 You cannot manage what you cannot measure. This is today’s business mantra and no aspect of any serious business is exempt, from productivity of operations to quality of customer service. The goal is to use objective metrics to drive down cost and improve quality. Is it any wonder that the tools that are driving the management of business should be applied to medical and service specialties like anesthesia? Much as anesthesiologists and CRNAs may resist efforts to quantify their productivity and objectively assess the quality of care provided, this is becoming the new reality in medicine. To resist is to demonstrate one’s inflexibility and to invite alternative solutions. The largest and most aggressive players in the specialty are investing millions in the tools and technology of productivity and quality measurement. Whether this is ultimately good for the specialty is another question for another day.
From OR Utilization to Provider Productivity
The...
You cannot manage what you cannot measure. This is today’s business mantra and no aspect of any serious business is exempt, from productivity of operations to quality of customer service. The goal is to use objective metrics to drive down cost and improve quality. Is it any wonder that the tools that are driving the management of business should be applied to medical and service specialties like anesthesia? Much as anesthesiologists and CRNAs may resist efforts to quantify their productivity and objectively assess the quality of care provided, this is becoming the new reality in medicine. To resist is to demonstrate one’s inflexibility and to invite alternative solutions. The largest and most aggressive players in the specialty are investing millions in the tools and technology of productivity and quality measurement. Whether this is ultimately good for the specialty is another question for another day.
From OR Utilization to Provider Productivity
The...
10733 Hits
 Neda M. Ryan, Esq. Corporate Compliance Attorney, Anesthesia Business Consultants, Jackson, MI
Christopher J. Ryan, Esq. Giarmarco, Mullins & Horton, PC, Troy, MI
The number of self-pay patients continues to rise. The term “self-pay” used to apply primarily to the population of individuals who are uninsured; now, the term continues to expand to also represent the insured population with high deductible plans. Some in the community call self-pay “no pay” because collecting payment from these individuals can be extremely difficult. Unfortunately for healthcare providers, medical debts do not rise to the top of many consumers’ priority lists, especially if money is tight. They often fall behind items like mortgages, car payments and credit card bills. To address this situation there are two options: either eliminate self-pay patients from a practice altogether (which is not feasible for most anesthesiologists), or take the right steps early on to increase a practice’s likelihood of...
Neda M. Ryan, Esq. Corporate Compliance Attorney, Anesthesia Business Consultants, Jackson, MI
Christopher J. Ryan, Esq. Giarmarco, Mullins & Horton, PC, Troy, MI
The number of self-pay patients continues to rise. The term “self-pay” used to apply primarily to the population of individuals who are uninsured; now, the term continues to expand to also represent the insured population with high deductible plans. Some in the community call self-pay “no pay” because collecting payment from these individuals can be extremely difficult. Unfortunately for healthcare providers, medical debts do not rise to the top of many consumers’ priority lists, especially if money is tight. They often fall behind items like mortgages, car payments and credit card bills. To address this situation there are two options: either eliminate self-pay patients from a practice altogether (which is not feasible for most anesthesiologists), or take the right steps early on to increase a practice’s likelihood of...
4279 Hits
On July 6, 2015, as we advised readers in our Alert of July 20th, the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) jointly announced efforts to help physicians prepare for the October 1st changeover to ICD-10 diagnosis coding. The joint announcement indicated that or a full year from October 1, 2015, Medicare review contractors will not deny physician claims “based solely on the specificity of the ICD-10 diagnosis code as long as the physician/practitioner used a valid code from the right family.” Confronted with many requests for a clarification of what constitutes “a valid code from the right family,” CMS issued a longer set of Frequently Asked Questions (FAQs) on July 27, and then revised those FAQs again on July 31. The short answer is that a “valid” code is one consisting of three to seven characters but “a three-character code is to be used...
2672 Hits
 A review of recent activity by the Health and Human Services Office of Inspector General (OIG) indicates that it may be physicians’ turn for a higher level of scrutiny. Over the past few years, the OIG has released three Special Fraud Alerts focusing on physicians’ arrangements. In 2013, the OIG issued a fraud alert about physician-owned device distributorships, and in 2014 it issued a fraud alert about lab payments to physicians. The third alert, issued June 9, 2015, addresses physician compensation arrangements that may result in significant liability under the federal Anti-Kickback Statute (AKS).
One purpose of the AKS is to protect patients from inappropriate medical referrals or recommendations by healthcare professionals who may be unduly influenced by financial incentives. Section 1128B(b) of the Social Security Act (the Act) makes it a criminal offense to knowingly and willfully offer, pay, solicit or receive any remuneration to induce, or in return for,...
A review of recent activity by the Health and Human Services Office of Inspector General (OIG) indicates that it may be physicians’ turn for a higher level of scrutiny. Over the past few years, the OIG has released three Special Fraud Alerts focusing on physicians’ arrangements. In 2013, the OIG issued a fraud alert about physician-owned device distributorships, and in 2014 it issued a fraud alert about lab payments to physicians. The third alert, issued June 9, 2015, addresses physician compensation arrangements that may result in significant liability under the federal Anti-Kickback Statute (AKS).
One purpose of the AKS is to protect patients from inappropriate medical referrals or recommendations by healthcare professionals who may be unduly influenced by financial incentives. Section 1128B(b) of the Social Security Act (the Act) makes it a criminal offense to knowingly and willfully offer, pay, solicit or receive any remuneration to induce, or in return for,...
3937 Hits
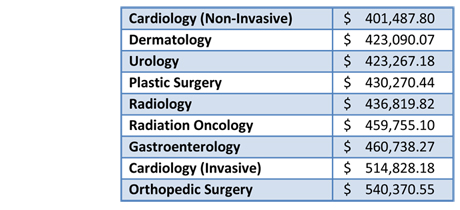 The amount of physician compensation is one of the key issues in every negotiation between anesthesiologists and anesthesiology groups and hospitals or health systems. What is the fair market value for an anesthesiologist? And how much do you have to offer to attract him or her? There is no definitive set of data, just a handful of surveys, some free and some for sale at hefty prices. Practices that are sufficiently large or that have a long history often realize that their own internal information may be the best available. In the interest of covering as many bases as possible and providing the greatest amount of data on which interested readers may perform their meta-analyses, we bring to your attention the latest public physician compensation information, released last week by Modern Healthcare in its Physician Compensation: 2015 report.
For 2015, Modern Healthcare reports an average salary for anesthesiologists of $384,290, which comes from...
The amount of physician compensation is one of the key issues in every negotiation between anesthesiologists and anesthesiology groups and hospitals or health systems. What is the fair market value for an anesthesiologist? And how much do you have to offer to attract him or her? There is no definitive set of data, just a handful of surveys, some free and some for sale at hefty prices. Practices that are sufficiently large or that have a long history often realize that their own internal information may be the best available. In the interest of covering as many bases as possible and providing the greatest amount of data on which interested readers may perform their meta-analyses, we bring to your attention the latest public physician compensation information, released last week by Modern Healthcare in its Physician Compensation: 2015 report.
For 2015, Modern Healthcare reports an average salary for anesthesiologists of $384,290, which comes from...
4851 Hits