Summer 2020
Internal Audits: Process and Frequency
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I
Perfect Office Solutions, Inc., Leesburg, FL
Many practices are too busy with day-to-day work to keep track of how often they should conduct internal audits. However, if your practice has a compliance plan, it generally outlines the required audit frequency. Do you know what your compliance plan requires?
 If your anesthesiology practice is still using the compliance plan outline published in September 1997 by the American Society of Anesthesiologists™ in Compliance With Medicare and Other Payor Billing Requirements, your practice is required to review pre-submissions (claims reviewed before filing to the insurance carrier) on a quarterly basis, and post-submission (claims reviewed after filing to the insurance carrier) at regular intervals, such as semi-annually. You may also want to consider updating your compliance plan to ensure it meets current standards.
If your anesthesiology practice is still using the compliance plan outline published in September 1997 by the American Society of Anesthesiologists™ in Compliance With Medicare and Other Payor Billing Requirements, your practice is required to review pre-submissions (claims reviewed before filing to the insurance carrier) on a quarterly basis, and post-submission (claims reviewed after filing to the insurance carrier) at regular intervals, such as semi-annually. You may also want to consider updating your compliance plan to ensure it meets current standards.
How to Prepare for Audit
Having anesthesia records available as you start your internal audit will make the review process easier. If anesthesia records are not available, you should obtain them from the hospital’s medical records department.
An internal audit is simply an objective review of the anesthesia services billed to monitor the accuracy and suitability of claims. It should be performed by a qualified employee—such as the office administrator, manager, a certified coder (other than the employee who coded the services), the compliance officer, a physician or a combination of staff members.
Each practice determines the number of charges or percentage of claims to be reviewed for each provider. It also determines how to make appropriate corrections and, depending on the internal audit results and compliance plan requirements (when applicable), whether to contact legal counsel. Although the standard compliance plan requires the practice to discuss all claims monitoring with legal counsel, the practice may modify the plan to require legal counsel consultation only during external audits.
A simple pre-submission review should compare the codes and modifiers billed with the documentation on file. Because the auditor reviews this information before submitting the claim, corrections are made during the review process, and corrective actions are taken and conveyed to staff. For example, a review determined the coder mistook “TKA” for a total knee arthroscopy (01400, base value - 4), rather than a total knee arthroplasty (01402, base value - 7). The practice must take several corrective steps:
- Change code, if applicable. Make certain what procedure was performed as different clinical staff may be using different acronyms;
- Ensure acronyms in your practice are clearly defined; and
- Request a report of 01400 and 01402 claims filed to verify accuracy. Choose your time frame based on payer policy and timely filing requirements, such as one year or 90 days.
A post-submission review is more complex and should include a review from the time the claim is entered all the way through resolution. Choose a date within the past six months; and, in addition to checking codes and modifiers used, review payment processes to ensure correct payments were received and appropriate adjustments were taken. Each practice should know exactly what payment to expect from each payer. Medicare pays by location and the amount is standard; other payers may be contracted using various amounts and time calculation techniques, so a matrix of expected reimbursement is helpful. At the very least, a form listing annual expected amounts is necessary.
