Fall 2021
Conflict and Governance
Will Latham, MBA
President Latham Consulting Group, Inc., Chattanooga, TN
Conflict naturally arises in every organization. Intelligent people can disagree.
Conflict can be useful in coming to the correct decision about an issue. On the other hand, conflict, and especially how individuals approach conflict, can have a significant negative impact on a group’s performance if they are not taken into account.
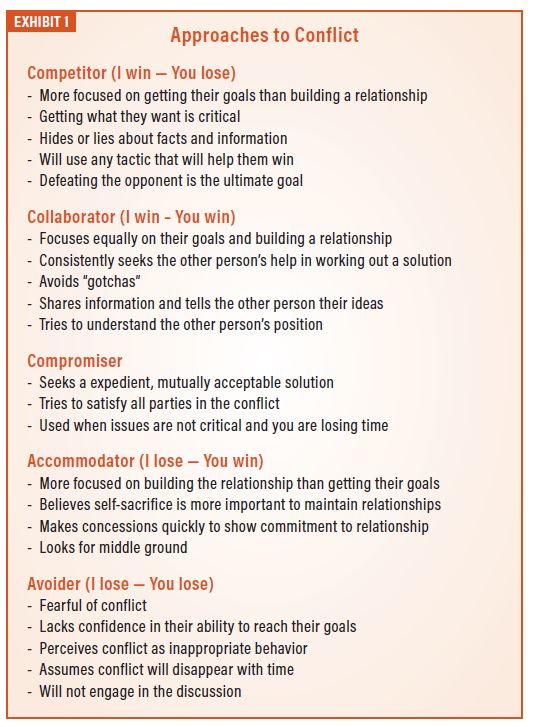
A well-known organizational development theory relates to how individuals approach conflict in group settings. One theory (developed by two organizational development psychologists, Kenneth W. Thomas and Ralph H. Kilmann) holds that there are five approaches an individual takes in dealing with conflict (see details in Exhibit 1):
- Competitor.
- Collaborator.
- Compromiser.
- Accommodator.
- Avoider.
Where do most anesthesiologists fall in regard to their conflict style? Although there is no anesthesiology-wide data, it has been our experience that most anesthesiologists are conflict avoiders. In fact we have actually worked with a number of anesthesiology groups who have used the Thomas-Kilmann Conflict Mode Instrument and we have consistently found that, in regard to physician-to-physician relations, 80 percent of the surveyed anesthesiologists are conflict avoiders.
What are the implications of this situation?
- Some group members are good with conflict, and others aren’t. Those that are comfortable often dominate group meetings while others try to become invisible.
- Those group members who are introverts or who are anxious about speaking in a group setting do all they can to avoid expressing their thoughts in group meetings.
- When the group votes on an issue, some are hesitant to raise their hands for fear they will be attacked by others.
- When someone doesn’t adhere to group decisions (often someone who is a competitor), no one wants to confront them.
It’s likely that your group has individuals with different styles, but because many or most group members are avoiders, your group should take this into account as it develops or modifies its system of governance. Here are some key steps that can improve group performance and overcome the negatives of avoidance.
Meeting Control – Ground Rules
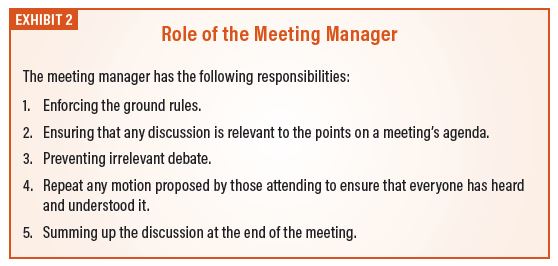
Every meeting should have someone designated as the meeting manager. This person should be charged with directing the meeting and have the responsibilities as outlined in Exhibit 2.
Further, the meeting manager should enforce meeting ground rules.
Why develop ground rules? Think about your most recent group meeting. Did the attendees exhibit any of the following behaviors?
- Some members never speak up, or speak up rarely.
- Multiple people talking at the same time.
- The conversation drifts way off topic.
- Interrupting telephone calls are taken in the meeting room.
- Participants arrive late.
- Low attendance.
- Some participate in the discussions, while others don’t (until the “after the meeting meeting”).
- Individuals raise many problems but do not pose solutions.
- There are many sidebar discussions— either by talking to the person seated next to them, or through texting.
To help eliminate these behaviors, the group should develop ground rules for group meetings. Ground rules are the observable behaviors that the group members agree are expected from every attendee. The focus is on observable behaviors.
Here is an example of an unobservable behavior: a ground rule that states that everyone is expected to “be openminded” is subject to dispute, depending on an individual’s viewpoint. Why? Because being open-minded occurs inside the brain and is not an indisputable observable behavior.
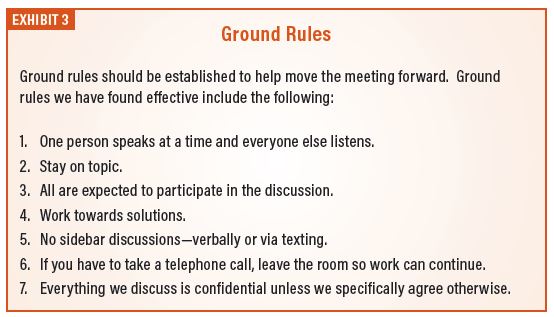
It’s best to set ground rules as a group process. In other words, you should have the attendees develop the ground rules together rather than copy the list in Exhibit 3 and say “here are our new ground rules. Individuals are more likely to adhere to the ground rules if they have a hand in developing them.
