Anesthesia Industry eAlerts
Sent to subscribers every Monday morning, our eAlerts deliver timely updates on regulatory, legislative and practice management developments of interest to anesthesia professionals.
Complete the simple form below to subscribe.
What Anesthesia Providers Should Know about Their Surgeons
Analysis of a group’s revenue potential often overlooks the impact of the surgeons with whom the group partners. Today’s article addresses three critical factors that anesthesia practices should consider when projecting future revenue.
May 22, 2023
In the current environment, many of the managers and directors of most anesthesia practices are increasingly concerned about the revenue potential of their practices. An increasing Medicare population is just one of the potential challenges placing downward pressure on a practice’s revenue potential. Most practices must rely on the financial support of their primary facilities to generate enough income to recruit and retain an appropriate team of qualified providers. While many hospital administrators recognize the importance and value of a strong anesthesia department, even their resources are not unlimited. These challenges are forcing most practices to perform a deeper dive into the factors that determine their income and lifestyle.
While it is always important to know what has been collected and how much money there is in the bank, given the dynamic nature of accounts receivable, it is increasingly imperative that financial management be more prospective and proactive. This means they must be vigilant in identifying opportunities and aggressive in assessing negative trends and potential threats. To this end we have long since been encouraging our clients to distinguish the services they provide in three categories: time-based surgical cases; obstetric cases and non-time-based flat fee services. Increasingly, we are now encouraging our clients to take a closer look at their surgeons, because after all, they are the ones who generate most of the revenue for both the facility and the anesthesia practice. In fact, it is usually the quirks and idiosyncrasies of the various surgical practices that most impact the economics of the specialty.
The Three Metrics
From our perspective, there are three things that the anesthesia providers should know about each of their surgeons. First of all, it is very important to identify the busiest surgeons and how likely they are to stay loyal to the facility. Is their allegiance something that the anesthesia practice can count on? Beyond this, though, it is significant to determine how busy they are. Are their clinical days full and generating a reasonable number of billable ASA units? Ultimately, the practice must also know the impact of payer mix and the extent to which they are generating an average yield per day that can cover the cost or providing the care.
It is only with these three critical metrics in hand that the anesthesia department can have an effective dialogue with administration about the future of the practice.
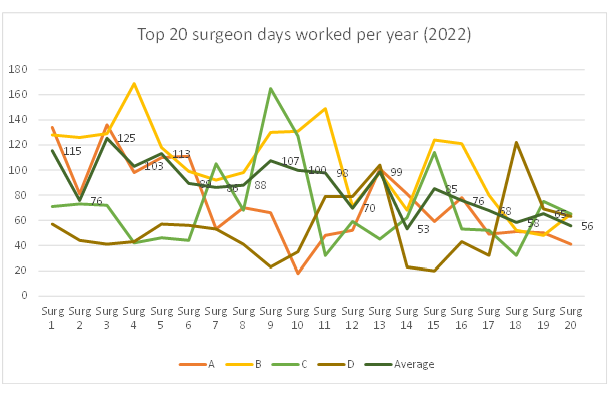
Activity Level
No two surgical practices are the same. The chart below shows monthly case volumes for the top 20 surgical practices from five client practices. It is not uncommon to have a few exceptionally productive surgeons, which is always a good thing. What matters, though, is the impact of the average on the revenue potential of the practice. For the five practices included in this study, 20 surgeons generate an average of 33 percent of total surgical revenue. In this sample, the average surgeon booked cases 87 days a year. Obviously, some were considerably more productive in terms of cases performed but as we will indicate below, this is only part of the story. After all, no two cases are exactly the same even though each represents a unit of work for the practice.
The following are intended to highlight data and trends that anesthesia practices may want to track.
Billable Units
What actually matters more to the anesthesia practice is the average number of billable units attributable to each surgeon per day on the schedule. Conventional wisdom holds that a good day’s work in the operating room should generate between 50 and 60 billable ASA units. While it is true that many facilities will schedule multiple surgeons into a given anesthetizing location and ideally the practice will track average ASA units per anesthetizing location per day, for purposes of this analysis we are primarily focused on the top surgeons who have been given significant block time allocations.
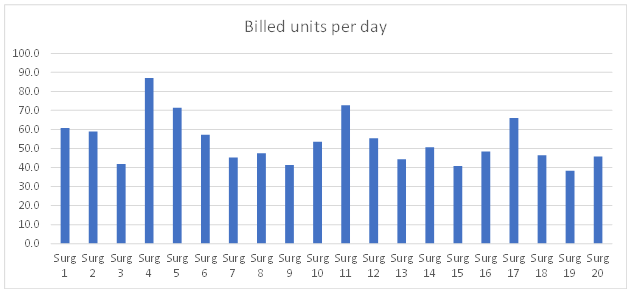
The chart above represents the calculation of normalized production metrics: total average ASA units billed per surgeon’s scheduled day. For this sample, the average surgeon generated 53 billable units per clinical day. It turns out that this is a particularly useful metric to share with administration; and the 53 units per anesthetizing location day is a very appropriate target to shoot for.
Ultimately, the actual value of each surgeon’s work is greatly impacted by the payer mix of the patients treated. The most significant elements here are the percentage of units billed to Medicare and Medicaid. The higher this public payer percentage, the less opportunity the practice has to offset the impact of the significantly discounted public payer rates.
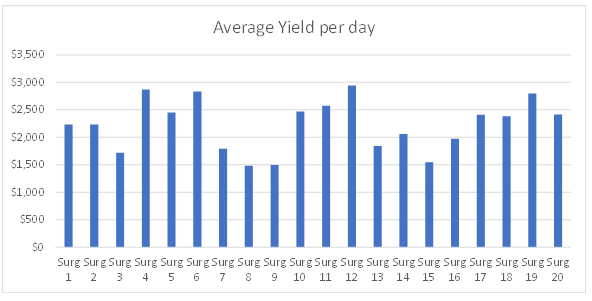
Average Daily Yield
The best way to evaluate the data below is to compare the revenue potential of each day of a surgeon’s schedule with the actual cost of providing the service. Typically, $2,200 is the cost of a physician-only practice where the physicians are paid at the MGMA median. The actual calculation of the cost of a day’s care for a care-team practice (physicians and CRNAs) can be somewhat less, but this depends on the compensation and mix of providers.
The table below is presented simply as an example of the calculations that can be prepared for a given practice. These were determined by multiplying the revenue divided by the total days.
Traditionally, anesthesia providers have not spent much time analyzing their surgeons, but things are changing, and surgeon metrics are no longer something that should be taken for granted. A detailed analysis of the anesthesia impact of surgeon behavior can be of considerable interest to administrators. If nothing else, it is a good way to demonstrate the value of the anesthesia database.
With best wishes,
Rita Astani
President—Anesthesia