Summer 2020
Governance Traps and Tricks
Will Latham, MBA, President
Latham Consulting Group, Inc., Chattanooga, TN
In today’s challenging times, effective group governance takes on even greater importance. If a group cannot develop plans, make decisions and implement its plans, someone else will choose the course of the group.
Following are some governance challenges that clients have approached us with over the last year.
Speed Bump
The Problem:
 “Our group revisits issues over and over again. We have members of the group who, if they do not get their way in the first vote, raise the issue over and over again to either torture the group into changing the decision, or to paralyze the group.”
“Our group revisits issues over and over again. We have members of the group who, if they do not get their way in the first vote, raise the issue over and over again to either torture the group into changing the decision, or to paralyze the group.”
The Solution:
One way to reduce the use of this “torture” technique is to implement a “speed bump” for items to return to the agenda for discussion.
For example, the group could implement a policy that requires 30 percent of the shareholders to sign a document asking to bring an item back to the floor for re-discussion once a decision has been made (it is important that they sign a document, rather than someone say “I had 30 percent of the people say they’d like to re-discuss this issue”).
This policy doesn’t close the door to re-discussing an issue (if more than 30 percent want to re-discuss an issue, the group probably should). However, it will typically reduce the number of times this “torture” technique is used.
Reduce Disruptive Behavior
The Problem:
“Our group has several disruptive physicians and we have not been able to deal with or even confront them. This job falls to the group leadership, and it’s the last thing they want to deal with. Even if they take on the disruptive physician, it is often an argument over who should decide what appropriate behavior should be.”
The Solution:
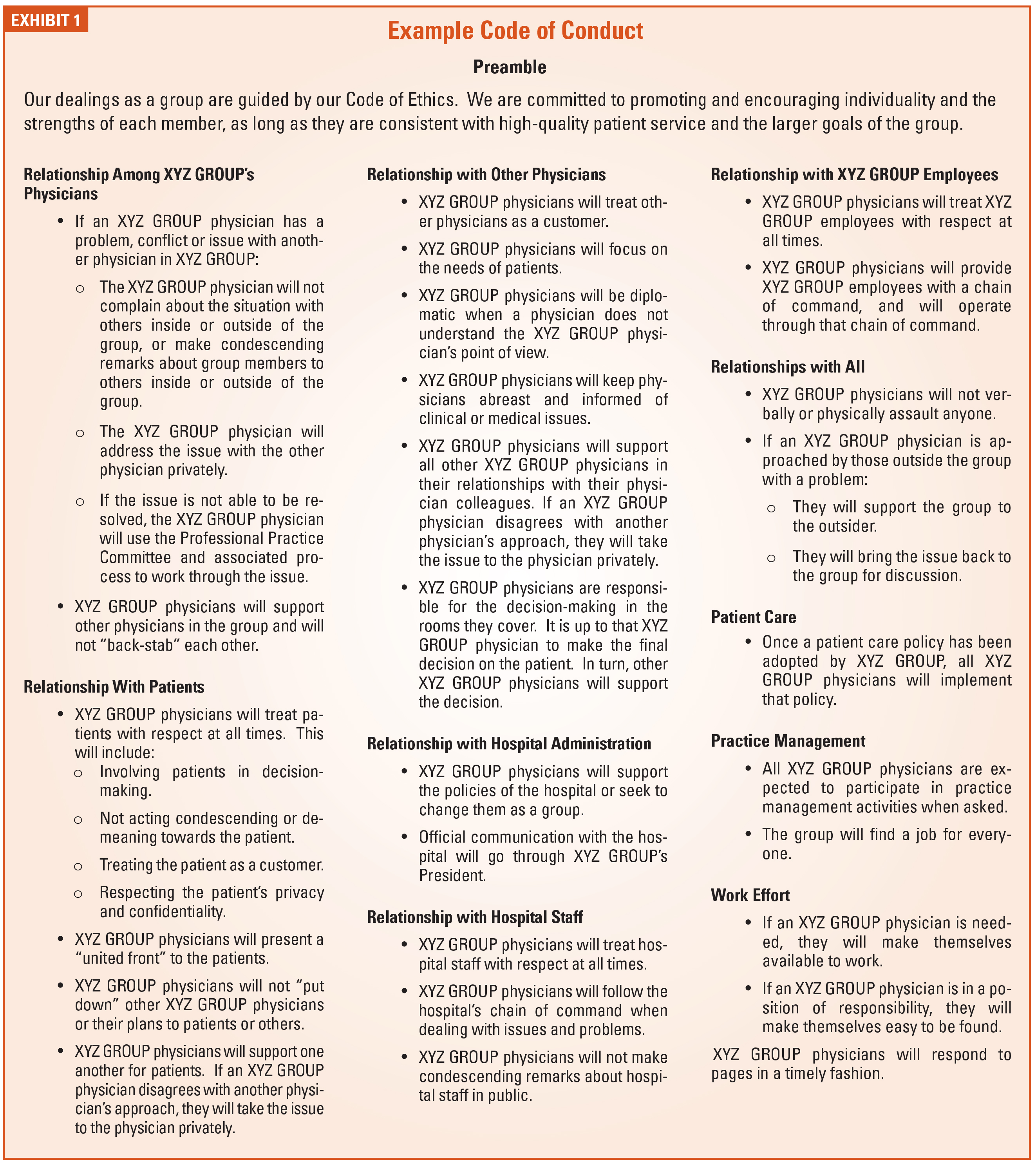
 One way to address this situation is for the group to develop a “Code of Conduct.”
