Winter 2020
What Determines the Cost of Anesthesia Care?
Jody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services Anesthesia Business Consultants, LLC, Jackson, MI
 The cost of anesthesia care has become one of the most significant issues in the management of today’s anesthesia practices. This is not to say that quality of care is not important, but it has become a given. Ultimately the essential challenge facing virtually all practices is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the needs of the facility or facilities being served. The problem is that the options for generating more revenue are limited to three: enhancing fee-for-service collections; generating additional revenue from new services, such as nerve blocks and ultrasonic guidance for postop pain management; and negotiating subsidy support from the facility. None of these constitutes a quick or definitive fix.
The cost of anesthesia care has become one of the most significant issues in the management of today’s anesthesia practices. This is not to say that quality of care is not important, but it has become a given. Ultimately the essential challenge facing virtually all practices is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the needs of the facility or facilities being served. The problem is that the options for generating more revenue are limited to three: enhancing fee-for-service collections; generating additional revenue from new services, such as nerve blocks and ultrasonic guidance for postop pain management; and negotiating subsidy support from the facility. None of these constitutes a quick or definitive fix.
The largest expense for any practice is the cost of providers. The most obvious way to reduce the cost of care is to either reduce the number of providers needed or modify the staffing model. Physician-only practices may want to consider bringing on CRNAs. Care-team practices may want to consider increasing the number of CRNAs. Although changing the configuration of the team might appear simple, especially to those hospital administrators who don’t want to increase the stipend, there are many considerations that must be carefully weighed. Reducing the number of one category of provider in order to increase the number of another can be very disruptive and become the anesthesia equivalent of voting members off the island. Such adjustments to the staffing model really only work when they are implemented over time, based on attrition.
Practical and logistical considerations aside, how should one evaluate the impact of a given staffing model? What is the appropriate metric? How should it be calculated? What is a reasonable benchmark? Since one cannot manage what one cannot measure, the logical place to start is with a calculation of cost. To be useful this must represent a normalized metric, such as cost per anesthetizing location day.
Suppose the coverage requirement consists of seven locations (four ORs, two Endo rooms and one OB), Monday through Friday, and three on the weekend (an elective room on Saturday, plus one call person each night). Given the current environment, there are three basic staffing options: a physician-only model; a traditional medical direction model, with one physician medically directing three CRNAs; and a non-medical direction model, where one physician may oversee five or six CRNAs—a model that is becoming more common in the 17 opt-out states. The financial implications of each model are summarized in the three tables below. It should be noted that in any particular practice scenario there may be multiple variables that could change the outcome. A physician cost of $475,000 may be high in some markets and low in others. Similarly, CRNA compensation varies considerably across the country. Staffing models may also vary. Obviously, the more providers that are required, the higher the cost per provider day will be. A number of factors determine the staffing model, but historical precedent is often the most significant. Changes in staffing model occur most often when a contract changes hands and a new staffing entity proposes a new staffing model.
 In any pro forma model the assumptions are critical and can have a significant impact on the result of the calculations. This model assumes a small community hospital where some of the ORs may run late but where the average room runs about eight hours. OB is unpredictable but tends not to be very busy.
In any pro forma model the assumptions are critical and can have a significant impact on the result of the calculations. This model assumes a small community hospital where some of the ORs may run late but where the average room runs about eight hours. OB is unpredictable but tends not to be very busy.
The key to the validity of any analytical model is the reasonableness of the assumptions. The models presented below make some simple and generic assumptions for purposes of demonstrating the dramatic impact staffing changes can have on a practice but the reality of any specific practice analysis, especially those that are larger, and especially those that cover a variety of venue types, can be far more complex.
