eAlerts
-
The 2023 Quality Payment Program: Updates for Anesthesia
Bryan Sullivan, MSHS
Chief Quality Officer, Anesthesia Business Consultants, LLC, Jackson, MIThe Merit-based Incentive Payment Systems (MIPS) program is entering its eighth year of operation, and it is still a hotbed of confusion, anxiety and—depending on whom you ask—misinformation. This is largely because participation in MIPS is extremely dependent on the specialty, the group, the reporting option and the clinician’s commitment to continued participation. For the past several years, providers were offered an exemption to the program due to the COVID-19 pandemic, but 2023 will not likely continue to enjoy this backstop. To help dispel some of the stress with navigating MIPS, this article will walk through the requirements of 2023 reporting and be a resource to review if you have any questions about how you need to participate next year.

MIPS Category Review
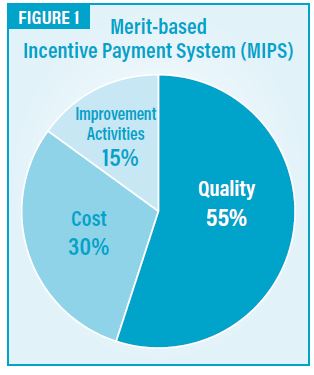
At the high level, there are only two categories that need to be considered under MIPS: Quality and Improvement Activities. These two categories comprise 70 percent of your overall MIPS composite score, as Cost is automatically calculated by CMS, based on your billing.
When added together, these three categories must total 75 points or more to avoid a penalty in 2023. For example, at the end of the year when each category score is calculated, and your results are 80 percent in Quality, 100 percent in Improvement Activities, and CMS awarded 75 percent in Cost, your total would be as follows:
If the total score is above or below the 75-point threshold, bonuses or penalties will be assessed on a linear sliding scale. If this looks a little daunting, you may be excluded from the entire program if you bill less than $90,000 in traditional Medicare allowed per provider. If you are curious about your status, click here (https://qpp.cms.gov/participation-lookup) for the MIPS participation lookup tool.
Now that we have a general understanding of MIPS at a high level for next year, let’s look at some details.
Category Details
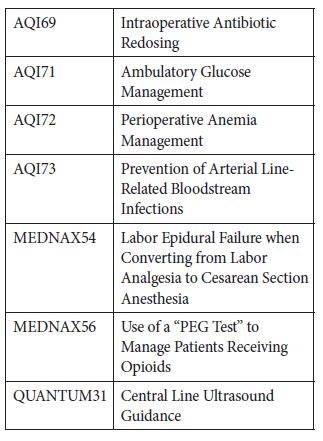
Thankfully, little has changed within each category for 2023. For example, the data completeness requirement remains at 70 percent for Quality category reporting, meaning clinicians will need to report on 70 percent of each measure’s eligible population to be counted. The big news is that a widely reported Quality measure will be retired. MIPS 76 (Prevention of Central Venous Catheter - Related Bloodstream Infections) is no longer an eligible measure because most clinicians were compliant and therefore didn’t differentiate “good” providers from “bad” providers. This will affect all anesthesia providers that were planning on using the Anesthesia Specialty Set to report and comply with the Quality category. The specialty sets were useful in previous years, but as we will see, a better pathway exists with the MVPs! Additionally, several Improvement Activities were retired for 2023, but this may not have a material effect on anesthesia providers due to some other changes within the program.Last month, CMS finalized the 2023 measures for all of medicine. You can review the specifications here (https://qpp.cms.gov/participation-lookup) to download the official list and details. For our registry, we can report on the following measures:
For those who are a little more interested in some of the details, the three point floor for measures without a benchmark has been removed. This served as a point floor for any providers reporting QCDR measures that were not widely adopted in the industry; but, again, this will not likely have an effect on any anesthesia providers moving forward.
The one other detail important for anesthesia providers is to confirm your Non-Patient Facing status with CMS. This status exempts anesthesia clinicians from reporting the Promoting Interoperability category, which is the old “Meaningful Use” program. The reason this is important for 2023 is that CMS will not automatically exclude CRNAs with this status; and, if you are identified as a patient-facing clinician, we need to review this special situation. We will be proactively checking your status; but, to confirm your own status, click here (https://qpp.cms.gov/participation-lookup).
If all of this seems a little overwhelming, I have great news and a solution for you. It is called the MIPS Value Pathways (MVP)!
MIPS Value Pathways
To simplify the entire process of reporting measures to CMS, the creation and use of an MVP for anesthesia is available next year. The MVP bundles a set of measures to report, rather than burdening providers to choose. For 2023, the compliance requirement for an MVP is to report four quality measures to include an outcome measure and two medium-weighted or one high-weighted improvement activity. The only catch to an MVP is that you must proactively register between April 1, 2023 and November 30, 2023.The measures to choose from are as follows:
Quality (Choose 4)
- #404: Anesthesiology Smoking Abstinence
- #424: Perioperative Temperature Management
- #430: Prevention of Post-Operative Nausea and Vomiting (PONY) - Combination Therapy
- #463: Prevention of Post-Operative Vomiting (POV) - Combination Therapy (Pediatrics)
- #477: Multimodal Pain Management (MIPS CQMs Specifications)
- AQI48: Patient-Reported Experience with Anesthesia
- AQI69: Intraoperative Antibiotic Redosing
Improvement Activities (2 Medium or 1 High)
- IA_BE_6: Regularly Assess Patient Experience of Care and Follow Up on Findings - High
- IA_BE_22: Improved practices that engage patients pre-visit - Medium
- IA_BMH_2: Tobacco use - Medium
- IA_CC_2: Implementation of improvements that contribute to more timely communication of test results - Medium
- IA_CC_15: PSH Care Coordination - High
- IA_CC_19: Tracking of clinician’s relationship to and responsibility for a patient by reporting MACRA patient relationship codes - High
- IA_EPA_1: Provide 24/7 Access to MIPS Eligible Clinicians or Groups Who Have Real-Time Access to Patient’s Medical Records - High
- IA_PSPA_1: Participation in an AHRQ-listed patient safety organization – Medium
- IA_PSPA_7: Use of QCDR data for ongoing practice assessment and improvements - Medium
- IA_PSPA_16: Use of decision support and standardized treatment protocols - Medium
- IA_PSPA_20: Leadership engagement in regular guidance and demonstrated commitment for implementing practice improvement changes - Medium
To illustrate how this works, ABC can automatically continue to report on your relationship codes through billing operations (measure IA_CC_19), and you can choose to report the following four quality measures to be fully compliant next year.
- #424: Perioperative Temperature Management
- #430: Prevention of Post-Operative Nausea and Vomiting (PONV)
- #463: Prevention of Post-Operative Vomiting (POV) - Combination Therapy (Pediatrics)
- #477: Multimodal Pain Management
This is the easiest way to meet compliance in 2023; but, if you are interested in learning more about this program, you can review the CMS website.