You should ask the attendees “what observable behaviors should be expected of each attendee?” Exhibit 3 provides an example of ground rules we have found to be effective.
Don’t Assume Consensus
Several years ago, we worked with a 25-physician group. Five members of the group were very comfortable with conflict and had great debates and discussion at their meetings. The other 20 were conflict avoiders and rarely spoke up. When they did speak up, they were often attacked by one or more of the five; so, over time, they spoke up less and less.
When the five appeared to reach agreement, the president said, “so it sounds like we have consensus on this issue; let’s move on to the next topic.” However, the reality was that the other 20 were not happy with the consensus but were not comfortable speaking up.
When a physician is at a meeting and is sitting quietly with his or her arms crossed, does he or she agree or disagree with consensus? He or she disagrees! They are just hesitant to speak up.
It is for this reason that we strongly suggest that groups formally vote on each-and-every issue, so they know how close they are to full agreement.
Use Secret Ballots for Voting
Many group meetings are longer than they need to be for the sole reason that group members are hesitant to raise their hand when voting. Why? They are conflict avoiders and fear criticism or retribution from other group members. They will do almost everything they can to delay or avoid a vote, so they don’t have to raise their hand and anger a colleague.
Therefore, we recommend that groups use “secret ballots” to vote on all issues. This can be done with 3 by 5 cards or a voting app.
Why are secret ballots useful?
- They allow the individuals to “vote their conscience” with less fear of retribution.
- They avoid one physician “bullying” another physician into changing their vote.
- They often speed up a meeting because people don’t delay voting to put off conflict.
Why do we suggest all issues instead of just controversial issues? If it is only used for controversial issues the group will be hesitant to implement it; and, when it is used, the “pucker factor” will rise considerably.
We have found that by using secret ballot, meeting times are cut by 30 to 50 percent.
Groups that use secret ballots for all their issues have told me that there is only one potentially negative outcome—that people will push too quickly for a vote. Therefore, it is up to the meeting manager to make sure that the group has had a full discussion of the issue prior to voting.
Use Anonymous Surveys
 Conflict avoiders find it difficult to speak up in group meetings. That’s why whenever we facilitate a meeting we always interview or survey participants ahead of the meeting. We have found that conflict avoiding physicians are great at hiding their thoughts during meetings.
Conflict avoiders find it difficult to speak up in group meetings. That’s why whenever we facilitate a meeting we always interview or survey participants ahead of the meeting. We have found that conflict avoiding physicians are great at hiding their thoughts during meetings.
The most successful anesthesia groups we know of utilize anonymous surveys, sometimes about specific issues and sometimes to take the general temperature of the organization. Anonymous surveys allow important issues to get on the table that would otherwise not come to light in the meeting.
Develop a Code of Conduct to Deal with Disruptive Physicians
Conflict avoidance is not limited to the general membership of an anesthesiology group—most group leaders don’t enjoy conflict, even though they know it is necessary at certain times.
One of the most challenging aspects of group leadership is dealing with disruptive physician behavior. To make life easier on the leaders (and ultimately the whole group) the group should develop a code of conduct.
A code of conduct sets out, in general terms, the standards of behaviors expected of the members of the group. Such a code is created for the following reasons:
- As a vehicle to communicate what the group finds important about physician behavior and conduct.
- As a method to improve the chances that the group will continue to have the freedom to govern itself.
- As a method to hold errant physicians in check without making them feel they are under personal attack.
- To remove personalities and private opinions if it becomes necessary to intervene in a situation.
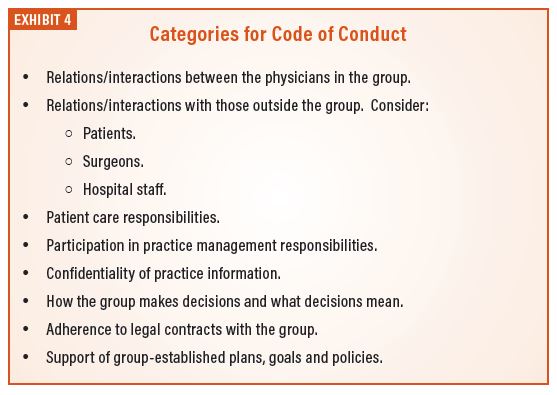
When developing the answers to these questions, it is useful to break down the answers into various categories, such as shown in Exhibit 4.
This tool gives group leaders something to “hang their hat on” when they must confront disruptive behavior. It’s no longer “your opinion versus my opinion” as it concerns appropriate behavior. Instead, the discussion becomes “here is what you are doing as compared to what we agreed upon as our code of conduct.”
What is the best way to develop a code of conduct? The most important step is to include all the physicians in its development. If they are not involved, the physicians will see the document as something imposed on them and therefore will be less likely to adhere to the agreements. The best time to develop a code of conduct is during the group’s annual planning retreat. If physician misbehavior is particularly acute, the group might consider a separate meeting to address just the code of conduct.
Conflict
Once again, conflict in any organization is natural. The best performing groups understand that physicians tend to be conflict avoiders and develop governance policies and processes that take this into account.

For more than 30 years, Will Latham, MBA has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 135 medical practices representing over 1,300 physicians. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at wlatham@lathamconsulting.com.