The Physician-Only Model
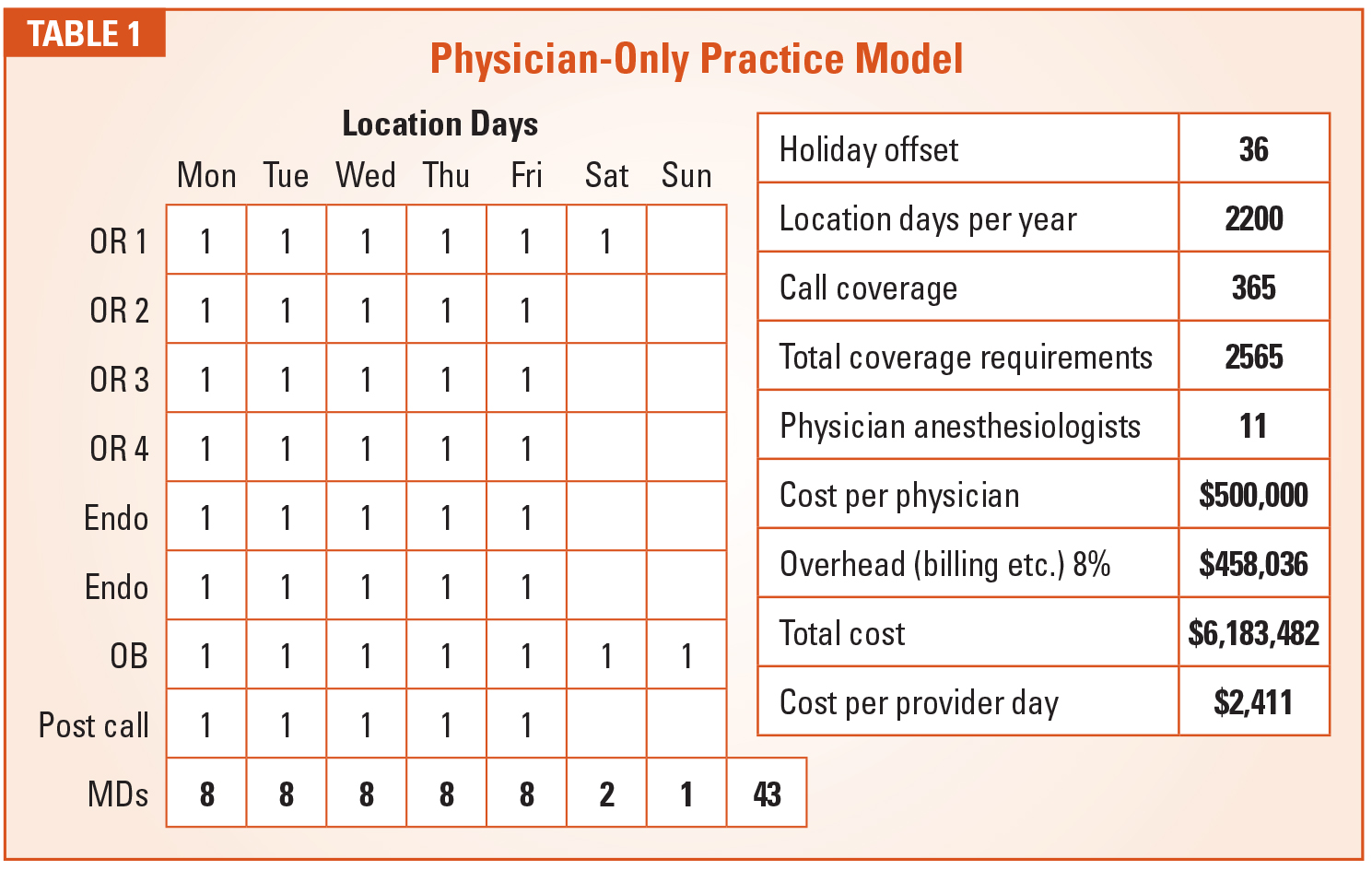
The first question is what is the optimum number of providers? The typical full-time anesthesiologist now gets an average of eight weeks of vacation. Thus, they are available for 215 days per year (365 minus 104 weekend days, 40 vacation days and 6 holidays). There are two ways to calculate the number of physicians needed: the simple method is based on the number of provider days needed divided by 215. A more refined model is based on hours of coverage divided by 21,500 or 10 hours per day. Most claim they work at least fifty hours per week, although this may not adequately allow for the impact of call. CRNAS, by contrast, typically get six weeks of vacation and work five eight-hour shifts, or a total of 40 hours per week.