Bryan Sullivan, MSHS is Chief Quality Officer for ABC. He also serves as Chief Operating Officer for Plexus Technology Group (Plexus TG). Mr. Sullivan currently manages the MiraMed Qualified Clinical Data Registry (QCDR) and all other quality management matters for Plexus TG and ABC clients. Mr. Sullivan began his career with the implementation of clinical trial management platforms for pharmaceutical companies. He made the transition to healthcare IT in the anesthesia software space in 2008. Mr. Sullivan deployed anesthesia information management systems for eko systems, Inc., before joining ABC in 2011. He has a Master of Science degree in Health Sciences from George Washington University, as well as a Bachelor of Science degree in Business Administration from the College of William & Mary. Mr. Sullivan is also a Project Management Professional through the Project Management Institute (PMI). He can be reached at Bryan.Sullivan@AnesthesiaLLC.com. -
New Year, New Challenges
Happy New Year!
As we bring 2022 to a close, our question is simple: was this the new normal we had been waiting for since the challenges of the Pandemic? In some ways, it was. Most of our clients saw surgical volumes level out at pre-Covid levels. Beyond this basic reality, though, American healthcare continues to provide numerous challenges. Many practices simply went out of business, either through practice mergers or by becoming hospital employees. We did our best to track the issues and guide our clients through the turbulent waters of American healthcare. It is always difficult to know what priorities to focus on. I hope you will find this collection particularly interesting and relevant.
Our Bryan Sullivan leads us off with a very detailed discussion of what we can expect from the 2023 Quality Payment Program. Ever since the pay for performance concept first began to be implemented, there have been numerous questions from our clients about the details of each year’s program and the value of participating. Bryan does a great job of explaining how to be compliant.
Managing group practices effectively has always posed many challenges. We have worked hard to help clients navigate management challenges. Will Latham, a very experienced practice management consultant, shared some very practical suggestions gleaned from his 30 years in the business in his article, Cooperation Without Trust. He has a great way of getting to the heart of the issues with some very useful suggestions.
Our very own VP, Jody Locke, pulls the lens back on the current economic realities of anesthesia practice. Clients used to focus on the need to optimize collections, but Jody’s article reminds us that today’s challenge is about managing the whole budget and, where necessary, figuring out how to enroll the hospital in your practice. It is a very insightful compilation of his years of experience managing anesthesia practices across the country.
In this era of Facebook, Whatsapp, Instagram, Twitter and Tiktok, it is impossible to discuss strategic options without consideration of social media. Kristine Squiers, from our marketing department, dives into this interesting subject by addressing some of the most common questions we get asked. I am sure this will be the beginning of an interesting and ongoing discussion.
Attorney Mark Weiss often contributes to our journal, and his article about a $24.3 million judgment is a fascinating exploration of a topic few of us have seriously considered. The letters RFP are probably three of the scariest to anesthesia practice managers. Mark provides some very relevant suggestions for dealing with overzealous hospital administrators.
We all know there is a serious manpower shortage. There are obviously many implications, including increased subsidies so practices can recruit and retain a sufficient number of providers. Lorraine Morandi, one of Plexus Management Group’s managers, attempts to explore the nature and implications of the current CRNA shortage.
On behalf of our entire team, let me wish you a productive and profitable 2023. As always, we are particularly grateful for your comments and feedback on these pieces. We are especially interested in your suggestions for future topics.
With best wishes,
Tony Mira
Vice Chairman and Founder -
Today’s Anesthesia Economics: Coping with New Realities
Jody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services
Anesthesia Business Consultants, LLC, Jackson, MINavigating an anesthesia practice through the turbulent and murky waters of American healthcare has never been easy, but the unique challenges of today’s market have dramatically raised the bar, and many practices are simply opting out. It used to be that the key to success was quality care. If a team of qualified providers consistently provided reliable care that enhanced the patient’s surgical or obstetric experience, most practices enjoyed stable and long-term relationships with the facilities they served. The only thing that most anesthesia providers really had to worry about was what happened in the operating room or delivery suite. Now that is no longer the case. What happens outside the operating room and how providers respond to it is far more likely to determine the future of the practice. This gives new meaning to thinking outside the box.Today’s anesthesia challenges fall into three broad categories: getting adequately paid, maintaining a qualified team of providers and dealing with facility service expectations. It has never been so difficult to get adequately paid for the valuable services anesthesia providers administer. Recruiting and retaining an adequate team of qualified providers is becoming not only more expensive but more challenging.
Getting Paid for Anesthesia and Pain Management Services
Because of its complex method of calculating charges, anesthesia is unique among medical specialties. It is the only specialty where providers are paid for their time and the risks associated with the surgical procedure performed. While the complexity of anesthesia billing has historically served the specialty well, it is now inspiring payers to dissect its elements and write their own rules for payment. We consistently capture all the potentially billable elements of an anesthesia service only to have many of them modified during the adjudication of the claim. Let’s consider some of the clearest examples. The ASA suggests that the base value for a procedure should be modified based on unique patient and operative factors using the physical status and emergency modifiers, but Medicare has long since decided that these are needlessly discretionary and does not recognize them for payment. Anesthesia providers have been getting paid for the use of ultrasonic guidance (USG) to perform nerve blocks, but now these USG payments will soon be eliminated in many cases. The whole concept of billable anesthesia time is coming under ever greater scrutiny ever since the Centers for Medicare & Medicaid Services (CMS) decided to pay for time by the minute.Unlike most other countries across the globe, in the United States, a practice’s payer mix is its key to revenue potential. While five or six insurance plans tend to generate 80 percent of a practice’s revenue, the overall list of revenue sources can be very extensive, and each plan may have its own payment rules. We tend to focus on the distinction between public payers (Medicare, Medicaid, Workers Compensation, Tricare and Champus) and commercial PPO plans because the public plans tend to be the most severely discounted. Historically, practices have been able to make up for declining public payer rates through aggressive negotiation of commercial contracts. The problem is that, as the percentage of patients covered by the public payers continues to increase inexorably, commercial plans are becoming more intransigent in their willingness to increase their rates. The net impact of an aging population and its impact on payer mix is resulting in declining net yields per billed unit.
When it comes to collecting everything that is collectible for the valuable services anesthesia providers administer, there are three primary challenges that every practice must come to terms with. First, there is the fact that, as compared to office-based providers, anesthesiologists and certified registered nurse anesthetist (CRNAs) have no ongoing relationship with their patients; they rely on hospital staff to gather the critical demographic information necessary to submit claims and receive payment. Second, we live in a society where the expectation is that patients have insurance to cover their medical expenses; patient balances tend to be looked at as incidental and of lower priority to the patient than other bills such as mortgage or rent, utilities, cable, car payment and groceries. Third, while there are numerous effective strategies to collect the allowable from insurance, there are relatively few approaches that result in consistent collections from the patients themselves. It is these factors that explain why collecting the patient’s balance is often the Achilles heel of accounts receivable management.
The problem is further compounded by the challenge of defining patient responsibility, which falls into three distinct categories, each of which poses its own challenges. Usually, the largest category consists of patient balances after insurance. Most insurance plans will pay at least 80 percent of their allowable payment for a given service. Some patients will have secondary insurance or a plan that covers the 20 percent, but many do not. Obviously, collecting this patient portion is significant to the practice as no one wants to accept a 20 percent discount. Conscientious patients with the means will usually pay their portion. The reality is that, for many patients, the 20 percent due for the anesthesia bill is in addition to the 20 percent due for all the other specialists and the hospital. Even a relatively minor surgery can result in significant balances due from the patient. The number one reason for bankruptcy in the United States is medical bills.
