Anesthesia Industry eAlerts
Sent to subscribers every Monday morning, our eAlerts deliver timely updates on regulatory, legislative and practice management developments of interest to anesthesia professionals.
Complete the simple form below to subscribe.
Monitored Anesthesia Care: The Rest of the Story
Change begets more change, and so it is with the introduction and evolution of monitored anesthesia care. Today’s article provides a sweeping view of MAC’s history, as well as future implications for the anesthesia technique.
July 3, 2023
While anesthesia providers may employ a wide variety of techniques to induce anesthesia from a coding and billing perspective, every case must be reported as only one of three modes of anesthesia: general anesthesia (GA), monitored anesthesia care (MAC) and regional anesthesia. The predominant mode for surgical cases is GA, and regional is the typical mode for obstetrics. It is MAC that seems to cause some confusion. Given the history of the term and the evolution of the specialty, this confusion is clearly understandable. The purpose of the following discussion is to put the reporting of anesthesia technique into perspective.
The Origin of MAC
The term “monitored anesthesia care” (MAC) was introduced in 1986 to improve on the term “anesthesia standby” used up until then, with the term “standby” being hard to defend when payment was requested. It was a result of a conference that included members of the American Society of Anesthesiologists (ASA) and representatives of the Healthcare Finance Administration (HCFA). The objective was to create a term that defined a clinical situation in which a patient’s medical status required the presence of an anesthesia provider to monitor the patient’s health through the surgical procedure but where the level of sedation did not render the patient unconscious or unable to respond purposefully to stimulus.
Upon adoption of the term, HCFA decided that all Medicare claims for patients undergoing a MAC anesthetic should be flagged with a QS modifier. This did not affect the rate of payment. All modes of anesthesia are paid at the same rate. The reason for the modifier was based on the perspective that MAC cases did not necessarily require an anesthesia professional, i.e., it might not be medically necessary to pay for this service. Based on this interpretation, a number of Medicare intermediaries determined that a second diagnosis for the case would be required in order to better justify the need for anesthesia.
At the time the term (MAC) was coined, it was actually intended to define the level of care provided to patients undergoing eye surgery. The anesthesia code most commonly used for these cases was 00142: Anesthesia for procedures of the eye, involving lens surgery. That code was valued at four base units in the calculation of Medicare payments. Most anesthesia providers considered the addition of MAC as a positive development that would ensure their payment for eye surgery on Medicare patients.
The Endoscopy Challenge
In the 1980s, most colonoscopies did not involve the need for anesthesia providers; but, over the next decade, this would change. At first, there was a public health issue. The goal was to encourage Medicare patients to get regular screenings for polyps and colon cancer. Eventually, the federal government addressed this concern with a new policy. Patients who scheduled a screening colonoscopy were entitled to anesthesia. If the colon turned out to be normal, they would incur no responsibility for their deductible or their co-insurance (20 percent of the allowable) for the anesthetic. This policy change encouraged many anesthesia practices to expand their involvement with endoscopists.
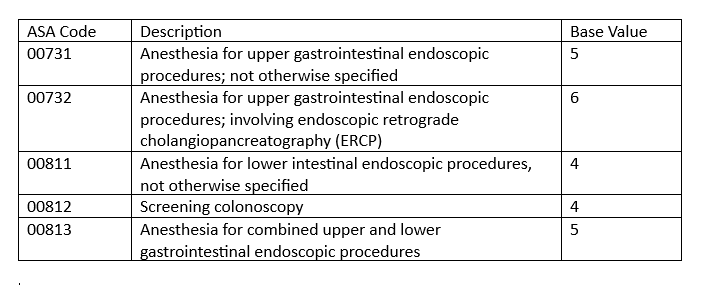
American medicine is never immune to the law of supply and demand. As the supply of a service increases, its demand decreases, and the price drops. This principle had a most curious impact on anesthesia. Initially, there were two codes for endoscopy, 00740 and 00810, both of which were worth five base units. As the volume of claims for anesthesia for endoscopic procedures continued to increase, the coding for anesthesia changed. Two anesthesia codes begat five. As indicated below, two were for upper GI procedures, two were for lower GI and one was for upper and lower. The net effect was that the base units for lower GI procedures dropped to four. In fact, Medicare went one step further and dropped the value of lower GI procedures with a normal colon to three units.
MAC Versus GA
Meanwhile, the ASA has clarified the definition of GA. If the patient loses consciousness or the ability to respond purposefully to adverse stimuli for any portion of the case, the anesthetic should be reported as GA. As a practical matter, endoscopic cases utilizing propofol will typically involve the patient losing consciousness at some point. Based on current ASA policy, we therefore recommend that all endoscopies involving a patient’s loss of consciousness be reported as GA.
Despite the fact that we articulate this recommendation quite clearly in all of our in-service presentations, many providers continue to default to the historical practice of reporting endoscopies as MAC cases. The reality is that given most payer policies the use of MAC for these cases will not jeopardize payment. The logic of our argument is that the use of MAC for these cases tends to undermine the value of the service provided, which is never in the long-term interest of the specialty.
One thing that complicates the determination of MAC versus GA is the facility. Especially, in the mid-Atlantic region there are outpatient facilities that are not licensed for general anesthesia. When care is provided in such settings then MAC would be required.
The Future of Payment for Endoscopy
For most anesthesia practices, endoscopy has been the fastest growing and most profitable line of business. It is not uncommon for anesthesia groups to obtain 30 percent of their revenue from endoscopy. There is no question that the use of professional anesthesia services has increased the safety and comfort of patients in such cases. It has also increased, no doubt, the productivity of endoscopists. The problem is some insurers are now starting to push back on the dramatic increase in anesthesia claims for colonoscopy procedures. We are starting to see evidence of this pushback in various parts of the country. Harvard Pilgrim, a major insurance plan in Massachusetts refuses to pay for anesthesia for colonoscopies for patients with an ASA I physical status. Other plans may follow suit—more examples of the law of supply and demand at work.
We have been in this business for decades and have seen many changes. When there is a new policy announcement or when we discover a new problem, we must not get so focused on that particular issue that we lose sight of the larger context. At one point, we were very focused on the distinction between general and MAC anesthesia and its implications for the claims we were submitted. Eventually, though, we came to realize that was just the first step in a protracted process that has more to do with the value of services provided than the payment. The reporting of endoscopic services has gotten considerably more complex over the past few decades. And what does that mean? As we get more excited about the potential, the payers are contemplating how to thwart our advance.
If you have any questions on this topic, please reach out to your account executive.
With best wishes,
Rita Astani
President—Anesthesia