Spring 2019
Assessing Ambulatory Anesthesia Opppportunities: Robust Due Diligence Required
Jody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services Anesthesia Business Consultants, LLC, Jackson, MI
It is the rare anesthesia practice that covers only one hospital these days. Most anesthesia practices cover at least one ambulatory facility in addition to their primary hospital, and many practices actively pursue every outpatient opportunity within their service area. Usually, this serves the practice’s strategic and financial objectives—but not always.
 Conventional wisdom holds that the payer mix is generally more favorable in ambulatory venues. It can also be the case that clinical days are both shorter and more profitable. At least this is the hope. The problem is that hope and reality are often quite different.
Conventional wisdom holds that the payer mix is generally more favorable in ambulatory venues. It can also be the case that clinical days are both shorter and more profitable. At least this is the hope. The problem is that hope and reality are often quite different.
Each anesthesia practice is a unique and distinctive entity. As shown by the examples in this article, each anesthesia ambulatory arrangement is unique as well. This reality underscores the significance of determining each ambulatory agreement’s true potential upfront rather than downstream, when it has created a drag on the practice. One could say that a practice expansion is a lot like an anesthetic: the most critical phase is the preparation.
Let us consider three distinct types of ambulatory or outpatient facilities. The first and most common is the ambulatory surgery center (ASC). These may be associated with a hospital or independently owned by surgeons. The common feature of such facilities is accessibility. The intent is to provide a convenient venue with ample parking and easy access that offers as efficient a surgical experience as possible.
The next type is the endoscopy center. This may be part of an ASC or it may be a freestanding facility. Endoscopists thrive in an environment with high patient turnover. The more cases they can perform per day, the better. Endoscopic procedures tend to be short, and the majority of patients are covered by Medicare.
Because Medicare policy has changed over the past four years, Medicare patients now have a fairly compelling incentive to receive regular screenings. If the case is booked as a screening colonoscopy, the patient has no deductible or copayment. This positive development notwithstanding, recent changes to the anesthesia codes have resulted in a decline in revenue potential for these cases.
The third category is somewhat of a catchall that includes doctors and dental offices in which the anesthesia provider works in partnership with one or more physicians. Such venues may or may not have all the necessary equipment to provide general anesthesia.
Driving Factors
From a practice management perspective, ambulatory opportunities can be significant in several ways, although the specific benefit to a given practice must be carefully evaluated on a facility-by-facility basis.
As cases migrate from traditional inpatient venues to outpatient venues, there is value in being able to maintain the income from these cases. Since no after-hours call is required with ambulatory venues, the inclusion of such facilities may lessen the anesthesia providers’ call burden.
 Venues may provide an opportunity for different staffing models. A physician-only practice may consider a medical direction model in the ASC. Sometimes the potential advantage is purely strategic; covering all the ambulatory venues in a particular market may keep out potential competitors who might be seeking to displace the practice. And sometimes it is a matter of survival. Many anesthesia practices that lost their hospital contracts only exist today because they expanded into the ambulatory market.
Venues may provide an opportunity for different staffing models. A physician-only practice may consider a medical direction model in the ASC. Sometimes the potential advantage is purely strategic; covering all the ambulatory venues in a particular market may keep out potential competitors who might be seeking to displace the practice. And sometimes it is a matter of survival. Many anesthesia practices that lost their hospital contracts only exist today because they expanded into the ambulatory market.
Any practice that wants to expand its coverage should first consider its goals and objectives. What is the intent? Taking on a new line of business always involves a certain degree of risk. We all know that any deal that seems too good to be true usually is.
If the primary goal is financial, then there must be a solid basis for believing that the revenue potential will be greater than the cost of providing the service. However, this can be a very tricky calculation, especially if the proposed agreement is with a new facility where neither volume potential nor payer mix can be definitively determined. And if the objective is strategic, how much risk is the practice willing to bear, and for how long?
Some exclusive service agreements with hospitals may preclude expansion into what could be viewed as competitive venues, i.e., those that would be drawing cases away from the hospital. Any consideration of expansion must begin with clarification of existing commitments. The good news is that, increasingly, hospital administrators have come to understand that the practice that has other contracts may not need as much financial support as those that don’t.
Essential Information
Often, the evaluation of such opportunities involves more due and less diligence. Three types of information are essential.