And then there is the growing number of patients who do not have any insurance coverage at all or for whom there is no insurance of record. These are optimistically listed as self-pay patients. When there is valid insurance coverage, the provider at least gets something. When there is no insurance coverage, all bets are off, and the practice has no leverage to collect anything. Depending on the location of the practice, self-pay may mean no pay or discounted pay. The reality is that the cost of healthcare has gotten so expensive that the bills sent to them are cruel reminders of their desperate status. It should be noted that, in this era of cell phones with caller ID, most people do not answer calls associated with unrecognized numbers.A third subset of patients fall into a category called pre-paid, typically associated with cosmetic services. This is usually a small percentage of practice patients, but it should be a model for the management of self-pay patients across the board. The ideal scenario would be to obtain payment up front before the services are provided. However, this is an option not available to most anesthesia practices. Unfortunately, most practices simply do not have a mechanism to get even a prepayment. There have been some limited experiments by a few practices to have hospital employees ask for a pre-payment for anesthesia, but such experiments have been largely unsuccessful, except in the ambulatory environment.
Because so many charges do not get paid in full, accounts receivable management requires attention. Knowing when to continue to pursue and when to write off an unpaid balance is an aspect of practice management too few providers have come to understand and appreciate. It is no longer enough to just know your performance metrics; the key is to know what is changing and why.
Managing the Cost of Anesthesia Services
Determining a reasonable and appropriate cost for the provision of anesthesia services is a multi-factorial exercise with numerous variables. What makes the calculation especially challenging are the diverse variables: the size and configuration of the team and how it may need to be assessed and modified based on provider defection. Dynamic market factors make it especially difficult to structure a plan that will continue to meet the expectations of the customer today and into the future. In fact, more often than not, the real challenge is trying to meet customer expectations today, much less tomorrow. While many anesthesia practices used to present very stable organizations with loyal and committed members, such practices are now the exception rather than the rule. Never have so many practices decided to either merge or sell out in order to avoid the challenges of staying competitive and profitable. The days of the independent private anesthesia practice serving one facility, or a small collection of facilities, are waning.The biggest single cost for anesthesia is the cost of providers, physician anesthesiologists, CRNAs and physician assistants (PAs). Unlike other specialties where physicians typically have extensive office and overhead expenses, the overhead burden for anesthesia practices rarely exceeds 10 percent. What this means is that there needs to be enough revenue generated from collections to cover the cost of the salaries and benefits of the providers plus any overhead costs such as billing fees, accounting charges and legal expenses. Because provider salaries are so high, a minor miscalculation with regard to the number of providers needed can prove disastrous.
There is no greater challenge today than knowing what is a fair and reasonable compensation package for a physician anesthesiologist, a CRNA or a PA. There are a number of national survey organizations that provide market data, but none is without its shortcomings or flaws. The fundamental problem is that most surveys show W2 salary data. Because benefits packages vary considerably it is never clear how to compare and evaluate different packages. It is also true that no two anesthesia providers work the same or have an equally challenging or demanding schedule. When trying to assess the competitiveness of its CRNA package, the managers soon noticed that each of the practices they were trying to compare their package to had different call burdens and very different types of cases. Diverse market factors can have a significant impact. It is not always just the value of a compensation package that determines whether a given provider will decide to join a particular practice. It would be nice if determining the appropriate compensation package was as clear-cut as determining the profitability of a business, but it is not, and there is always a certain amount of wishful thinking.
A typical benchmark for anesthesia provider compensation is the MGMA survey. Sullivan Cotter also provides benchmark data. Many consultants prefer the MGMA data, but both surveys have their limitations. They are only conducted annually, and the sample sizes are limited. Typically, MGMA data comes from private anesthesia practices while Sullivan Cotter data comes from hospitals. Ideally, one should always use reference data from a variety of sources, but this is not always reasonable given unique practice circumstances. Also, the real point is if a practice cannot attract providers with compensation based on national survey data, then the survey data is basically useless.
The variety of anesthesia staffing options available to individual anesthesia practices is another unique challenge, especially given the fact that determining the optimum ratio of physicians to CRNAs involves a careful analysis of how each category of provider is actually used by the practice. Many assume that, since physician compensation is higher than CRNA compensation, they might assume that using more CRNAs will save money; but this is definitely not the case unless CRNAs are going to practice independently without any physician medical direction. The fact is that CRNA compensation has been rising, a fact that greatly changes the relative cost advantage. It might seem obvious that having one physician medically direct four CRNAs (each managing a busy operating room in a surgi-center with a favorable payer mix) is less expensive and more profitable than having four physicians provide the same services. This is an extreme example, however, and a detailed assessment of staffing options by surgical venue can reveal a variety of profitability levels. Determining a staffing model is inevitably a function of three factors: how staffing has been historically provided, how easy it is to change staffing ratios and current compensation expectations for each category of provider. It is quite common to hear hospital administrators suggest that the practice needs to leverage its physicians with more CRNAs, but this is often not the most cost-effective option.Anesthesia compensation models can be another confounding factor in determining the cost of the anesthesia team. Many physicians in physician-only practices in the western United States believe that it is possible to incentivize providers to be more productive. For some physicians, the mode of compensation may also be a form of incentive if there is sufficient flexibility to generate more income by being more productive. A well-known MGMA speaker once explained that, if you have seen one anesthesia compensation plan, you have seen one anesthesia compensation plan. Many practices will go to great lengths to provide unique incentives for their members.
There is no question about it: we are seeing increasing numbers of provider defections among anesthesia practices. One of our client practices recently shared that it had experienced more than a dozen years with only minimal providers leaving only to be overwhelmed by providers leaving in the past year. They are not alone. If a single provider retires or leaves the practice, it is generally not unexpected or disruptive. But when multiple providers leave in a short period of time, it can be very disruptive on a number of levels. There is always the question of why they are leaving and what it says about the level of confidence providers have in the future of the practice. Stressful hospital contract negotiations can have a particularly disruptive impact, especially when there is concern about the potential outcome of contract negotiations. The worst possible scenario is when members of a group practice start to see the defections as a precursor of things to come. The real problem is that it is typically the most qualified providers who leave first, because they have the best options. There is nothing worse than the death spiral inspired by provider defections, but it is all too common a phenomenon.
There is clearly a manpower shortage for both anesthesiologists and CRNAs today. Provider training programs are simply not keeping up with the increasing number of anesthetizing locations that need to be covered. The result is a buyer’s market for anesthesia providers. Any provider unhappy with his or her work situation can easily find other options. This moving around has created a whole new set of recruiting challenges for many anesthesia practices.Where does all this leave us now? For many of today’s anesthesia practices, the greatest challenge is to recruit and retain enough qualified providers to meet the service expectations of the various clients. This is proving to be a challenge that requires an entirely new set of skills and resources. It used to be that, whatever level of coverage was requested, anesthesia practices would attempt to deliver, but the time has come where anesthesia practices must focus more on resetting customer expectations. Every service has a cost, and this is what hospital administrators must come to understand and appreciate.