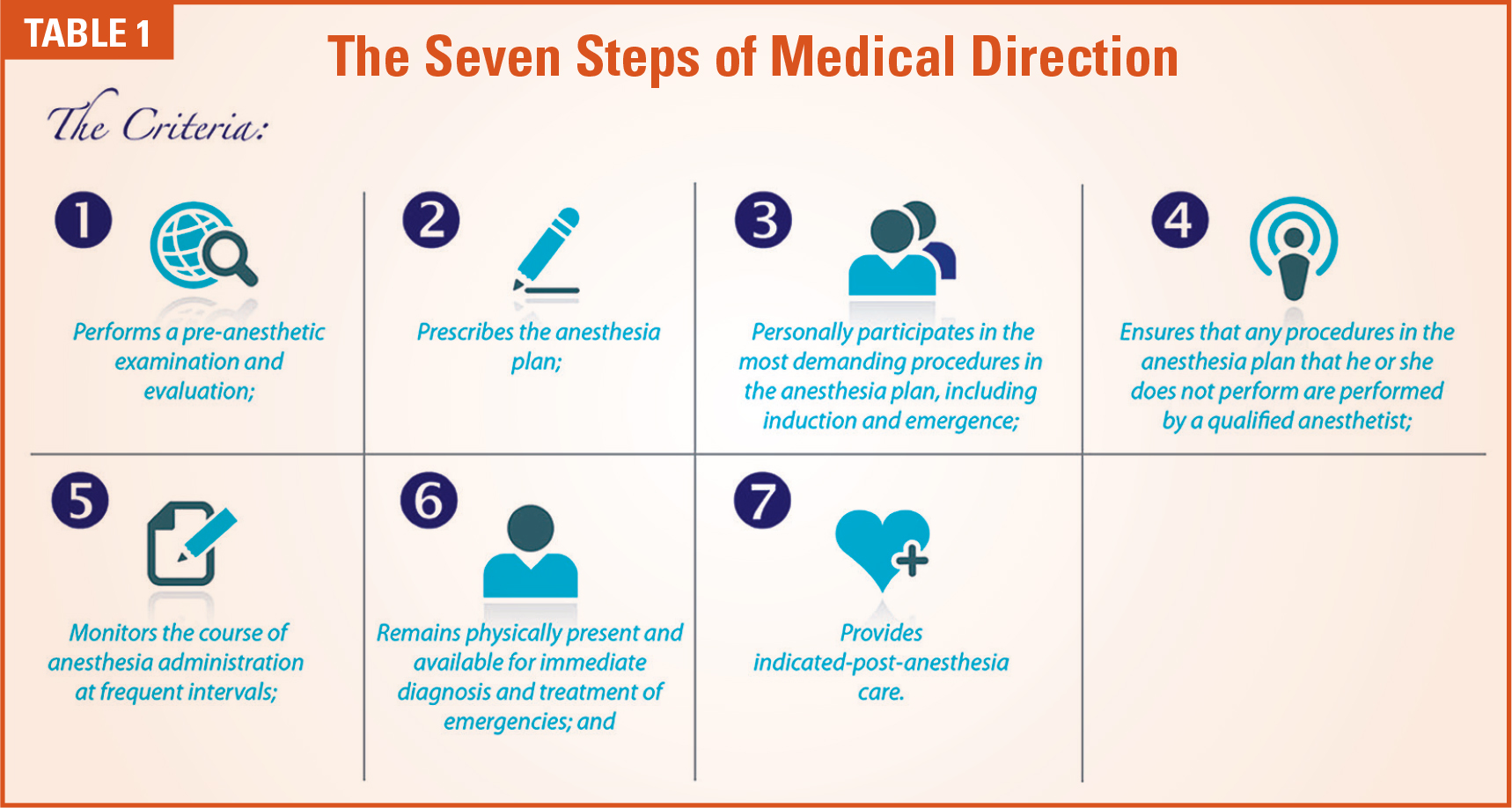
Payment will be made at the medically directed rate if the physician medically directs qualified individuals (all of whom could be CRNAs, anesthesiologists’ assistants, interns, residents or combinations of these individuals) in two, three, or four concurrent cases and the physician performs the following activities.
The physician must document in the medical record that he or she performed the pre-anesthetic examination and evaluation. Physicians must also document that they provided indicated post-anesthesia care, were present during some portion of the anesthesia monitoring and were present during the most demanding procedures in the anesthesia plan, including induction and emergence, where indicated. (Source: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf)
An important area to review is concurrency and documentation of medical direction criteria. (See Tables 1 and 2). Depending on the software concurrency reporting capabilities, it may be necessary to review an entire day of concurrency if your practice includes residents, certified registered nurse anesthetists, anesthesia assistants or student registered nurse anesthetists. It is important to understand that concurrency calculations must include all patients, regardless of type of insurance. While some carriers allow a combination of up to four concurrent cases, graduate medical rules differ and allow up to two cases when residents or SRNAs are involved.