One way to address this situation is for the group to develop a “Code of Conduct.”
A Code of Conduct indicates the agreed upon standards of behavior expected of a member of the group. It sets out, in general terms, the standards and duties which are reasonable to expect a member of the group to observe.
Properly developed, this document can be used to effectively reign in problematic physician behavior. Everyone has fair warning about what the agreed upon expectations are. Toleration for outliers is reduced. Group leadership can act because an intervention is no longer seen as one person’s opinion versus another’s.
We believe that the group should set expectations in a number of areas, to include:
- Relations/interactions between group physicians.
- Relations/interactions with group employees.
- Relations/interactions with those outside the group.
- Patients and patient care.
- Participation in practice management responsibilities.
- Confidentiality of practice information.
- Support of group decisions, established goals and policies.
For each area the group should answer the following questions:
- What behaviors do we expect of each other? What is acceptable to us?
- What is inappropriate?
- What are some of the “unwritten rules” that guide our behavior?
- What are the rights and responsibilities of each physician?
An example Code of Conduct can be found in Exhibit 1.
Use Committees to Share the Load
The Problem:
“Our Board is overloaded. Most of the shareholders are uninvolved, except to veto items or complain. We have committees, but they don’t function well.”
The Solution:
We have found that the best medical group Boards use their committees to process information prior to the Board addressing an item. When an item is raised at the Board level, their first step is often to send it to a committee to:
- Define the scope of the issue.
- Gather needed data.
- Analyze the data.
- Recommend a solution.
 Once the committee has developed a solution or recommendation, this information should be presented to the Board. However, the Board must be extremely careful to not redo the work of the committee. If the Board feels the committee has not completed the assignment, it should be sent back to the committee for further work.
Once the committee has developed a solution or recommendation, this information should be presented to the Board. However, the Board must be extremely careful to not redo the work of the committee. If the Board feels the committee has not completed the assignment, it should be sent back to the committee for further work.
In addition, the Board should make every effort to accept the committee’s recommendation. Why? If the Board always rejects the committees’ recommendations or re-does the work, the committees will reach the conclusion that their thoughts are not being considered and stop doing the work.
Conflict Avoidance and Voting
The Problem:
“Our meetings go on and on forever. Some group members keep talking and talking, while others sit in silence. And when we vote, people seem reluctant to raise their hand and express their true opinion.”
The Solution:
In our experience physicians tend to be conflict avoiders when it comes to their peers. Sometimes discussions go on and on because people don’t want to raise their hands to vote and possibly enter into conflict with those that don’t agree with them. This can make meetings last much longer than they need to.
To deal with conflict avoidance, we are seeing more and more groups move to using “secret ballots” for their voting process. Most groups use secret ballots for electing their Board and officers, but some groups use them when they need to vote on controversial issues, or in some cases, all issues.
Why are secret ballots useful?
- They allow the individuals to “vote their conscience” with less fear of retribution.
- They avoid one physician “bullying” another physician into changing their vote.
- They often speed up a meeting because people don’t delay voting to put off conflict.
There are several ways to implement secret ballots—here are two:
- Use 3 x 5 cards as the secret ballots.
- I have observed some groups starting to use “audience response systems.” Some of these are apps on smartphones while others utilize dedicated voting devices. A group we worked with recently moved to using such a voting system for all issues. They found that this has cut 25 - 50 percent off the time of every meeting by using secret ballot.
Authority
The Problem:
“We have created an Executive Committee of three physicians and given them significant authority. However, they will not make decisions within the bounds of their authority because they are afraid of second guessing by the other physicians. What can we do?”
The Solution:
There’s no doubt about it, serving as a leader in a physician group is a tough job. Decisions will be second-guessed, and some people will not like any decision that is made. Here are several suggestions:

- First, the leadership must recognize that criticism comes with the job—if they can’t take it or expect it not to exist, they should avoid serving as a leader.
- The leadership must help each other develop the mindset that it is their job to make these tough decisions, and then stick up for each other in front of the larger group.
- If the larger group continually second guesses the authority of the leadership, the group at large should re-discuss what level of authority they are truly willing to give the leadership.
- In some cases, leaders are afraid to make decisions because any decision can be recalled to the larger group for another vote by the members at large. Naturally, this defeats the purpose of a governance structure. For group’s with this problem, they should consider a provision that requires a two-thirds majority of the shareholders to even bring up for discussion an issue decided within the authority of the leadership.
Critical Time
These are unprecedented times for anesthesiology groups. The challenges are greater than ever, as is the need for effective group governance.
If your group suffers from any of the problems mentioned in this article, we suggest you seriously consider implementing the solutions offered. The anesthesiology groups that have implemented these ideas have found their ability to make decisions and move forward to be greatly strengthened.
 For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at WLatham@LathamConsulting.com.
For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at WLatham@LathamConsulting.com.