Negotiating an Anesthesia Subsidy
The traditional anesthesia practice model was based on a private group contracting with a facility for the exclusive right to provide anesthesia services. There was even a time when fee for service revenue from professional services provided would generate sufficient collections to cover the cost of providing the service. Those were the good old days before service expectations began to outstrip revenue potential. Today’s practices are having to develop an entirely new practice model based on today’s realities. Hospital subsidy revenue is ever more important to practice budgets. While many practices chose to outsource their billing to maximize collections, they are now having to hire outside consultants to negotiate reasonable contracts with adequate subsidies. This, however, means that anesthesia groups are having to deal with the flipside of the coin. The more hospitals have to pay for anesthesia services, the more they want accountability and collaboration. The key to the future of today’s practices is partnership with its customers. As a quintessential service organization, each anesthesia practice must focus on a value proposition that not only enhances its relationship with its facilities, but which enhances their value in the competitive healthcare market.
There was a time when private anesthesia practices were reluctant to open their books to administration. Transparency is now an essential prerequisite for a meaningful negotiation. The only way to convince administration that you need financial support is to show exactly why you need support. Financial disclosure involves a complete review of assumptions. What are the coverage and call requirements, and how many providers are needed? What is the status of the current team? How many providers have recently left; how many are considering leaving; and how many will it take to meet the specific coverage and call expectations of the facility? Every practice must be able to justify its assumptions with regard to staffing and manpower. As a practice makes its case for continuing the relationship, the administration will inevitably push back. Is the practice well managed? Are there substandard providers? Can the practice clearly demonstrate it is the best anesthesia solution for the facility?Once the lawyers get involved, agreements evolve from simple letters of intent to complex documents with lots of legalese and fine print. If you compare today’s anesthesia service agreements to those of 20 years ago, it becomes obvious how many layers of government regulation and legal precautions have been added in. Among the most interesting and often challenging aspects of today’s agreements are the performance metrics. Somehow, anesthesia providers have become saddled with the efficient and effective management of the operating rooms as measured in such things as first case start times, average turnover times and case cancelations for ambulatory facilities. The introduction of automated anesthesia records provides considerably more data that is easier to obtain, but it also raises expectations with regard to what is available. Yes, it is true that anesthesia practices have more and better data about what actually happens in the operating room and delivery suite, but managing the database and mining it effectively opens a whole new world of opportunity for most practices that they are not prepared for. It used to be that documenting the care provided was the least of a provider’s concerns, and yet many now complain that the documentation requirements of anesthesia are more challenging than providing the care. It is almost like playing a game where no one really knows the rules or what it takes to win.
Virtually every contract renegotiation today involves a detailed financial pro forma. In theory, these should not be so complicated. The basic idea is to project the cost of the services requested and the revenue potential for the billable services rendered and show the variance, which is what the facility is being asked to pay. In reality, there is nothing simple about these pro formas, and most practices recognize the need to bring in consultants to guide them through the process. Not only are there many assumptions that have to be tested, especially with regard to the revenue potential of the practice, but the pro forma actually needs to reflect the dynamic nature of the market. Failure to factor in the major risk factors can result in disaster. As the old saying goes, anyone can get the numbers right today, but will they be right tomorrow?
Anesthesia practices tended to be haunted by these three-letter acronyms: RFP and FMV. The first, the request for proposal, is the facility’s attempt to validate the group’s practice model against the market. Their fair market valuation may also be an attempt to have an independent third party confirm a reasonable pro forma. It is not always clear at the onset if the purpose of the exercise is to confirm that the current practice is the best solution or whether it should be replaced. These are just a couple examples of today’s practice management vocabulary that providers must master in order to remain current and viable.And so, at the end of the day, what really makes a difference? It is all about the relationship between the practice and its customers. If the relationship is strong and if there is respect and trust on the part of administration, there is a good chance that the relationship will continue. The administration must have confidence that the relationship represents an alignment of incentives and holds the best prospect for a win-win scenario. We used to hear from clients that they only met with administration to renegotiate the contract and therein lay the challenge for the practice: they were little more than a line item in the hospital budget. The name of the game today is partnership. Administration must believe that yours is the best option, that you provide the best service and that you can help them navigate the future.
Final Thoughts
Strategic planning consultants love to remind their clients that the beliefs and strategies that got the practice to where it is today will most likely not get it to where it needs to be tomorrow. The best managers are aggressive students of the business. There is a tool consultants often use called a SWOT analysis, standing for strength, weaknesses, opportunities and threats. It is an invaluable tool that practices would be well advised to apply and monitor continuously.
Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants, LLC. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@ AnesthesiaLLC.com. -
Cooperation Without Trust
Will Latham, MBA, President
Latham Consulting Group, Inc., Chattanooga, TNWouldn’t it be great if all the physicians in your group fully trusted each other at all times on all issues? If that’s how it works in your group, count your blessings.In most cases, however, there is at least some distrust among members of anesthesiology groups. This is the result of differing opinions, differing goals (often due to age and financial situation), and what we have found to be a naturally forming level of paranoia.
This issue is complicated by the fact that most, (but not all) anesthesiologists are conflict avoiders. They would rather avoid a situation than confront their partners on issues.
Yet, even without full trust and conflict avoidance among group members, anesthesiology groups need to move forward. And to move forward, they must decide which direction they will move.
Here are four methods we have seen groups use to make decisions and move forward.
1. Commit to Support Group Decisions
There is an adage that erroneously gets credence: individual physicians believe that “if I didn’t vote for it, or I don’t agree with it, then I don’t have to do it.”
If this is the normative behavior of your group, you will always be troubled in making real decisions and moving forward. To improve the situation, your group needs to ask and answer three key questions:
- How will we make decisions as a group? Typically, this is through discussion and a vote.
- What is expected of each physician once the group has decided on an issue? The shareholders should pre-commit to support it, do it and not sabotage it.
- What are a physician’s options if they don’t like the decision? The shareholders should commit that they will follow ONLY one of the following options:
- Do it anyway, that’s group practice.
- Try to get it changed in the appropriate forum, such as a group meeting, but keep supporting or doing it until changed.
- Self-select yourself out of the group.
2. Can Three by Five Cards Really Save Us?
When the members of an anesthesiology group meet, at either shareholders or board meetings, they typically deal with issues that require a decision. Unfortunately, voting doesn’t work very well in many medical groups for the following reasons:- Some group members believe the idea of actually voting is too “formal.”
- Some groups think they have consensus because no one speaks up (or only a few speak up and the thought is the rest are willing to go along). These groups are fooling themselves because, when people don’t speak up, it typically means they disagree. In addition, if you think you have consensus, why not vote to make sure you do?
- Because many physicians are conflict avoiders. Sometimes discussions go on and on because people don’t want to raise their hands to vote and possibly enter into conflict with those that don’t agree with them. This can make meetings last much longer than they need to.
In my opinion, it’s best to formally vote on issues to make sure the group has the needed majority or super-majority vote. This assumes that the group has gone through a process where the group members agree to support group decisions as noted above.
