages intended to meet the contractual requirements of hospitals and payers. Ultimately, some practices were organized on tighter and more unified models than others. For many, though, especially those with complicated internal productivity compensation plans, the new entities remain more confederations of competing providers than truly integrated business entities.
Not only has the pharmacology of anesthesia evolved significantly, and not only has the scope of the typical practice continued to change dramatically, but the very nature of anesthesia practice has undergone a paradigm shift. The majority of today’s group practices are less than 40 years old. Many practices were effectively shotgun marriages intended to meet the contractual requirements of hospitals and payers. Ultimately, some practices were organized on tighter and more unified models than others. For many, though, especially those with complicated internal productivity compensation plans, the new entities remain more confederations of competing providers than truly integrated business entities.
It used to be that if anesthesia providers were clinically busy and the payer mix was adequate, they could generate sufficient professional fee income to maintain their independence. It was commonly thought that if a provider could consistently bill 50 ASA units per location day there was no need for financial support. Over the past ten years, the specialty has experienced a tectonic shift that is the result of three main factors: a proliferation of anesthetizing locations as cases have migrated from traditional inpatient venues to all manner of outpatient venues; a resulting decline in provider productivity as measured in average units generated per location day; and a gradual, but inexorable, erosion of the average yield per billed unit as Medicare and Medicaid represent an ever larger percentage of the payer mix. Given these powerful factors, it has become increasingly challenging to meet the income expectations of providers. The greatest challenge of most of today’s anesthesia practice is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the service requirements of the facilities they serve. The current perception is that there is a shortage of providers.
All of this has changed the politics of anesthesia. When anesthesia was a free good to the hospital, contractual relationships with facilities were much simpler. When an anesthesia group evolves from a no-subsidy practice to a subsidy practice, it changes the very nature of the relationship. The request for financial support now focuses on the value proposition being negotiated. Where once a group president could sit down with the CEO of the hospital and hammer out a deal, now the process often involves an extensive and expensive process that frequently requires consultants to evaluate the fair market value (FMV) of the practice.
The complexity of such negotiations has inevitably resulted in a much more political process. It used to be that hospital administrators were more willing to accept quirky anesthesia practice behaviors long as patients were treated well and had good outcomes. Most administrators never really gave much thought to other anesthesia service options. The new reality is completely different. It is the reality of the RFP (request for proposal). No three letters evoke such fear in the minds of anesthesia providers. The advent of a proliferation of RFPs means that administrators are now evaluating the current solution as compared to market options.
 Anesthesia departments were typically staffed by providers who chose to live in a particular community. Groups were often comprised of like-minded providers who had been recruited to be part of a team. In most situations the hospital communicated with a group president who enjoyed the respect of the members. Many of these leaders enjoyed long tenures as the leader. So what changed? Anesthesia practices started to grow and merge. Many sought experienced anesthesia administrators. In 1994, the American Society of Anesthesiologists (ASA) held its first Practice Management conference in Phoenix, a fact that demonstrated a growing concern for the management challenges facing the specialty. Increasingly, it became clear that it would take more than good care and consistent outcomes to ensure the success of an anesthesia practice. Hospital and managed care contracting were becoming the hot topics of the day.
Anesthesia departments were typically staffed by providers who chose to live in a particular community. Groups were often comprised of like-minded providers who had been recruited to be part of a team. In most situations the hospital communicated with a group president who enjoyed the respect of the members. Many of these leaders enjoyed long tenures as the leader. So what changed? Anesthesia practices started to grow and merge. Many sought experienced anesthesia administrators. In 1994, the American Society of Anesthesiologists (ASA) held its first Practice Management conference in Phoenix, a fact that demonstrated a growing concern for the management challenges facing the specialty. Increasingly, it became clear that it would take more than good care and consistent outcomes to ensure the success of an anesthesia practice. Hospital and managed care contracting were becoming the hot topics of the day.