The physician-only model (Table 1) is based on this calculation and an assumption that the average total compensation package, which includes the cost of malpractice and benefits, is probably about $500,000 nationwide at the current time. This is what groups need to offer to recruit and retain qualified providers. As the calculations indicate, a physician-only practice is a very expensive model. To support this staffing model, the providers would need to consistently generate 60 billable units a day at a net yield of $40 per unit, which is well beyond what most anesthesiologists actually generate. A shortfall would necessitate the need for financial support from the facility, and very few are willing to subsidize a physician- only staffing model.
The Medical Direction Model
 There are some ways to reduce the cost of care for a physician-only model. Including non-shareholder providers who get paid at a lower rate may help some. The use of independent contractors who only have to be paid when they work may also be helpful.
There are some ways to reduce the cost of care for a physician-only model. Including non-shareholder providers who get paid at a lower rate may help some. The use of independent contractors who only have to be paid when they work may also be helpful.
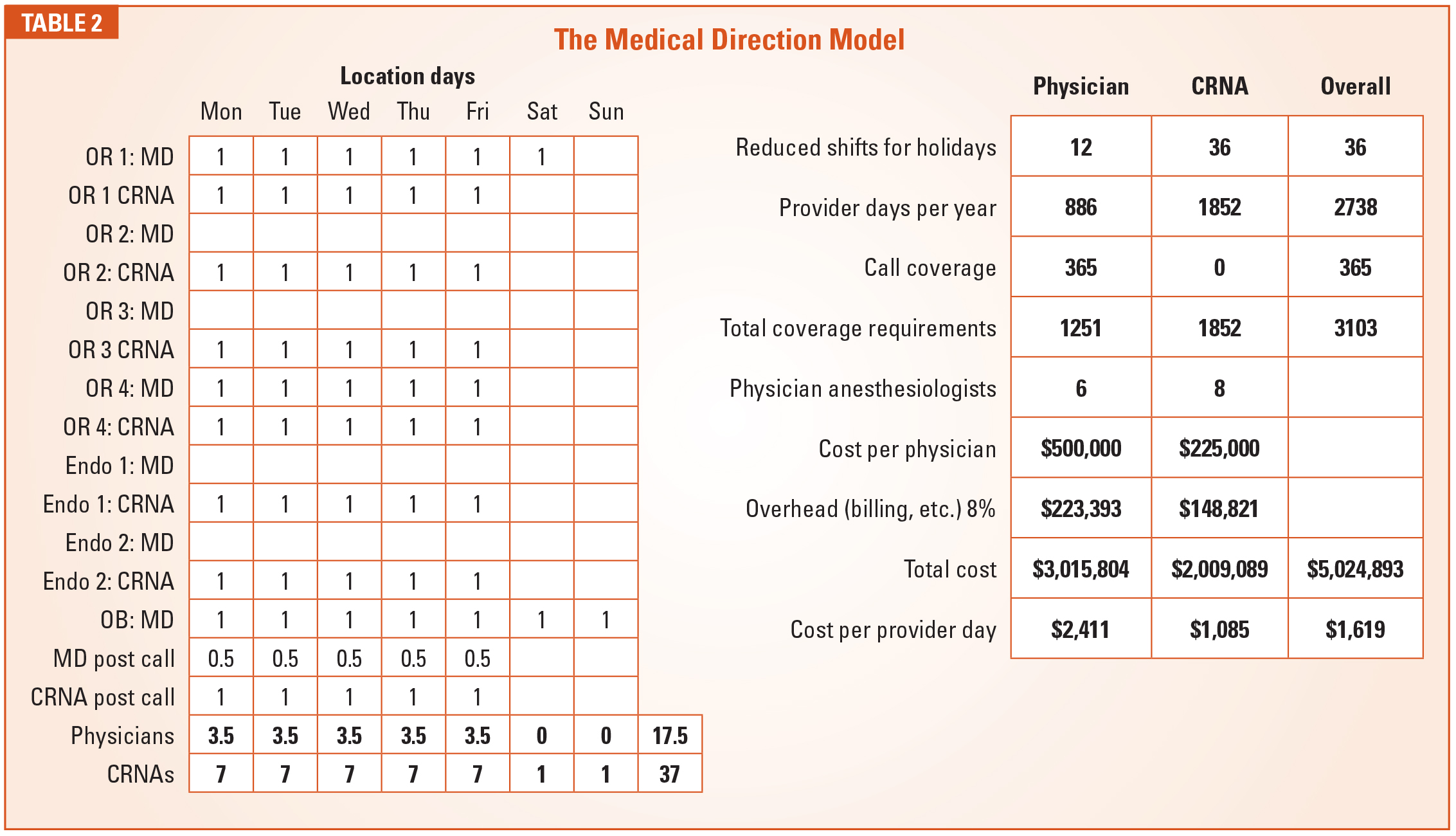
At least 75 percent of all anesthesia care provided in the United States is administered by CRNAs, and the majority of these are medically directed by physicians. Traditional medical direction guidelines limit the number of CRNAs a physician anesthesiologist may manage at any point in time to four. As a practical matter, most medically directing anesthesiologists routinely oversee between two and three CRNAs at a time. The more a physician’s time is leveraged, the more cost-effective the model; but practical and logistical considerations are usually the rate-limiting factor.