To deal with conflict avoidance, I am seeing more and more groups move to using “secret ballots” for their voting process. Most groups use secret ballots for electing their board and officers, but some groups use them when they need to vote on controversial issues, or in more and more cases, on all issues. Why are secret ballots useful?
- They allow the individuals to “vote their conscience” with less fear of retribution.
- They avoid one physician “bullying” another physician into changing their vote.
- They often speed up a meeting because people don’t delay voting to put off conflict.
There are several ways to implement secret ballots—here are two:
- Use three-by-five cards as the secret ballots.
- We have observed some groups starting to use “audience response systems.” One medical group president recently told us that his group has begun using such a voting system for all issues and that they had cut about 25 percent off the time of every meeting by using the system.
Groups that use secret ballots for all their issues have told us that there is only one potentially negative outcome—that people will push too quickly for a vote. Therefore, it is up to the meeting manager to make sure that the group has had a full discussion of the issue prior to voting.
3. Fair Elections
If elections are not conducted in a fair and reasonable method, it taints a group’s governance and reduces physicians’ adherence to group decisions. So naturally, election voting should allow for people to be nominated, and then secret ballot used for the actual vote.But sometimes it’s difficult to make a change when one is needed. This is another result of conflict avoidance. If someone in power doesn't want to lose their position, it is difficult for other shareholders to challenge them. This can result in the group not electing the people believed best to lead, and a feeling that the whole process is unfair and thus tainted.
One way out of this conundrum is to alter the election process to that as shown in Exhibit 1. By using this method, no one has to stand up and challenge the current leaders.
4. Revisiting Issues
Many medical groups make a decision and then revisit it over and over again.This situation comes about when a few members of the group do not get their way in the first vote. They then use this strategy to either torture the group into changing the decision, or to paralyze the group.
When other group members state their frustration about the problems revisiting an issue will cause, the physicians who want to revisit the issue typically respond that additional information has come to light which they believe should be considered in making the decision. This can go on ad infinitum and the ability to pursue key opportunities (or the ability to avoid key threats) can be lost.
Many organizations suffer from this problem, but the situation is more challenging for medical groups where the shareholder physicians are usually equal owners of the practice. Some physician shareholders believe that equal ownership gives them the right to have a say about every issue at any time they want (and often waste precious group meeting time). And they use this right as a torture technique to get what they want.
One way to reduce the use of this torture technique (revisiting issues over and over again) is to put a “speed bump” for items to return to the agenda for discussion.
For example, the group could implement a policy that requires 30 percent of the shareholders to sign a document asking to bring an item back to the floor for re-discussion once a decision has been made (it is important that they sign a document, rather than someone say “I had 30 percent of the people say they’d like to re-discuss this issue”).
This policy doesn’t close the door to re-discussing an issue (if more than 30 percent want to re-discuss an issue, the group probably should). However, it will typically reduce the number of times this torture technique is used.
Some will Fight This
Let’s be realistic: there will be those in the group who will fight the implementation of the above ideas. But let’s also be truthful: the reason they will fight it is that they are getting something out of the current state of dysfunction.
So, don’t let the few prevent the group from making good changes that will benefit the entire group, rather than the individual.
For more than 30 years, Will Latham has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 135 medical practices representing over 1,300 physicians. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at wlatham@lathamconsulting.com. -
2023 Social Media and the Anesthesiology Practice: Marketing and Your Online Reputation
Kristine E. Squiers, MS
Social Media Specialist, MiraMed Global Services, Jackson, MIThere have been big changes in social media over the last year, with many more promised as Congress consistently looks for answers on regulation of social media and the social media platforms compete. This article looks at best practices for anesthesiologists for 2023, areas of concern and pitfalls to avoid.
What Should I Post?
Anesthesiologists might entertain a range of reasons to market on social media, such as providing information about the practice, emergency closures, new employees or business accomplishments. They might also want to provide information about anesthesia, procedures and insurance. Anesthesiologists and anesthesia groups with aspirations of securing larger contracts, mergers and investments can utilize social media to build a brand.There are many ways the anesthesia industry is presented and marketed in social media. Many comedy segments feature doctors, nurses or patients. Sometimes anesthesiologists present themselves seriously, providing information about procedures, equipment, instruments or medications. Some clinics take a broad approach and provide social media under the branded name of the practice and utilize the platform to build a branded identity. All of these are legitimate social media marketing methods for 2023.
Social media is interactive. Social media is dynamic. Although you can limit the amount of interaction, best practices favor more interaction. This means, if you want to build more visibility to market your practice, more interaction on your part, and your followers, is required. The less you do, the slower and less dynamic the response. The less interesting your posts are, the longer it takes to build an audience.
Managing Your Brand
One of the biggest concerns for healthcare providers in 2023 is their own personal safety and anonymity. Before posting anything, remember to consider that there are a lot of people who will be able to identify you or your staff if you post any of that information, so be aware of your level of exposure. Also be aware that images you post can have data embedded that share location information. Should your posts become very popular, over time your following could be thousands or even millions of people from all over the world.
Another concern is that the more visible your practice is online, the more likely you are to draw negative reviews, comments and images posted against you. If your goal is brand recognition and establishing yourself as a leader in the marketplace, act with prudence. Attempt to use best practices for handling the onslaught of negativity that inevitably will occur at some point. Consider reading this helpful article to avoid costly mistakes. https://www.yotpo.com/resources/how-to-harness-the-positive-power-of-negative-reviews/
Impacts of Congressional Regulations
In 2023, social media will have another year of battling misinformation and disinformation. Scandalous, unusual, riveting, salacious and conspiratorial posts rise above the millions of boring voices. For the professional anesthesiologist, 2023 posts should provide important information for your patients, so they do not turn to poor sources.
“Misinformation and disinformation—misinformation as inaccuracy and errors and disinformation as a falsehood created on purpose and the spread of it by malicious individuals (human or bots)—gain momentum from the desire to find a solution to a particular disease or illness by patients or their relatives, who inadvertently contribute to spreading misleading information.”1
Because hearings in congress continue to identify genuine concerns about the health, safety and security of social media users and the United States as a whole, many in congress believe that it is time to add to or change the only legislation governing social media:
“The last major legislation to regulate social media was the Communications Decency Act (CDA) passed in 1996. This bill governs most social media platforms, and section 230 of the CDA, in particular, limits platforms’ liability for content published by users. These companies, such as Instagram, Facebook and Twitter have contended that they are noneditorial platforms and thus they should not be held responsible for what is published on their sites. This interpretation may have been believable 25 years ago, before the growth of social media or the increasing power of algorithmic content curation, but this interpretation no longer reflects reality.”2
It is likely we will see social media regulation proposed by congress in 2023.
Which Platform Should I Use?