This growing awareness of the practice management challenges facing the specialty and a desire to exert leverage in their contract negotiations was not always well received by hospital administrators. The politics of medicine started to play itself out. Some practices were astute in managing their relationship with administration, others were not. It is often said that managing a suite of operating rooms effectively is like sitting on a three legged stool where anesthesia is one leg, the surgeons are another leg and administration is the third leg. Historically, hospitals have aligned themselves with the surgeons and done everything possible to encourage their loyalty, which has resulted in some very unprofitable coverage requirements for anesthesia. Anesthesia has more and better data about what happens in the operating rooms. Many in the anesthesia community started suggesting that anesthesia should play a much more significant role in managing the operating rooms and enhancing the profitability of hospitals. Although the potential of this advantage has yet to be fully realized, it is a card that practices are starting to play to align themselves with administration.
Every anesthesia practice has its challenges. Practices that can align themselves with administration in a collaborative problem-solving mode enjoy far more support from administration. Unfortunately, many are not so savvy. Money is often the straw that broke the camel’s back. If administration does not view the anesthesia practice as a reasonable business partner, the relationship is doomed. The list of anesthesia practices that have succumbed is growing. The irony of this situation is that while the current group may have gone out of business, the hospital still needs anesthesia providers.
Economic Realities
 Anesthesia is an increasingly expensive service to provide. The burdened cost of a physician anesthesiologist can be as much as $500,000 per year. Many CRNAs get paid at least half that. There is no such thing as a local market any more. Anesthesia providers tend to migrate to practices with the best compensation and the most reasonable call requirements, no matter where they are located. It is a provider’s market. The migration of cases to ambulatory facilities has only exacerbated the challenge as anesthesiologists move from traditional hospital practices with a full call requirement to ambulatory centers where they only have to work Monday through Friday, with no nights or weekends.
Anesthesia is an increasingly expensive service to provide. The burdened cost of a physician anesthesiologist can be as much as $500,000 per year. Many CRNAs get paid at least half that. There is no such thing as a local market any more. Anesthesia providers tend to migrate to practices with the best compensation and the most reasonable call requirements, no matter where they are located. It is a provider’s market. The migration of cases to ambulatory facilities has only exacerbated the challenge as anesthesiologists move from traditional hospital practices with a full call requirement to ambulatory centers where they only have to work Monday through Friday, with no nights or weekends.
Unfortunately, too many hospital administrators do not fully appreciate the economics of anesthesia. The profitability of an anesthesia practice is ultimately a function of one thing: the profitability of coverage. There is a cost for each anesthetizing location that must be staffed. It may represent the cost of an anesthesiologist divided by the number of days he or she works a year as in the following example.
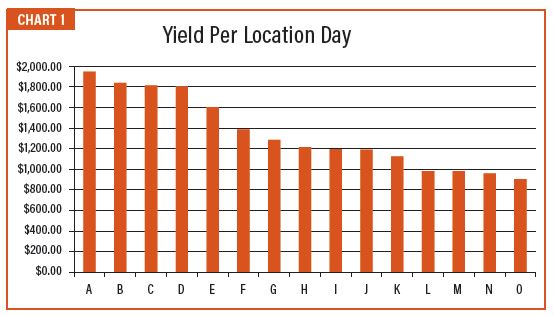
If the total cost of a physician is $475,000 and the provider works 227 days a year, then the cost per clinical day is $2,100. The question is how many actual days of work generate $2,100 in collections, net of overhead costs such as billing and management? Some practices can reduce this cost through a leveraged careteam model where a physician may medically direct three or four CRNAs. Even when this can be done successfully, it may not close the gap between the cost and the revenue per location day.
The chart shown below is a representative sample of the actual yields per clinical day of 15 client practices from across the country. It should be noted that none actually generate $2100 per day, which is why all practices must focus on reducing the cost of providing care.