First, the anesthesia revenue potential must be projected. This involves a determination of case volume and payer mix. Any assumptions used to determine these should be conservative. The biggest challenge is the ramp-up scenario, especially absent a financial guarantee for coverage as surgical volume builds.
Second, what are the coverage requirements and how consistently will cases be booked? Either case schedules are short and unpredictable, in which case, providers may cover them on a post-call day, or the schedule will be consistently full and require a dedicated team.
Finally, what will be the cost of coverage? This is the most critical piece of the business plan. You should know the per-day cost of all possible staffing options. Will a physician partner be the provider or a non-partner physician? Do you have the medical direction model? If so, what level of direction will be used?
Knowing your per diem cost is an essential prerequisite for any assessment of coverage requirements. For each category of provider, the per diem cost can be determined by dividing the total cost of a provider (base pay, bonuses, overtime, benefits and the cost of overhead) by the number of days the provider works per year.
Key Metrics
The best way to begin an evaluation of a new coverage opportunity is to establish benchmark references based on the existing practice. Most practices have a good idea of actual collections by facility or line of business. Basic production metrics are typically available from standard billing reports. They also know how each venue is staffed.
 What most do not have, however, are the critical normalized metrics, such as yields and costs per provider day. As a practical matter, the best data only includes activity for cases performed Monday through Friday between the hours of 7 am and 3 pm, a typical day shift. Why only weekdays from 7 am to 3 pm? This timeframe reflects typical ambulatory utilization.