Facebook is the most popular platform for patients to use for healthcare information. The next two most popular platforms for healthcare information are YouTube followed by Twitter. All three platforms are great for branding, but Facebook is seeing a decline in younger users. YouTube is seeing a steady increase in all users. Twitter is seeing instability, record losses and a questionable future.Twitter is experiencing a massive changeover since purchased by Elon Musk. This changeover has jeopardized its security protocols, leading to many data vulnerabilities as well as fake and fraudulent accounts popping up as verified.3
Most companies are pulling back on advertising, and established accounts are considering changing platforms.4
If you are using Twitter, you are going to see changes in 2023, so prepare now for a backup plan, such as an alternate platform. In 2023 you may want to consider utilizing your Google Business Profile which appears in Google search results and on the Google Map. You can post images, ads, videos, statements, information and more. Google Business Profiles are an easy way to manage your online reputation and build your brand. To find out more about getting your own Google Business Profile use this link: https://www.google.com/business/.
In conclusion, it is likely that we will see congress continue holding hearings on the regulation of social media. Questions of social impact, impact on psychological wellbeing, impact on homeland security and impact on the stock market are all open considerations that may yield unexpected changes. Be prepared with a backup plan, as the onslaught of change washing over these platforms could potentially impact you. Always consider safety and privacy issues before posting, and finally be aware that you will be attacked with negative comments, so prepare your responses.
Have a wonderful 2023!
1 A New Application of Social Impact in Social Media for Overcoming Fake News in Health by Cristina M. Pulido 1ORCID, Laura Ruiz-Eugenio 2,*ORCID, Gisela Redondo-Sama 3 and Beatriz Villarejo-Carballido 4ORCID
2 Maybe We Should Make Some Rules Here: A Framework for Social Media, Harwood, Graham. Chicago Policy Review (Online); Chicago (Jan 17, 2022). https://www.proquest.com/openview/1ab243336dcb4e6fdbc2c94ce51aa8c8/1?pq-origsite=gscholar&cbl=1576347
3 https://www.cnn.com/2022/11/10/tech/twitter-executives-resign
Kristine E. Squiers, MS manages all social media for MiraMed Global Services and its Family of Companies. Kristine began her digital marketing career in 2008, and has extensive experience in search engine optimization, digital advertising, website management, content marketing, lead generation and social media. Kristine has a Master of Science in Psychology with a specialization in Industrial and Organizational Psychology, as well as Graduate Certificates in Diversity Studies and Business Management.
 Thankfully, little has changed within each category for 2023. For example, the data completeness requirement remains at 70 percent for Quality category reporting, meaning clinicians will need to report on 70 percent of each measure’s eligible population to be counted. The big news is that a widely reported Quality measure will be retired. MIPS 76 (Prevention of Central Venous Catheter - Related Bloodstream Infections) is no longer an eligible measure because most clinicians were compliant and therefore didn’t differentiate “good” providers from “bad” providers. This will affect all anesthesia providers that were planning on using the Anesthesia Specialty Set to report and comply with the Quality category. The specialty sets were useful in previous years, but as we will see, a better pathway exists with the MVPs! Additionally, several Improvement Activities were retired for 2023, but this may not have a material effect on anesthesia providers due to some other changes within the program.
Thankfully, little has changed within each category for 2023. For example, the data completeness requirement remains at 70 percent for Quality category reporting, meaning clinicians will need to report on 70 percent of each measure’s eligible population to be counted. The big news is that a widely reported Quality measure will be retired. MIPS 76 (Prevention of Central Venous Catheter - Related Bloodstream Infections) is no longer an eligible measure because most clinicians were compliant and therefore didn’t differentiate “good” providers from “bad” providers. This will affect all anesthesia providers that were planning on using the Anesthesia Specialty Set to report and comply with the Quality category. The specialty sets were useful in previous years, but as we will see, a better pathway exists with the MVPs! Additionally, several Improvement Activities were retired for 2023, but this may not have a material effect on anesthesia providers due to some other changes within the program.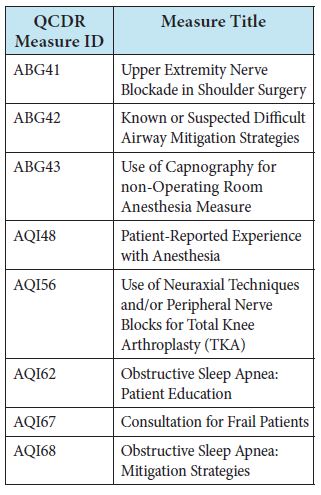
 To simplify the entire process of reporting measures to CMS, the creation and use of an MVP for anesthesia is available next year. The MVP bundles a set of measures to report, rather than burdening providers to choose. For 2023, the compliance requirement for an MVP is to report four quality measures to include an outcome measure and two medium-weighted or one high-weighted improvement activity. The only catch to an MVP is that you must proactively register between April 1, 2023 and November 30, 2023.
To simplify the entire process of reporting measures to CMS, the creation and use of an MVP for anesthesia is available next year. The MVP bundles a set of measures to report, rather than burdening providers to choose. For 2023, the compliance requirement for an MVP is to report four quality measures to include an outcome measure and two medium-weighted or one high-weighted improvement activity. The only catch to an MVP is that you must proactively register between April 1, 2023 and November 30, 2023. Bryan Sullivan, MSHS is Chief Quality Officer for ABC. He also serves as Chief Operating Officer for Plexus Technology Group (Plexus TG). Mr. Sullivan currently manages the MiraMed Qualified Clinical Data Registry (QCDR) and all other quality management matters for Plexus TG and ABC clients. Mr. Sullivan began his career with the implementation of clinical trial management platforms for pharmaceutical companies. He made the transition to healthcare IT in the anesthesia software space in 2008. Mr. Sullivan deployed anesthesia information management systems for eko systems, Inc., before joining ABC in 2011. He has a Master of Science degree in Health Sciences from George Washington University, as well as a Bachelor of Science degree in Business Administration from the College of William & Mary. Mr. Sullivan is also a Project Management Professional through the Project Management Institute (PMI). He can be reached at Bryan.Sullivan@AnesthesiaLLC.com.
Bryan Sullivan, MSHS is Chief Quality Officer for ABC. He also serves as Chief Operating Officer for Plexus Technology Group (Plexus TG). Mr. Sullivan currently manages the MiraMed Qualified Clinical Data Registry (QCDR) and all other quality management matters for Plexus TG and ABC clients. Mr. Sullivan began his career with the implementation of clinical trial management platforms for pharmaceutical companies. He made the transition to healthcare IT in the anesthesia software space in 2008. Mr. Sullivan deployed anesthesia information management systems for eko systems, Inc., before joining ABC in 2011. He has a Master of Science degree in Health Sciences from George Washington University, as well as a Bachelor of Science degree in Business Administration from the College of William & Mary. Mr. Sullivan is also a Project Management Professional through the Project Management Institute (PMI). He can be reached at Bryan.Sullivan@AnesthesiaLLC.com.
 Navigating an anesthesia practice through the turbulent and murky waters of American healthcare has never been easy, but the unique challenges of today’s market have dramatically raised the bar, and many practices are simply opting out. It used to be that the key to success was quality care. If a team of qualified providers consistently provided reliable care that enhanced the patient’s surgical or obstetric experience, most practices enjoyed stable and long-term relationships with the facilities they served. The only thing that most anesthesia providers really had to worry about was what happened in the operating room or delivery suite. Now that is no longer the case. What happens outside the operating room and how providers respond to it is far more likely to determine the future of the practice. This gives new meaning to thinking outside the box.
