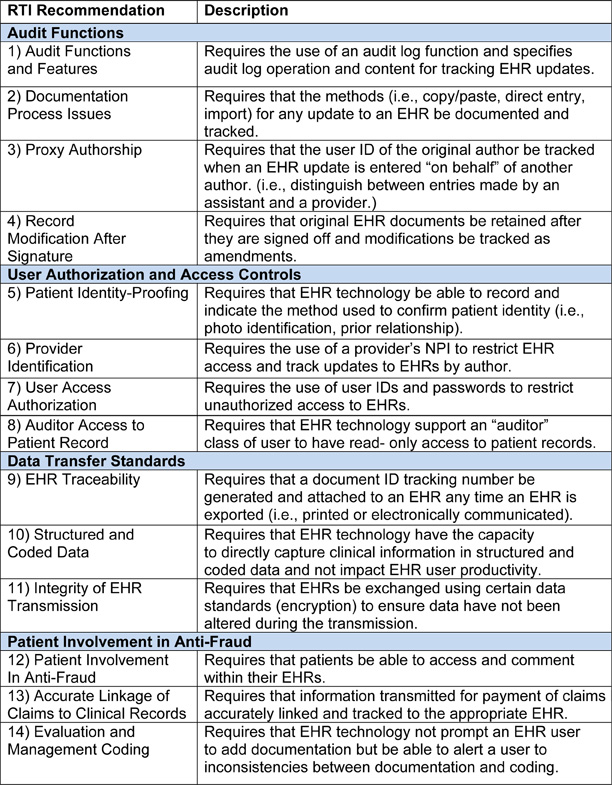
 Electronic health records (EHRs) make it easier to document patient care with incorrect information, not just with desirable data. To put it bluntly, as does the Health and Human Services Office of the Inspector General (OIG) in its just-released report Not All Recommended Fraud Safeguards Have Been Implemented in Hospital EHR Technology, “Experts in health information technology caution that EHR technology can make it easier to commit fraud.”
The technology can also facilitate unintentional errors, particularly if the provider is not certain whether he or she is reporting a case in perfect compliance with Medicare requirements. Consider the copy-and-paste feature of many software applications (including Windows). This feature allows providers and other users to retrieve information from one place or one record and place it in another through a few mouse-clicks. If a pain physician knows that a carrier will only deem repeat facet joint injections medically necessary “when the patient...
Electronic health records (EHRs) make it easier to document patient care with incorrect information, not just with desirable data. To put it bluntly, as does the Health and Human Services Office of the Inspector General (OIG) in its just-released report Not All Recommended Fraud Safeguards Have Been Implemented in Hospital EHR Technology, “Experts in health information technology caution that EHR technology can make it easier to commit fraud.”
The technology can also facilitate unintentional errors, particularly if the provider is not certain whether he or she is reporting a case in perfect compliance with Medicare requirements. Consider the copy-and-paste feature of many software applications (including Windows). This feature allows providers and other users to retrieve information from one place or one record and place it in another through a few mouse-clicks. If a pain physician knows that a carrier will only deem repeat facet joint injections medically necessary “when the patient...  As we head into the final quarter of the year, the departmental and group stability that anesthesiologists seek remain elusive. Hospitals and health systems continue their drive toward consolidation. National management companies report more and more acquisitions of anesthesia practices. The Affordable Care Act’s Health Insurance Exchanges will have begun to enroll beneficiaries by the time this issue of the Communique is in your hands, with much of the uncertainty over the functioning unresolved. Indeed, after forty attempts by the House of Representatives to repeal the Affordable Care Act, much of the law will be in effect by January 1, 2014, unless there is a successful forty-first or forty-second attempt, which strikes us as unlikely. Defunding may yet kill the ACA, but for now we must proceed on the assumption that the law will be very much with us next year.
The new environment demands accountability as well as “value” and...
As we head into the final quarter of the year, the departmental and group stability that anesthesiologists seek remain elusive. Hospitals and health systems continue their drive toward consolidation. National management companies report more and more acquisitions of anesthesia practices. The Affordable Care Act’s Health Insurance Exchanges will have begun to enroll beneficiaries by the time this issue of the Communique is in your hands, with much of the uncertainty over the functioning unresolved. Indeed, after forty attempts by the House of Representatives to repeal the Affordable Care Act, much of the law will be in effect by January 1, 2014, unless there is a successful forty-first or forty-second attempt, which strikes us as unlikely. Defunding may yet kill the ACA, but for now we must proceed on the assumption that the law will be very much with us next year.