What most do not have, however, are the critical normalized metrics, such as yields and costs per provider day. As a practical matter, the best data only includes activity for cases performed Monday through Friday between the hours of 7 am and 3 pm, a typical day shift. Why only weekdays from 7 am to 3 pm? This timeframe reflects typical ambulatory utilization.
Why is it so important to know the baseline metrics? Without them you have no point of comparison and no way to assess the impact of a new venue on the practice’s overall profitability. Many anesthesia practices assume that the addition of ambulatory contracts will enhance the practice’s profitability, but often this is not the case. We have seen numerous practices become spread too thin by unprofitable ambulatory commitments that limited what they could pay the partners. A couple of practices found themselves without enough revenue to recruit and retain needed providers.
Assess Impact

A simple and useful way to assess the impact of expansion is to calculate and track the overall practice net yield per ASA unit billed. As an alternative, some practices prefer to track the overall yield per hour of anesthesia time. Table 1 provides an example of such a calculation for a practice that already covers a variety of facilities. Note that for purposes of these calculations obstetric cases are excluded. This is also an example of a practice where the inclusion of six ambulatory facilities enhances the key metrics: the yield per unit billed and the yield per hour of billed anesthesia time.
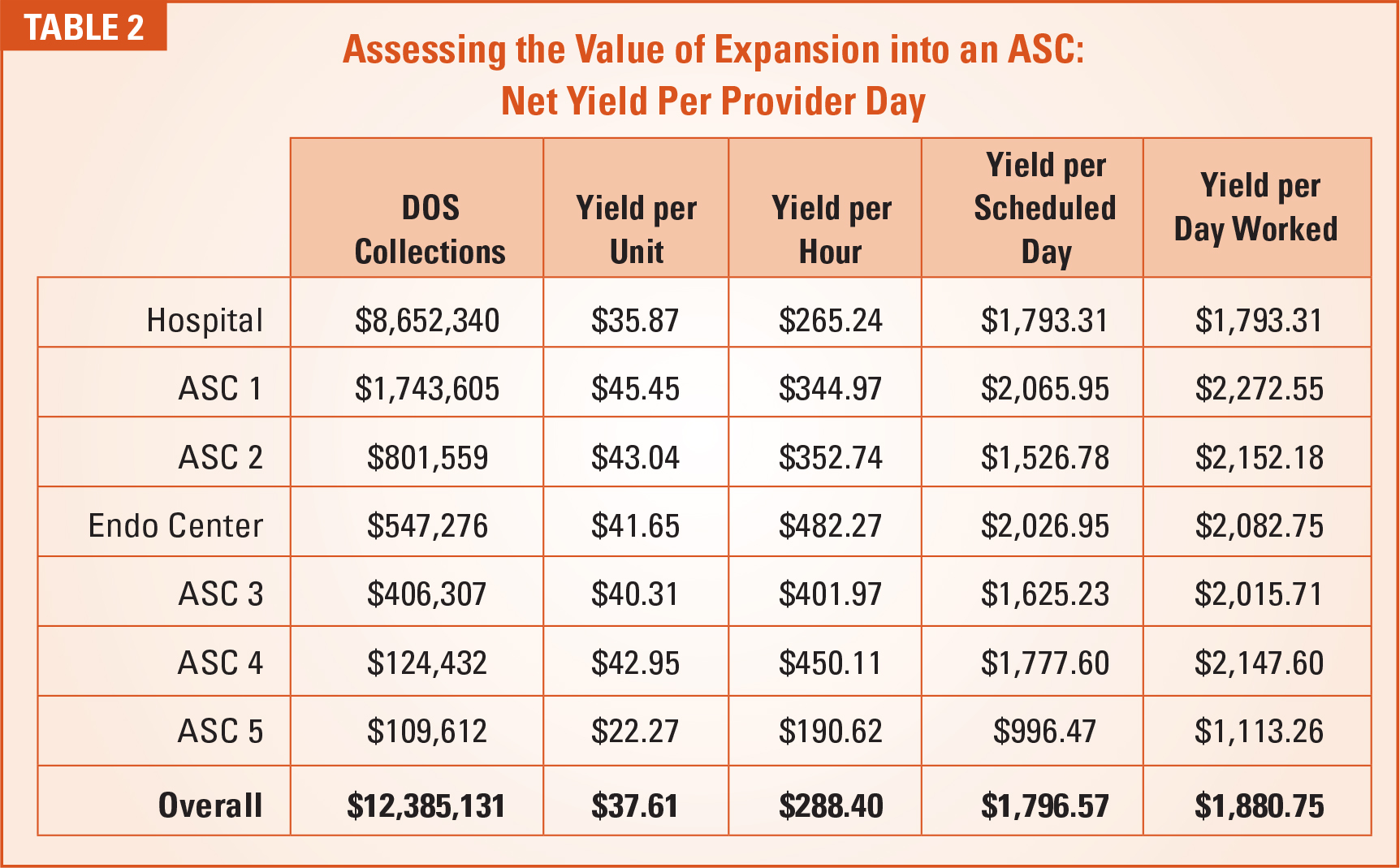
