Winter 2020
Chaos to Clarity: Resolving Strategic Issues
Will Latham, MBA
President, Latham Consulting Group, Inc., Chattanooga, TN
 Anesthesiology groups operate in a rapidly changing environment. The specialty faces many challenges, including pressure on reimbursement, hospital consolidation and the threat of consolidators.
Anesthesiology groups operate in a rapidly changing environment. The specialty faces many challenges, including pressure on reimbursement, hospital consolidation and the threat of consolidators.
Amazingly, many anesthesiology groups attempt to navigate these troubled waters without an agreed-upon plan. In most cases, most of a physician’s livelihood (his or her work, his or her compensation) is tied up in their practice, yet many resist spending one day a year developing an agreed-upon plan for the future of their organization.
So, let’s review what groups work on at such planning retreats, and then discuss how groups approach a planning process.
Key Issues
Although groups face a number of similar challenges and key issues, their answers to such issues and their plans differ based on their particular situation. Here are some of the issues that we see anesthesiology groups wrestle with:
- Independence: Is it our goal to remain independent? If so, what strategies will we need to implement to continue to be independent? If not, what criteria should we use to select a partner?
- Current Relationships: What is the status of our relationship with those we provide service to? Could such relationships be strengthened? If so, how?
- Geographic Coverage: What geographic area do we intend to cover as a group? What are the benefits of pursuing new business? What is our approach to new business: avoid opportunities, respond to requests, vigorously pursue?
- Size of the Group: How large will the group become? Will we grow to fill the service needs of the market, or will we set an upper-end limit on the number of physicians in the group?
- Mergers: Should the group consider/ pursue mergers with other anesthesiology groups in the region? What advantages would such mergers provide?
- Recruitment: Where do we stand in regards to our staffing needs and work/life balance? Are we “fat,” or are we “thin”? Are we where we want to be in regards to staffing? Should we consider alternative work arrangements?
- Shareholder Track: Will the group continue to add anesthesiologists on a shareholder track, or will it have long-term employed physicians? Will the group limit the number of shareholders? What expectations (beyond quality clinical care) will be required to become a voting shareholder?
- Governance: Does our current governance system meet the needs of our current organization? Do we need to give authority to a smaller group to make certain decisions? What authority should be given? Do we have effective means to deal with disruptive physicians? How can we improve communication? Do we have a succession planning process in place?
- Compensation/Call: Is our compensation system achieving the goals of the group? Is our call fair and reasonable?
Two things to note:
- These are not all the issues that we see discussed, only the most common ones.
- You will note that the questions have been provided but not the answers. As previously mentioned, the answers depend on your situation. Getting to the answers for your group is what a strategic planning process is all about.
Strategic Planning Process
Most groups’ strategic planning effort revolves around a weekend retreat of one or two days, where the members of the group meet to discuss and resolve key issues and map out a plan for the future.
The time at the retreat is the most valuable time (getting everyone together is often a challenge) and the most expensive (multiply the number of people in the room times an estimated hourly rate); and, therefore, it is essential that the group utilize the time at the retreat effectively. To do so, the physicians should be interviewed or surveyed prior to the meeting, asking them the following questions:
- What do you see as the major strengths of the group? What is working well?
- What are its major weaknesses? What is not working well?
- What is going on in the environment that might represent opportunities for, or threats to, the group?
- How do you expect the local healthcare market to change over the next five years and how should your practice operate in that environment?
- What issues do you think the group should address at the planning retreat?
Those leading the planning process should review the results of the interviews/surveys for common themes, identify the key issues to be addressed and develop a set of work papers to guide the retreat.