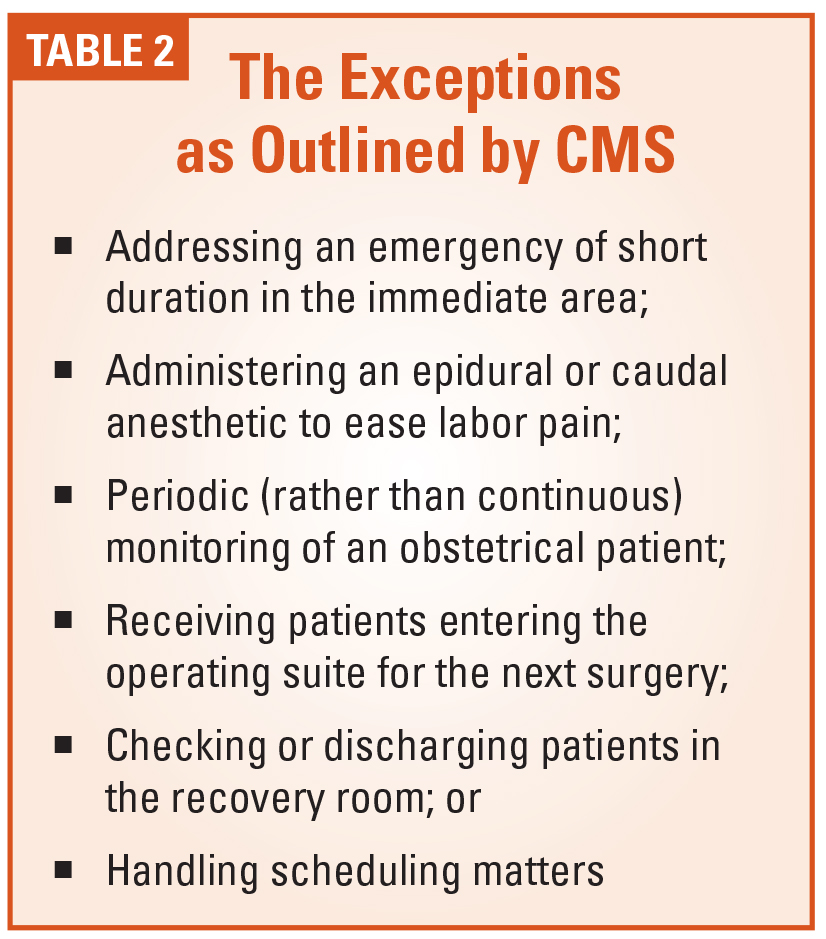
A physician who is concurrently furnishing services that meet the requirements for payment at the medically directed rate cannot ordinarily be involved in furnishing additional services to other patients. Nevertheless, engaging in activities described in Table 2 do not substantially diminish the scope of control exercised by the physician and do not constitute a separate service for the purpose of determining whether the requirements for payment at the medically directed rate are met.(Source: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf)
Whether conducting a pre- or postsubmission review, keep documentation of all steps taken in a compliance file. Even if your practice only reviews once a year, make certain the time frame agrees with the written compliance plan, when applicable. The adage, “It is better not to have a compliance plan, than to have one and not follow it,” is particularly true for anesthesia practices, as anesthesia billing rules are often vague and ambiguous.
Note: Novitas and other Medicare Administrative Contractors may allow additional exceptions. For example, Novitas indicates “An anesthesiologist may perform and, if otherwise eligible, seek reimbursement for procedures (such as arterial line insertions, central venous catheter insertions, pulmonary artery catheter insertions, and epidural, spinal, and peripheral nerve blocks) performed in an area immediately available to the operating room when performance of such services does not prevent him/her from being immediately available to respond to the needs of surgical patients.”
 Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I, has over 36 years of experience in anesthesia coding and billing and speaks about anesthesia issues nationally. She has a Masters Degree in Business Administration, is a certified coder and instructor through the American Academy of Professional Coders. Kelly is an Advanced Coding Specialist through the Board of Medical Specialty Coding and served as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November 2001. She can be reached at kellyddennis@attglobal.net.
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I, has over 36 years of experience in anesthesia coding and billing and speaks about anesthesia issues nationally. She has a Masters Degree in Business Administration, is a certified coder and instructor through the American Academy of Professional Coders. Kelly is an Advanced Coding Specialist through the Board of Medical Specialty Coding and served as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November 2001. She can be reached at kellyddennis@attglobal.net.