Table 2 shows an additional metric: yield per provider day. There are two ways to calculate this metric: based on scheduled days or based on actual days worked. Ideally, every practice should be able to calculate these metrics based on weekday shifts from 7 am to 3 pm.
It is important to remember that no two ambulatory facilities are managed the same. The key variables are the volume of activity, the payer mix and the consistency of scheduling.
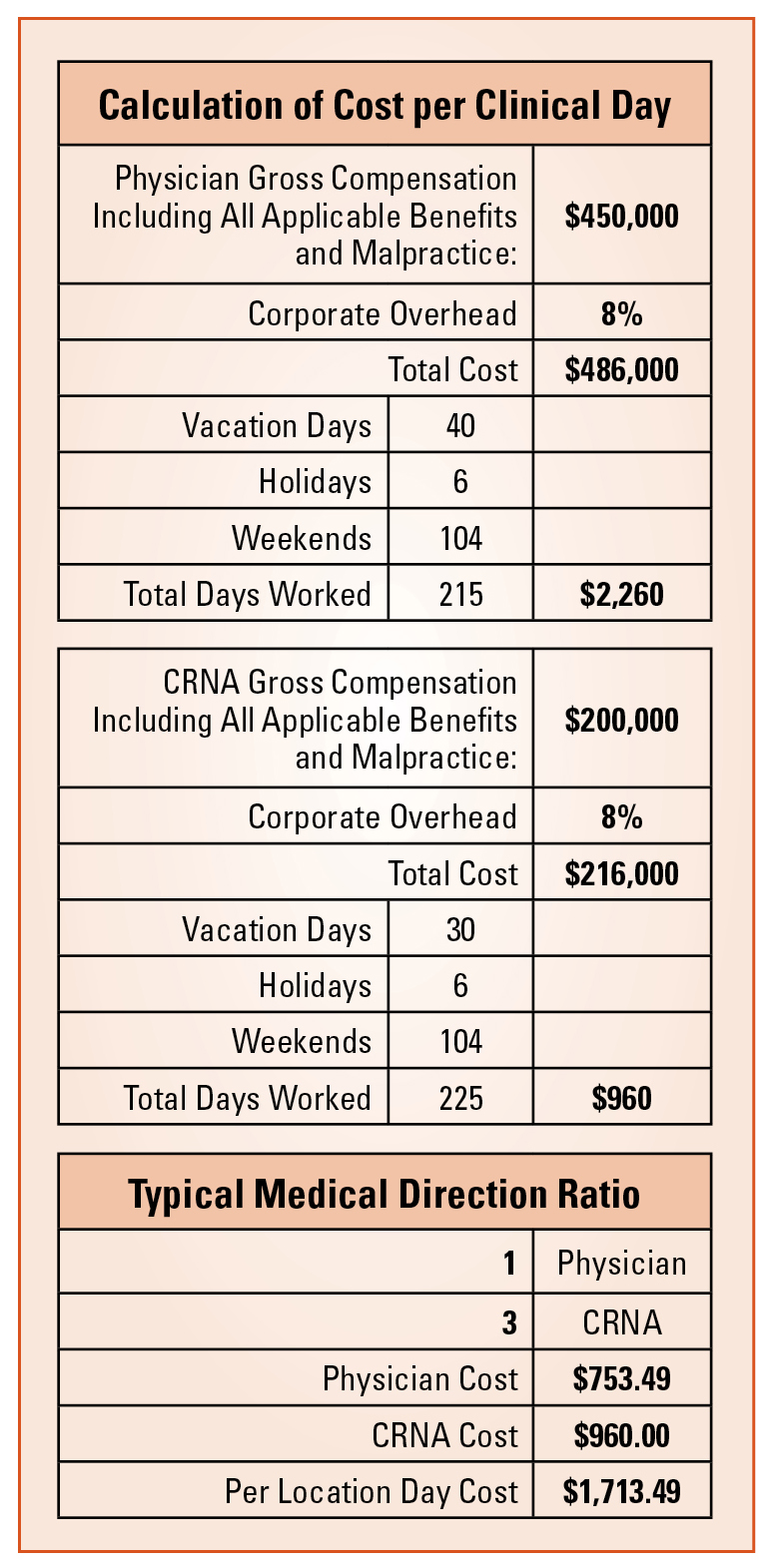
Calculating the cost per anesthetizing location day is not complicated, but some critical variables must be carefully determined. Provider compensation must include all related costs, such as benefits, pension commitments, malpractice and overhead. This is what accountants refer to as a burdened cost. It is also necessary to calculate how many days a typical provider works per year, which may be tricky if vacation policy is flexible. As a result, it may not always be possible to exactly determine provider days per year.
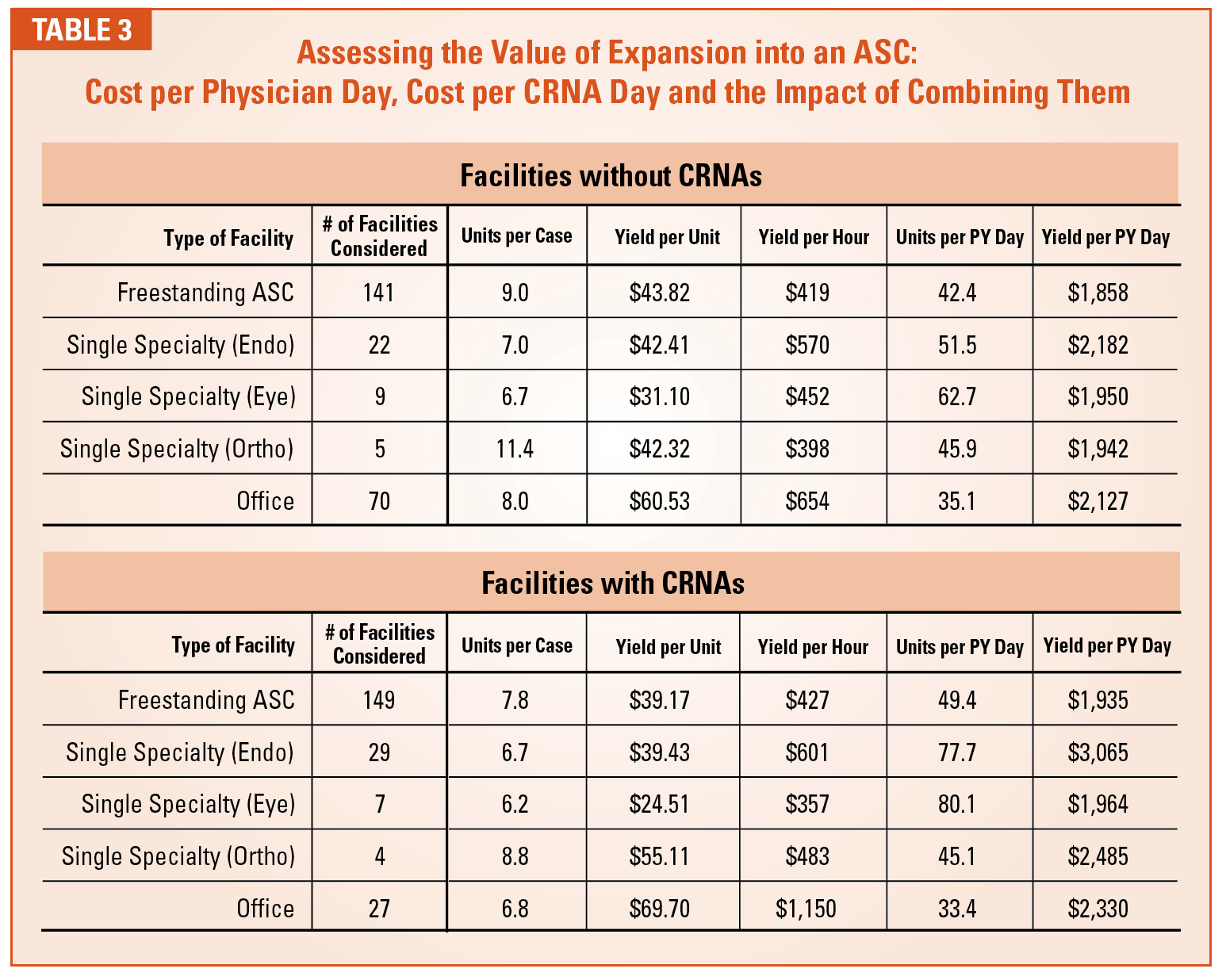
Table 3 provides three critical metrics to determine potential profitability: cost per physician day, cost per CRNA day and the impact of combining them. In the example given, one physician medically directs three CRNAs. Usually there is no cost savings if the ratio of physicians to CRNAs is less than 3:1.
Clear Plans Needed
The benchmark data and calculations provided thus far will allow a practice to establish the basic calculation of profit potential. The next step is to validate the numbers and assess the potential risk factors.
Usually the biggest challenge comes from the production and payer mix data provided by the facility, especially if it is just opening. Projected volumes and payer mix for a new facility can be notoriously unreliable. New facilities pose the biggest problem. What is the ramp-up going to look like and who will bear the cost? Cash flow always lags behind production by three or four months.
Since providers must be paid from the beginning, the question is: who will bear the expense of providing the service until the collections materialize? A large group may have the financial resources to cover the float, but doing so carries considerable risk. One would hope that the facility could provide some start-up support, but this rarely happens.
The best approach is to develop a clear business plan for each new contractual agreement. Many of these agreements are based on a handshake and a friendly agreement between the parties, but this is never advisable. There should be budget projections for both collections and cost. If the collections do not increase as projected, the practice should have the right to cancel the contract.
Should any of these considerations discourage today’s anesthesia practices from exploring opportunities for expansion? Absolutely not. Few practices will survive as stand-alone hospital-based practices. The greater the need to expand, however, the greater the caution required. The goal must be to pick the horse that will go the course. Due diligence must be rigorous and consistent. The risks of expansion are significant, but so are the potential rewards if the process is handled effectively.
Please note: ABC does not endorse any of the strategies described in this article, and any patient seen at any type of facility should first and foremost receive medically necessary services and have decisions made that promote the health and wellbeing of the patient.
 Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.
Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.