The model (Table 2) assumes two physicians medically directing six CRNAs in the ORs and the endoscopy units, and one working alone in Obstetrics. The table lays out the proposed coverage pattern and the calculation of the number of providers needed. What this shows is that the use of CRNAs allows for an offset to the daily cost of a physician. The CRNA cost of $1,085 dramatically impacts the overall cost per anesthetizing location day from $2,411 to $1,619 or an overall cost savings of $1,417,433.
A Caveat
There are two primary reasons why care-team practices may not realize the savings indicated above. First, they may have too many physicians, meaning that the cost of each physician is not offset appropriately by the cost of the CRNAs. Second, they may have too many one-to-one or one-to-two scenarios. The real cost savings is only realized at levels of one MD to three CRNAs.
With the introduction of the concept of opt-out states we now see a third model: the physician oversight model. Since CRNAs in opt-out states no longer need to be medically directed, an increasing number of practices, especially in the West, are allowing CRNAs to work independently with minimal physician oversight and no strict medical direction. This allows for the reduction of the number of physicians in the model.
The Physician Oversight Model
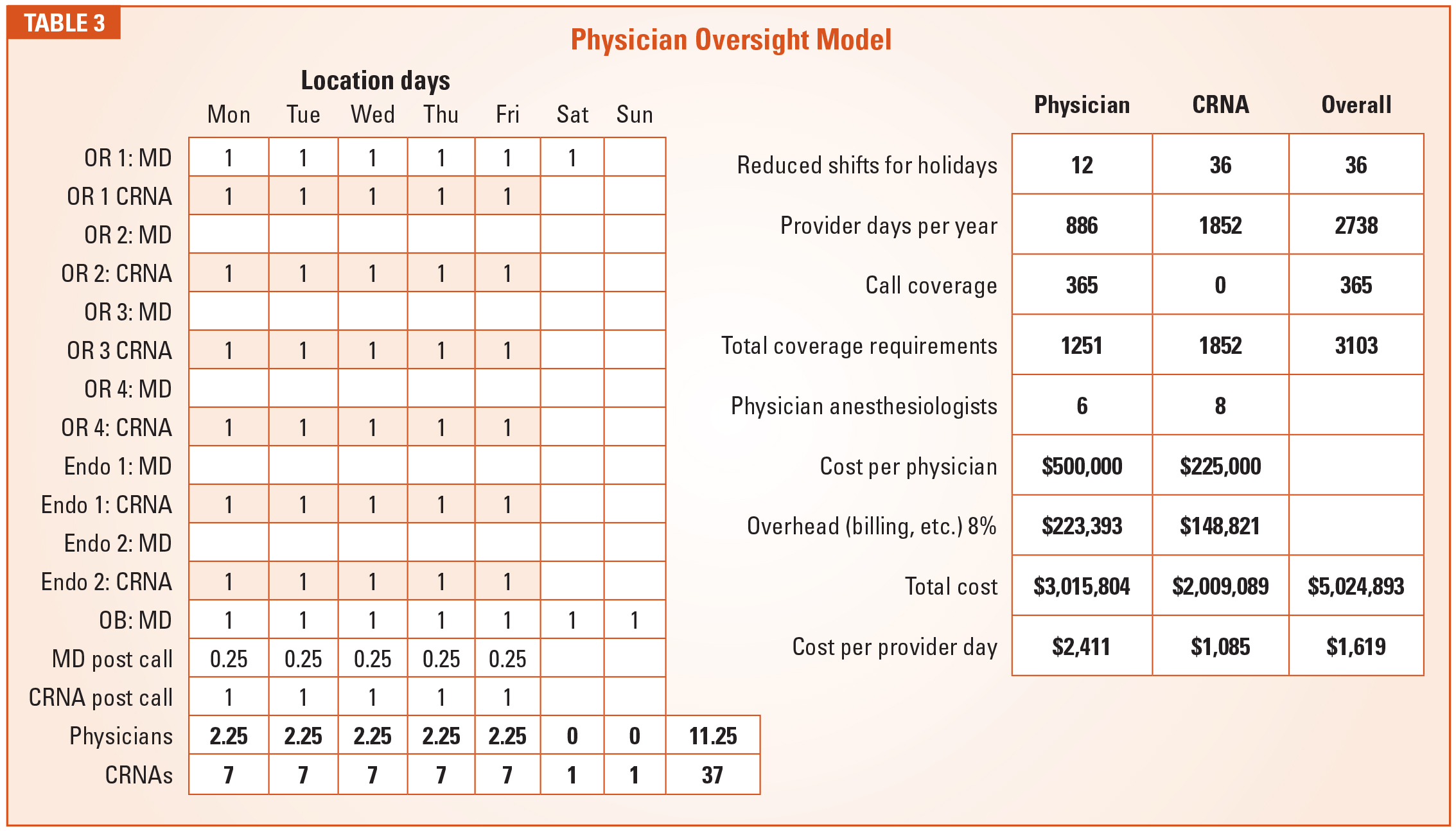
As the data (Table 3) demonstrates, modification of the staffing model can have a dramatic and meaningful impact on the cost of anesthesia care. It explains why hospital administrators who are negotiating with physician-only practices always ask first if the practice has considered a CRNA option. Sometimes, the CRNA approach will save money, but sometimes it is simply not applicable to the type of care required or consistent with the culture of the institution. This is when practices have to start thinking outside the box and look for other ways to reinvent their group configuration and financial model.