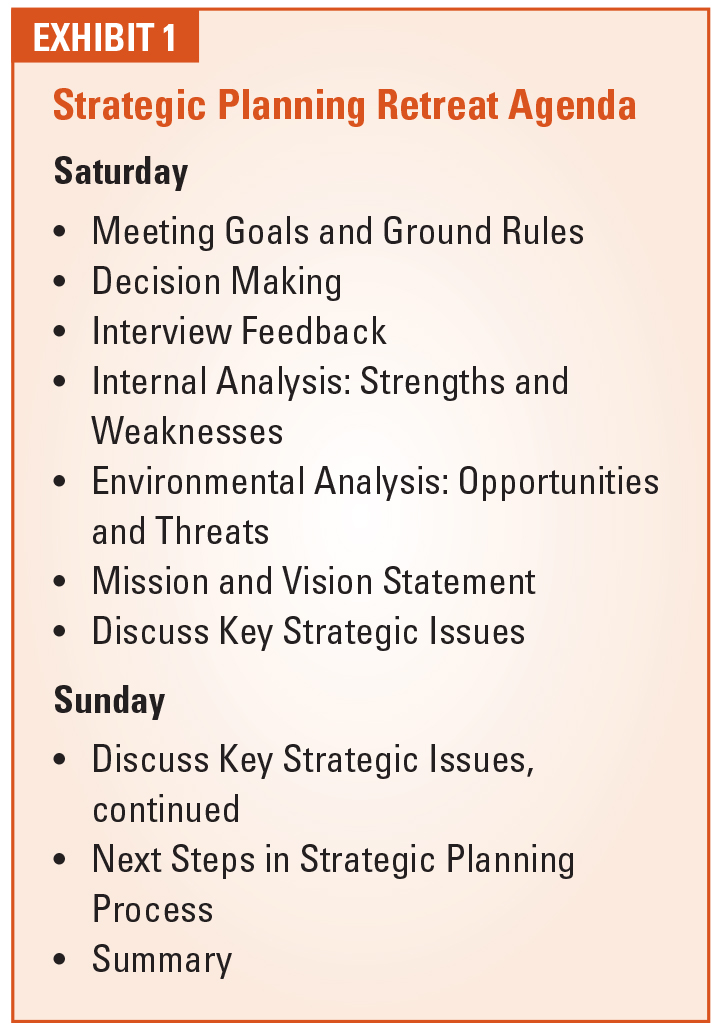
The retreat itself typically follows the schedule as shown in Exhibit 1. There are two parts of this process to emphasize—ground rules and decisions.
Ground Rules
Most group meetings of anesthesiologists do not work very effectively. Discussions get sidetracked. Some individuals dominate the conversation, while others do not speak at all. People make telephone calls or do other disruptive activities during the meeting. Therefore, it is critical that one of the first things the group should do is agree on a set of rules that the “meeting manager” will use to manage the meeting.
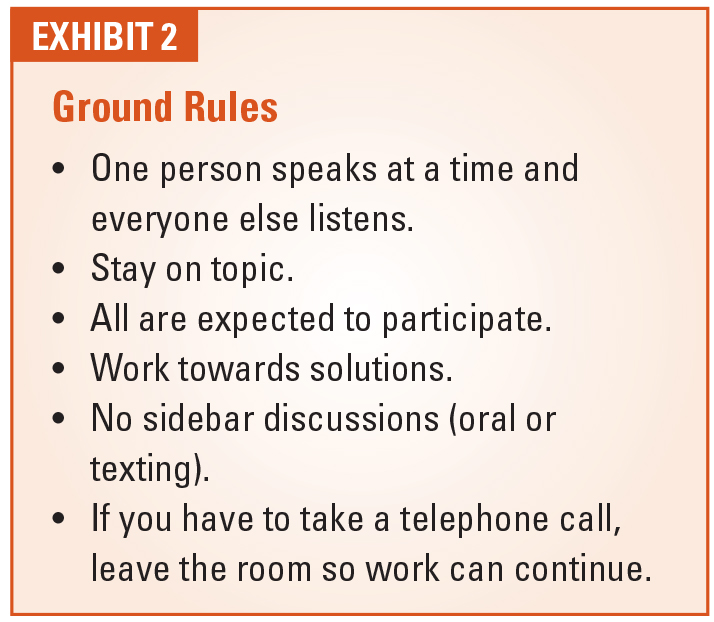
We have found the ground rules as shown in Exhibit 2 to be those that are most essential. Notice that all of these are “observable behaviors”—behaviors that can be seen rather than guessed at (how do you really tell that someone is being “open-minded”?).
Decisions
It is unlikely that all members of the group will agree on all issues. So, what do you do when all do not agree?