A number of factors make this simple profitability calculation difficult to apply to the entire practice. Some venues are inherently unprofitable. Depending how busy OB is, this is often a particularly unprofitable service for anesthesia. Hospitals often want to launch new service lines that require additional staff, but which provide little additional fee for service income to the practice. Call requirements are particularly onerous. About 75 percent of the revenue generated per anesthetizing location is generated between 7 AM and 3 PM. Requiring a physician or CRNA to remain in house all night is always an expensive requirement. It does not really matter how profitable certain lines of business are if their profitability is diluted by other unprofitable lines.
Most hospitals were designed and built on the assumption that “if you build it, they will come.” The reality is that in the current environment, cases migrate to the most convenient and most cost-effective venues. In fact, what we are seeing is a growing schism between the traditional inpatient venues which have become dumping grounds for the most acute Medicare patients and the ambulatory facilities where generally healthier patients with good commercial insurance go.
Hospital subsidies are supposed to compensate the anesthesia practice for the financial loss they incur meeting hospital coverage requirements. This is not always a straightforward calculation. Changes in case volume, as were experienced in 2020 as a result of Covid-19, or eroding payer mix, often impact the calculation negatively. It is often said that it is easy to calculate the necessary subsidy today, but it will probably be wrong tomorrow. More often than not, hospitals try to put the risk for such fluctuations on the anesthesia practice.
Poor payer mix, i.e., too high a percentage of Medicare and Medicaid patients, and inadequate or eroding case volume are often cited as the reason why practices fail; and, while these factors may be real, it is important to remember that the hospital will still need anesthesia. Consider that perhaps the practice was too wedded to certain preconceived assumptions to explore other options. Many hospitals are now suggesting employment options that are anathema to private practice providers, even though the end result might ensure a more reasonable and predictable level of compensation and a better quality of life. As mentioned at the outset, most anesthesia practices are now facing the same set of economic challenges that impact their ability to recruit and retain qualified providers. While it is true that some practices enjoy more favorable locations than others, the big difference between those that remain viable and those that don’t is their ability to think outside the box and find creative solutions. Why is it that national anesthesia staffing companies such as Envision and NAPA keep growing? They come at the challenges with a different set of assumptions. They may have slicker responses to RFPs and a greater quiver of arrows; but, at the end of the day, their solution is not that much different. It is just delivered with more credibility.
Social Considerations
 Anesthesia is unique in so many ways. The calculation of anesthesia charges and payments bears no relationship to that of any other specialty. Anesthesia providers are the only ones who get paid for the time they spend with patients as compared to surgeons who get a flat payment per procedure. Anesthesia groups have used this unique charge calculation to design some very creative compensation schemes. While not all practices pay their providers based on provider productivity, there are many that do, and this continues to be a defining feature of the specialty. Individual providers prefer to feel as though they are getting paid for every service they provide. And while this concept has made it possible for many providers to feel comfortable in a group practice, it is not always perceived as a positive by the rest of the OR staff. An OR nurse once commented that she could always tell how members got paid based on their behavior and their willingness or unwillingness to do certain cases.
Anesthesia is unique in so many ways. The calculation of anesthesia charges and payments bears no relationship to that of any other specialty. Anesthesia providers are the only ones who get paid for the time they spend with patients as compared to surgeons who get a flat payment per procedure. Anesthesia groups have used this unique charge calculation to design some very creative compensation schemes. While not all practices pay their providers based on provider productivity, there are many that do, and this continues to be a defining feature of the specialty. Individual providers prefer to feel as though they are getting paid for every service they provide. And while this concept has made it possible for many providers to feel comfortable in a group practice, it is not always perceived as a positive by the rest of the OR staff. An OR nurse once commented that she could always tell how members got paid based on their behavior and their willingness or unwillingness to do certain cases.
