The Significance of the Anesthesia Public Payer Percentage
Summary
The growing senior population and the number of patients covered by Medicaid and other public payors is creating an inexorable challenge to anesthesia practice budgets. The long-term implications of the impact of low public payment rates is only going to create more problems in the negotiation of hospital subsidies. It is also unclear how this drop in revenue potential may interface with new surprise billing laws.
Baby boomers are the fastest growing age group in the United States. Currently, 14.5 percent of the nation's population is 65 years old or greater. By year 2029, the national population of this same age group will be 20 percent. How is this affecting anesthesia practices today and what are the long-term implications? Demographic trends have the potential to dramatically change the economics of this specialty.
Those of us in the billing and practice management arena often refer to the concept of payer mix when evaluating the revenue potential of a practice. The term typically evokes the image of a pie chart, representing the various payer wedges of the practice. The Medicare and Medicaid slices represent the lowest payment rates and therefore, their respective sizes indicate the extent to which the practice is captive to state and federal payer rates. As this Public Payer Percentage (PPP) increases beyond 30 or 40 percent, it is inevitably an indicator of the need for financial support from the facility. The reality is that the traditional pie chart does not do justice to a payer mix, which is evolving and dynamic.
As the American population ages, more patients are covered by Medicare, although the rate of growth of the Medicare surgical population will inevitably lag behind the overall percentage in the community. The reason is that most of the conditions that afflict the elderly are medical conditions and not surgical conditions. Still, the number of Medicare patients undergoing surgical procedures continues to grow. In fact, this growth has been enhanced somewhat by recent changes in endoscopy policies, with GI becoming a significant and expanding line of business for most anesthesia practices. Although patients over 50 should get regular screenings, the bulk of these patients are over 60.
A different set of factors determine the Medicaid population, since eligibility is not based on a patient's age, but rather financial status. Location is often the most significant factor associated with inner-city hospitals. Under the Affordable Care Act (ACA), a number of states opted to expand their Medicaid programs. These programs do not typically increase as rapidly as Medicare programs, but they rarely decrease.
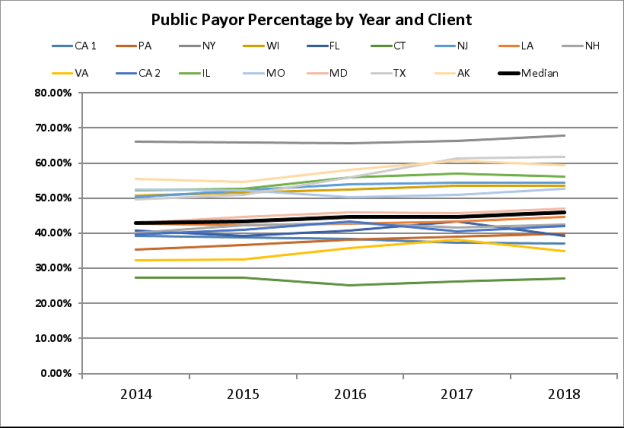
The chart below is based on a sample of 16 large ABC clients from across the country, representing practices in 15 states. While three of these clients have actually seen a slight decrease in their PPP, the average increase in this metric over the past five years has been 42.8 percent to 45.8 percent. Such trends tend to be predictive; as the population continues to age, we expect the percentage of Medicare patients to increase. Unless there is a major change in U.S. healthcare policy, we can also expect the percentage of patients who are uninsured or covered by Medicaid to continue to rise, although this is likely to be more pronounced in urban practices.

Consider the rates associated with each payor type in your practice. Let's assume that your average PPO plan rate is $60 per ASA unit. This is almost three times the average Medicare rate and four times the average Medicaid rate if the typical anesthesiologist were to generate 10,000 billable ASA units per year and neither the average PPP rate of $21.25, nor the average PPO rate of $55 had changed, then he or she would have seen an increase in the PPP of three percent and a corresponding loss in PPO and other commercial units. The overall financial impact would have been a loss in total collections of about $10,000 per provider, over five years. This might not seem like a lot and, in many cases, the impact could have been minimized by better commercial payment rates. However, the reality is that it is becoming harder and harder to negotiate with payors, thus making it increasingly difficult to offset the impact of the PPP. As a result, the PPP will ultimately come to represent ongoing erosion in the revenue potential of the practice.
Two additional factors may also play a role in evaluating the impact of the PPP. The first is the migration of cases from inpatient to outpatient venues. Conventional wisdom holds that the payer mix is more favorable in ASCs since there are fewer Medicare and Medicaid patients, but our review revealed that such is not always the case. One of the reasons is the impact of endoscopy, which may involve a higher percentage of Medicare patients.
We often say that if you have seen one anesthesia practice, then you have seen one anesthesia practice. Every situation is unique. While the impact of these basic demographic trends may not seem to be significant and severe, no practice should ignore them. It is a dynamic that must be taken into consideration when reevaluating hospital contracts. Many consultants will say that it is relatively easy to calculate the amount of a subsidy required today, but will it be right tomorrow? The projected impact of your PPP over time must be an important variable in the equation.
If you want a more detailed assessment of these demographic trends and their financial impact to your practice, please contact your ABC client service manager who will be happy to perform the necessary evaluation for you.