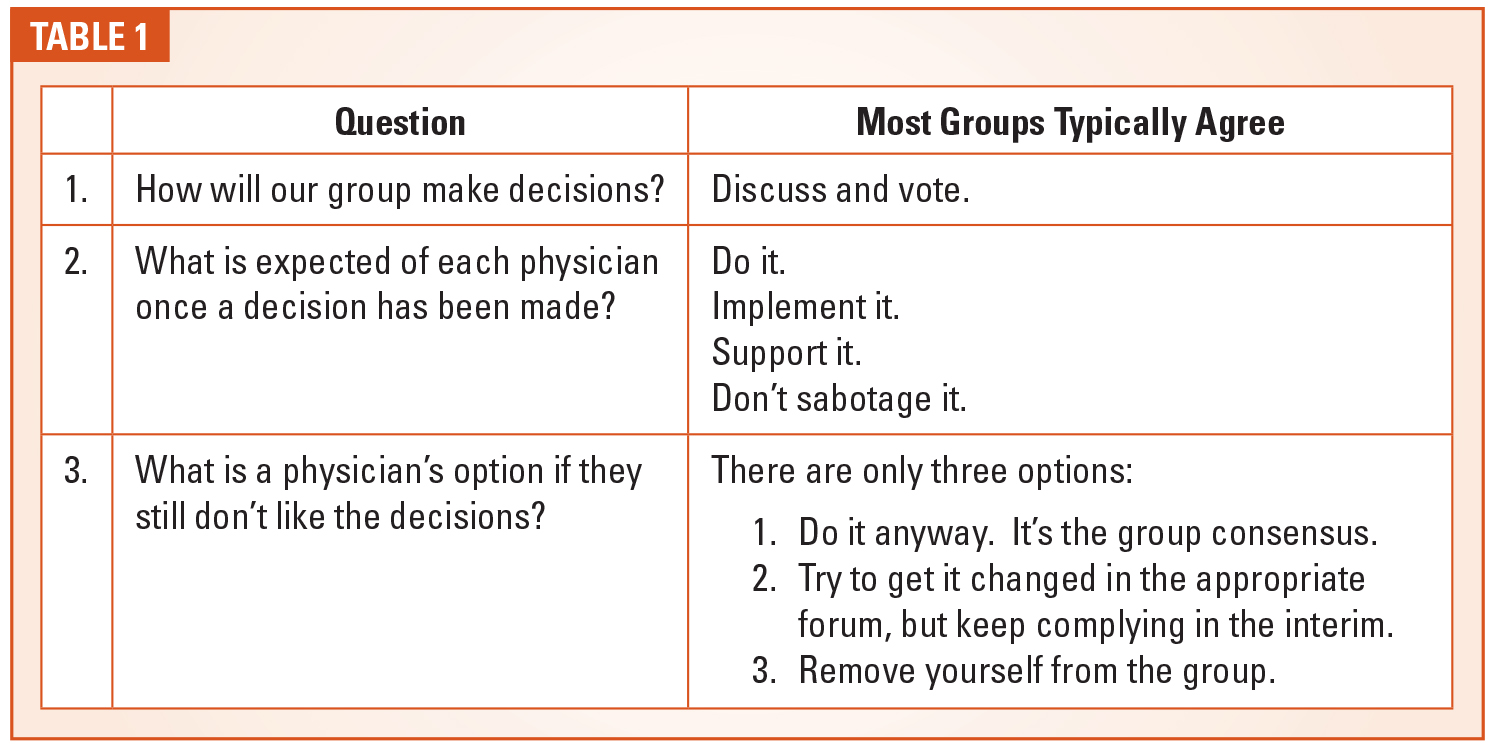
We believe that a group needs to pre-commit that all members of the group will support the decisions the group makes whether they agree with the decision or not. To do so, the group should ask and answer the following three questions as shown in Table 1.
(As a note, you are likely to find that 90-95 percent of the members of your group will completely agree with the thoughts in the “Most Groups Typically Agree” column. The remaining doctors may or may not agree or fulfill such commitments, but this gives the group the ability to challenge them if they don’t.)
Then, at the meeting, if consensus cannot be reached, the group should vote on the issue and move forward with the majority or super-majority position.
Large Groups
Larger anesthesiology groups (>30 – 40 shareholders) face a challenge when it comes to developing a strategic plan for their organization. There is a natural tension between shareholder involvement in the process and the ability to have the needed in-depth discussion to address key issues.
On the one hand, groups typically want to involve all the shareholders in the planning process, recognizing that the shareholders are more likely to support and adhere to the group’s plans if they have some input in the process.
However, trying to include dozens of shareholders in the detailed discussion to develop the plan is typically counterproductive. If a large group does this, one of the following typically happens:
- A smaller group of the attendees dominate the conversation (and most others “tune out”).
- Break-out groups are used to discuss specific issues. This can work well, but typically you cover less ground in these discussions and, at some point, you want to bring the whole group together to adopt the ideas of the small group.
- You choose a small number of topics with predefined motions that can be discussed and debated by the larger group in a very controlled manner.
 As an alternative, we have worked with a number of groups that have followed a different path in developing their strategic plan—a path that balances inclusion and the ability to have in-depth discussion.
As an alternative, we have worked with a number of groups that have followed a different path in developing their strategic plan—a path that balances inclusion and the ability to have in-depth discussion.
In order to develop a physicianendorsed and useful strategic plan for a group of the size and diversity of most large groups, the planning effort includes a process to obtain feedback from all shareholder physicians (either through interviews or surveys). This is followed by a “planning retreat process” where the group leadership (the Board and selected others—20 or less individuals) will meet to discuss key issues, develop/update a group mission/vision, and develop overall objectives and goals for the group for the planning horizon. Finally, a full group meeting will be held where the plans will be reviewed and explained, and where the shareholders will be able to provide additional input to the plan.
A Final Word
Running the gauntlet of challenges and opportunities that can be found in today’s anesthesia business environment requires strategic vision and successful planning. Anesthesia groups must take deliberate steps to ensure the planning process is sufficiently inclusive and ultimately effective. The principles and recommendations outlined above may prove helpful in the achievement of these goals.
 For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at WLatham@LathamConsulting.com.
For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at WLatham@LathamConsulting.com.