Clinically, anesthesia has many distinct characteristics. Each case is both art and science. The provider must assess the specific concerns of the patient, the needs of the surgeon, and their own experience with such cases. No two anesthetics for the same surgical procedure are the same. This fact alone encourages a kind of specialty autonomy. Starbucks strives to make every latte the same, no matter who prepares it or where it is delivered. This kind of thinking and what is often derided as “cookbook medicine” is anathema to anesthesia providers. And while groups will proctor new physicians for a short period when they are hired, once they are vetted, there is little or no oversight or guidance unless there are clinical issues. Anesthesia enjoys a long tradition of independent and autonomous clinical decision making that continues to influence how groups practice. A large group in Southern California once held a series of strategic retreats, the result of which was an agreement that the organization would be pre-eminent in matters of billing, contracting and human resource management, but that the individual providers would be completely autonomous in all matters clinical.
A former ASA president, Peter McDermot, MD was once quoted as saying, “Anesthesia group, that is an oxymoron; it is like herding cats.” And this is exactly what makes hospital administrators crazy. They want to know that the group speaks with one voice and that the group has the structure, commitment and tools to deal with outliers. It is no accident that virtually all professional service agreements now include language clarifying group disciplinary procedures and what it takes to remove problem providers.
This is one of the greatest challenges most groups face: disciplining their own. It has often been noted that most anesthesia practices are truly not business entities because they operate more as medical professional fraternities. The real problem is that, as American medicine becomes more competitive and as the cost of care becomes the primary focus of hospital administrations, it becomes increasingly important that business partners, such as the anesthesia groups, mirror the goals and objectives of the facility. Many an anesthesia group has lost its contract simply because it lacked effective and professional management. In fact, this has become one of the appeals of the large national anesthesia staffing companies. The perception is that they are run as professional entities.
One may also ask why so many hospital administrations are seriously considering employment models for their anesthesia providers even though this may ultimately result in a more expensive solution? The argument given is that employment equals control. This is no doubt a reaction to the perception that they simply need to find a different way to herd the cats.
There is a certain irony here. Ultimately, everyone wants control. Anesthesia providers want control of their own income and lifestyle. Hospital administrators want control of the anesthesia service so that it acts in concert with the other lines of business they manage. The reality is that all parties are at the mercy of market factors beyond their control. The truth is that no one actually has control. Anesthesia is a quintessential service specialty and must be prepared to respond to whatever volume and kinds of cases the surgeons bring to the facility. Let us just consider the impact of endoscopy, which now represents about 30 percent of most practice activity. The revenue potential of a practice is a function of OR utilization, payer mix, coding and billing policy changes, and payer pushback on what is starting to be deemed an over-used service. In the end, no one really has any control at all.
What it All Means
 We have a saying at Anesthesia Business Consultants that “if you have seen one anesthesia group, you have seen one anesthesia group.” Each is a unique product of its history, the culture of the medical community and the specific requirements of the institution. Because of this, it is often perilous to generalize about the state of the specialty or its future. Historians like to remind us that history unfolds from the general to the specific. The issues identified above represent the general themes that have marked the evolution of the specialty. Each may play itself out to varying degrees in the context of a particular practice. Some practices inevitably are fortunate or savvy enough to avoid any of the downsides as they navigate the changes in the industry. The practices that fail or morph into some other format do so because the stakeholders were simply not the ones with a better solution.
We have a saying at Anesthesia Business Consultants that “if you have seen one anesthesia group, you have seen one anesthesia group.” Each is a unique product of its history, the culture of the medical community and the specific requirements of the institution. Because of this, it is often perilous to generalize about the state of the specialty or its future. Historians like to remind us that history unfolds from the general to the specific. The issues identified above represent the general themes that have marked the evolution of the specialty. Each may play itself out to varying degrees in the context of a particular practice. Some practices inevitably are fortunate or savvy enough to avoid any of the downsides as they navigate the changes in the industry. The practices that fail or morph into some other format do so because the stakeholders were simply not the ones with a better solution.
Each practice that ends up changing provides a useful case study and insight as to how and why the current approach and strategy did not sustain the practice. More often than not, the beliefs and strategies that got us to where we are today will not get us to where we want to be tomorrow. The best managers are serious students of the specialty. This is the lesson we must all take to heart. After all, anyone who suggests that managing an anesthesia practice is easy is a terrible liar or a terrible manager.

Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.