Navigating an anesthesia practice through the turbulent and murky waters of American healthcare has never been easy, but the unique challenges of today’s market have dramatically raised the bar, and many practices are simply opting out. It used to be that the key to success was quality care. If a team of qualified providers consistently provided reliable care that enhanced the patient’s surgical or obstetric experience, most practices enjoyed stable and long-term relationships with the facilities they served. The only thing that most anesthesia providers really had to worry about was what happened in the operating room or delivery suite. Now that is no longer the case. What happens outside the operating room and how providers respond to it is far more likely to determine the future of the practice. This gives new meaning to thinking outside the box. Because of its complex method of calculating charges, anesthesia is unique among medical specialties. It is the only specialty where providers are paid for their time and the risks associated with the surgical procedure performed. While the complexity of anesthesia billing has historically served the specialty well, it is now inspiring payers to dissect its elements and write their own rules for payment. We consistently capture all the potentially billable elements of an anesthesia service only to have many of them modified during the adjudication of the claim. Let’s consider some of the clearest examples. The ASA suggests that the base value for a procedure should be modified based on unique patient and operative factors using the physical status and emergency modifiers, but Medicare has long since decided that these are needlessly discretionary and does not recognize them for payment. Anesthesia providers have been getting paid for the use of ultrasonic guidance (USG) to perform nerve blocks, but now these USG payments will soon be eliminated in many cases. The whole concept of billable anesthesia time is coming under ever greater scrutiny ever since the Centers for Medicare & Medicaid Services (CMS) decided to pay for time by the minute.
Because of its complex method of calculating charges, anesthesia is unique among medical specialties. It is the only specialty where providers are paid for their time and the risks associated with the surgical procedure performed. While the complexity of anesthesia billing has historically served the specialty well, it is now inspiring payers to dissect its elements and write their own rules for payment. We consistently capture all the potentially billable elements of an anesthesia service only to have many of them modified during the adjudication of the claim. Let’s consider some of the clearest examples. The ASA suggests that the base value for a procedure should be modified based on unique patient and operative factors using the physical status and emergency modifiers, but Medicare has long since decided that these are needlessly discretionary and does not recognize them for payment. Anesthesia providers have been getting paid for the use of ultrasonic guidance (USG) to perform nerve blocks, but now these USG payments will soon be eliminated in many cases. The whole concept of billable anesthesia time is coming under ever greater scrutiny ever since the Centers for Medicare & Medicaid Services (CMS) decided to pay for time by the minute. And then there is the growing number of patients who do not have any insurance coverage at all or for whom there is no insurance of record. These are optimistically listed as self-pay patients. When there is valid insurance coverage, the provider at least gets something. When there is no insurance coverage, all bets are off, and the practice has no leverage to collect anything. Depending on the location of the practice, self-pay may mean no pay or discounted pay. The reality is that the cost of healthcare has gotten so expensive that the bills sent to them are cruel reminders of their desperate status. It should be noted that, in this era of cell phones with caller ID, most people do not answer calls associated with unrecognized numbers.
And then there is the growing number of patients who do not have any insurance coverage at all or for whom there is no insurance of record. These are optimistically listed as self-pay patients. When there is valid insurance coverage, the provider at least gets something. When there is no insurance coverage, all bets are off, and the practice has no leverage to collect anything. Depending on the location of the practice, self-pay may mean no pay or discounted pay. The reality is that the cost of healthcare has gotten so expensive that the bills sent to them are cruel reminders of their desperate status. It should be noted that, in this era of cell phones with caller ID, most people do not answer calls associated with unrecognized numbers. Determining a reasonable and appropriate cost for the provision of anesthesia services is a multi-factorial exercise with numerous variables. What makes the calculation especially challenging are the diverse variables: the size and configuration of the team and how it may need to be assessed and modified based on provider defection. Dynamic market factors make it especially difficult to structure a plan that will continue to meet the expectations of the customer today and into the future. In fact, more often than not, the real challenge is trying to meet customer expectations today, much less tomorrow. While many anesthesia practices used to present very stable organizations with loyal and committed members, such practices are now the exception rather than the rule. Never have so many practices decided to either merge or sell out in order to avoid the challenges of staying competitive and profitable. The days of the independent private anesthesia practice serving one facility, or a small collection of facilities, are waning.
Determining a reasonable and appropriate cost for the provision of anesthesia services is a multi-factorial exercise with numerous variables. What makes the calculation especially challenging are the diverse variables: the size and configuration of the team and how it may need to be assessed and modified based on provider defection. Dynamic market factors make it especially difficult to structure a plan that will continue to meet the expectations of the customer today and into the future. In fact, more often than not, the real challenge is trying to meet customer expectations today, much less tomorrow. While many anesthesia practices used to present very stable organizations with loyal and committed members, such practices are now the exception rather than the rule. Never have so many practices decided to either merge or sell out in order to avoid the challenges of staying competitive and profitable. The days of the independent private anesthesia practice serving one facility, or a small collection of facilities, are waning. The variety of anesthesia staffing options available to individual anesthesia practices is another unique challenge, especially given the fact that determining the optimum ratio of physicians to CRNAs involves a careful analysis of how each category of provider is actually used by the practice. Many assume that, since physician compensation is higher than CRNA compensation, they might assume that using more CRNAs will save money; but this is definitely not the case unless CRNAs are going to practice independently without any physician medical direction. The fact is that CRNA compensation has been rising, a fact that greatly changes the relative cost advantage. It might seem obvious that having one physician medically direct four CRNAs (each managing a busy operating room in a surgi-center with a favorable payer mix) is less expensive and more profitable than having four physicians provide the same services. This is an extreme example, however, and a detailed assessment of staffing options by surgical venue can reveal a variety of profitability levels. Determining a staffing model is inevitably a function of three factors: how staffing has been historically provided, how easy it is to change staffing ratios and current compensation expectations for each category of provider. It is quite common to hear hospital administrators suggest that the practice needs to leverage its physicians with more CRNAs, but this is often not the most cost-effective option.
The variety of anesthesia staffing options available to individual anesthesia practices is another unique challenge, especially given the fact that determining the optimum ratio of physicians to CRNAs involves a careful analysis of how each category of provider is actually used by the practice. Many assume that, since physician compensation is higher than CRNA compensation, they might assume that using more CRNAs will save money; but this is definitely not the case unless CRNAs are going to practice independently without any physician medical direction. The fact is that CRNA compensation has been rising, a fact that greatly changes the relative cost advantage. It might seem obvious that having one physician medically direct four CRNAs (each managing a busy operating room in a surgi-center with a favorable payer mix) is less expensive and more profitable than having four physicians provide the same services. This is an extreme example, however, and a detailed assessment of staffing options by surgical venue can reveal a variety of profitability levels. Determining a staffing model is inevitably a function of three factors: how staffing has been historically provided, how easy it is to change staffing ratios and current compensation expectations for each category of provider. It is quite common to hear hospital administrators suggest that the practice needs to leverage its physicians with more CRNAs, but this is often not the most cost-effective option. There is clearly a manpower shortage for both anesthesiologists and CRNAs today. Provider training programs are simply not keeping up with the increasing number of anesthetizing locations that need to be covered. The result is a buyer’s market for anesthesia providers. Any provider unhappy with his or her work situation can easily find other options. This moving around has created a whole new set of recruiting challenges for many anesthesia practices.