The most common problem is that coverage requirements have outstripped the revenue potential of the practice. Hospitals tend to see availability to surgeons, which is an expensive commodity for the anesthesia practice that incurs the cost of a provider every time a room is opened whether or not the room is productive. Let’s pick a number, say 50 ASA units per location day. Suppose the hospital minimizes the number of rooms that do not meet this target. If minimizing the number of unproductive rooms allows for a reduction in anesthesia staffing, the result could be significant.
 We often say that the anesthesia department has more and better data about what happens in the operating rooms each day than any other department in the hospital. The question is whether the practice is using this data effectively to help the administration run the operating rooms more efficiently. This is becoming one of the new frontiers for the specialty. Sharing operating room utilization data is not going to be a quick fix to under-utilization, but its value cannot be ignored. Anesthesia providers need to be seen as team players in the management of the operating rooms and delivery suites. The more active a role they play, the more it will ultimately benefit their practice. This is the kind of out-of-the-box thinking that anesthesia practices should be pursuing as the cost of care becomes an ever more important factor in determining where patients get directed for the procedures they need.
We often say that the anesthesia department has more and better data about what happens in the operating rooms each day than any other department in the hospital. The question is whether the practice is using this data effectively to help the administration run the operating rooms more efficiently. This is becoming one of the new frontiers for the specialty. Sharing operating room utilization data is not going to be a quick fix to under-utilization, but its value cannot be ignored. Anesthesia providers need to be seen as team players in the management of the operating rooms and delivery suites. The more active a role they play, the more it will ultimately benefit their practice. This is the kind of out-of-the-box thinking that anesthesia practices should be pursuing as the cost of care becomes an ever more important factor in determining where patients get directed for the procedures they need.
 Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.
Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.