The new environment demands accountability as well as “value” and...  The Centers for Medicare and Medicaid Services (CMS) released the 1369-page final regulations containing the changes to the Physician Fee Schedule for 2014 (the “Final Rule”) on the Wednesday before Thanksgiving. Updates and provisions of interest to anesthesiologists include the 2014 conversion factor and changes to the Physician Quality Reporting System (PQRS) and Value-Based Payment Modifier requirements.
Conversion Factor
The national average anesthesia conversion factor (CF) is set at $17.2283 for 2014, down from $21.9243 this year. This includes a one-percent increase in the Medicare Economic Index for anesthesia services; many other specialties saw no increase or a negative impact.
The general Medicare conversion factor, which applies to pain medicine, critical care, evaluation and management and other “flat fee” services, will decrease by 20.1 percent, to $27.2006. In March 2013, CMS had projected a CF decrease of 24.4 percent for 2014.
The announcement of a decrease should not raise an alarm: ...
The Centers for Medicare and Medicaid Services (CMS) released the 1369-page final regulations containing the changes to the Physician Fee Schedule for 2014 (the “Final Rule”) on the Wednesday before Thanksgiving. Updates and provisions of interest to anesthesiologists include the 2014 conversion factor and changes to the Physician Quality Reporting System (PQRS) and Value-Based Payment Modifier requirements.
Conversion Factor
The national average anesthesia conversion factor (CF) is set at $17.2283 for 2014, down from $21.9243 this year. This includes a one-percent increase in the Medicare Economic Index for anesthesia services; many other specialties saw no increase or a negative impact.
The general Medicare conversion factor, which applies to pain medicine, critical care, evaluation and management and other “flat fee” services, will decrease by 20.1 percent, to $27.2006. In March 2013, CMS had projected a CF decrease of 24.4 percent for 2014.
The announcement of a decrease should not raise an alarm: ...  Many anesthesia practices across the country are hybrid entities, consisting of a subgroup of anesthesiologists and CRNAs who provide only surgical and obstetric anesthesia and another subset who spend part or all of their time in the management of chronic pain. The circumstances that have encouraged the development of such entities vary considerably, but it is a common phenomenon across the country in all types of settings.
In some cases, the different sets of providers appear to work quite harmoniously but these are the exceptions rather than the rule. Most struggle with a consistent set of challenges that derive directly from the fundamental differences between the two types of practices. Even a cursory review of any of these practices reveals just how different the criteria are for success in chronic pain as compared to O.R. or obstetric anesthesia. Simply put, the demands of a hospital-based anesthesia practice bear little or no...
Many anesthesia practices across the country are hybrid entities, consisting of a subgroup of anesthesiologists and CRNAs who provide only surgical and obstetric anesthesia and another subset who spend part or all of their time in the management of chronic pain. The circumstances that have encouraged the development of such entities vary considerably, but it is a common phenomenon across the country in all types of settings.
In some cases, the different sets of providers appear to work quite harmoniously but these are the exceptions rather than the rule. Most struggle with a consistent set of challenges that derive directly from the fundamental differences between the two types of practices. Even a cursory review of any of these practices reveals just how different the criteria are for success in chronic pain as compared to O.R. or obstetric anesthesia. Simply put, the demands of a hospital-based anesthesia practice bear little or no...
BREAKING NEWS: CMS released the final 2014 Physician Fee Schedule rule on Wednesday, November 27. The Medicare conversion factor will be reduced by 20.1 percent, not 24.4 percent as projected last March—unless Congress intervenes, as most observers expect will happen. Please see next week’s Alert for more information.
December 2, 2013
One of the longest-running Medicare whistleblower lawsuits, U.S. ex rel. El-Amin v. George Washington University (D.D.C. November 25, 2013), has apparently come to an end, without a trial. Late last month, the United States District Court granted the defendant’s motion for summary judgment, which means that even if the plaintiff’s factual allegations were true, the defendant would prevail as a matter of law.
Four nurse anesthetists then employed by the George Washington University (GWU) brought a qui tam or whistleblower lawsuit against GWU in 1995. They alleged that between 1989 and 1995, GWU had submitted thousands of claims to Medicare...