There is clearly a manpower shortage for both anesthesiologists and CRNAs today. Provider training programs are simply not keeping up with the increasing number of anesthetizing locations that need to be covered. The result is a buyer’s market for anesthesia providers. Any provider unhappy with his or her work situation can easily find other options. This moving around has created a whole new set of recruiting challenges for many anesthesia practices. There was a time when private anesthesia practices were reluctant to open their books to administration. Transparency is now an essential prerequisite for a meaningful negotiation. The only way to convince administration that you need financial support is to show exactly why you need support. Financial disclosure involves a complete review of assumptions. What are the coverage and call requirements, and how many providers are needed? What is the status of the current team? How many providers have recently left; how many are considering leaving; and how many will it take to meet the specific coverage and call expectations of the facility? Every practice must be able to justify its assumptions with regard to staffing and manpower. As a practice makes its case for continuing the relationship, the administration will inevitably push back. Is the practice well managed? Are there substandard providers? Can the practice clearly demonstrate it is the best anesthesia solution for the facility?
There was a time when private anesthesia practices were reluctant to open their books to administration. Transparency is now an essential prerequisite for a meaningful negotiation. The only way to convince administration that you need financial support is to show exactly why you need support. Financial disclosure involves a complete review of assumptions. What are the coverage and call requirements, and how many providers are needed? What is the status of the current team? How many providers have recently left; how many are considering leaving; and how many will it take to meet the specific coverage and call expectations of the facility? Every practice must be able to justify its assumptions with regard to staffing and manpower. As a practice makes its case for continuing the relationship, the administration will inevitably push back. Is the practice well managed? Are there substandard providers? Can the practice clearly demonstrate it is the best anesthesia solution for the facility? Anesthesia practices tended to be haunted by these three-letter acronyms: RFP and FMV. The first, the request for proposal, is the facility’s attempt to validate the group’s practice model against the market. Their fair market valuation may also be an attempt to have an independent third party confirm a reasonable pro forma. It is not always clear at the onset if the purpose of the exercise is to confirm that the current practice is the best solution or whether it should be replaced. These are just a couple examples of today’s practice management vocabulary that providers must master in order to remain current and viable.
Anesthesia practices tended to be haunted by these three-letter acronyms: RFP and FMV. The first, the request for proposal, is the facility’s attempt to validate the group’s practice model against the market. Their fair market valuation may also be an attempt to have an independent third party confirm a reasonable pro forma. It is not always clear at the onset if the purpose of the exercise is to confirm that the current practice is the best solution or whether it should be replaced. These are just a couple examples of today’s practice management vocabulary that providers must master in order to remain current and viable. Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants, LLC. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at
Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants, LLC. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at  Wouldn’t it be great if all the physicians in your group fully trusted each other at all times on all issues? If that’s how it works in your group, count your blessings.
Wouldn’t it be great if all the physicians in your group fully trusted each other at all times on all issues? If that’s how it works in your group, count your blessings. When the members of an anesthesiology group meet, at either shareholders or board meetings, they typically deal with issues that require a decision. Unfortunately, voting doesn’t work very well in many medical groups for the following reasons:
When the members of an anesthesiology group meet, at either shareholders or board meetings, they typically deal with issues that require a decision. Unfortunately, voting doesn’t work very well in many medical groups for the following reasons: If elections are not conducted in a fair and reasonable method, it taints a group’s governance and reduces physicians’ adherence to group decisions. So naturally, election voting should allow for people to be nominated, and then secret ballot used for the actual vote.
If elections are not conducted in a fair and reasonable method, it taints a group’s governance and reduces physicians’ adherence to group decisions. So naturally, election voting should allow for people to be nominated, and then secret ballot used for the actual vote.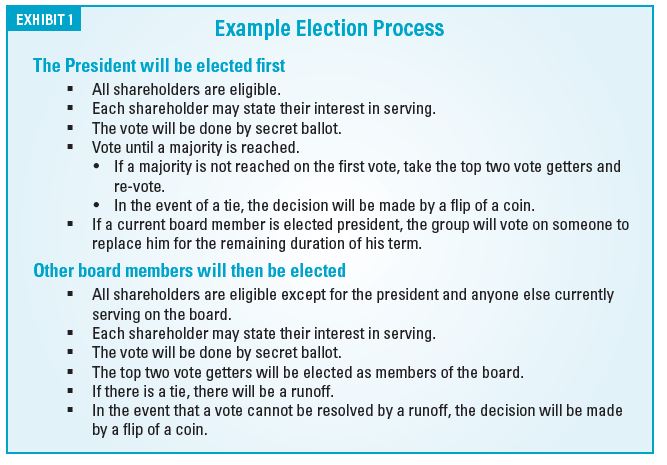
 Many medical groups make a decision and then revisit it over and over again.
Many medical groups make a decision and then revisit it over and over again. For more than 30 years, Will Latham has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 135 medical practices representing over 1,300 physicians. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at
For more than 30 years, Will Latham has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 135 medical practices representing over 1,300 physicians. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at  Anesthesiologists might entertain a range of reasons to market on social media, such as providing information about the practice, emergency closures, new employees or business accomplishments. They might also want to provide information about anesthesia, procedures and insurance. Anesthesiologists and anesthesia groups with aspirations of securing larger contracts, mergers and investments can utilize social media to build a brand.
Anesthesiologists might entertain a range of reasons to market on social media, such as providing information about the practice, emergency closures, new employees or business accomplishments. They might also want to provide information about anesthesia, procedures and insurance. Anesthesiologists and anesthesia groups with aspirations of securing larger contracts, mergers and investments can utilize social media to build a brand. Facebook is the most popular platform for patients to use for healthcare information. The next two most popular platforms for healthcare information are YouTube followed by Twitter. All three platforms are great for branding, but Facebook is seeing a decline in younger users. YouTube is seeing a steady increase in all users. Twitter is seeing instability, record losses and a questionable future.
Facebook is the most popular platform for patients to use for healthcare information. The next two most popular platforms for healthcare information are YouTube followed by Twitter. All three platforms are great for branding, but Facebook is seeing a decline in younger users. YouTube is seeing a steady increase in all users. Twitter is seeing instability, record losses and a questionable future. Kristine E. Squiers, MS manages all social media for MiraMed Global Services and its Family of Companies. Kristine began her digital marketing career in 2008, and has extensive experience in search engine optimization, digital advertising, website management, content marketing, lead generation and social media. Kristine has a Master of Science in Psychology with a specialization in Industrial and Organizational Psychology, as well as Graduate Certificates in Diversity Studies and Business Management.
Kristine E. Squiers, MS manages all social media for MiraMed Global Services and its Family of Companies. Kristine began her digital marketing career in 2008, and has extensive experience in search engine optimization, digital advertising, website management, content marketing, lead generation and social media. Kristine has a Master of Science in Psychology with a specialization in Industrial and Organizational Psychology, as well as Graduate Certificates in Diversity Studies and Business Management.