eAlerts
-
Who Really Owns Your Anesthesia Group?
Mark F. Weiss, JD
The Mark F. Weiss Law Firm, Dallas, TX, Los Angeles and Santa Barbara, CA Walmart is famous for its slogan “Save Money. Live Better.”
Walmart is famous for its slogan “Save Money. Live Better.”It’s no surprise that the slogan is aimed at the customer.
But have you ever wondered about the supplier?
There is a tremendous analogy here for medical groups of all stripes and for anesthesiology groups in particular.
Lower Prices. Every Day.
From the inception of its business, Walmart employed a low-price strategy. And, it’s certainly no trade secret that the way Walmart sells at low prices is to buy at even lower prices—in fact, at the lowest prices.
To get those lowest prices, Walmart is willing, and quite able, to buy in very large quantities. And, therein lies the twist, the twist tie, if you will, for its suppliers, and, by analogy, you will see, for you.
Manufacturers, as they began selling to Walmart, craved the large distribution the chain offered. They’d assess how much Walmart would buy, and look at how many stores Walmart would put their product in. In order to get access to the Walmart business and the tremendous distribution, the manufacturers would then sell to Walmart at reduced prices— in fact, at their lowest prices.As a result of capturing Walmart’s business, many suppliers thought they had reached the promised land. Their sales shot up. Sure, margins on those sales were slim, but the quantities were stupendous. But that was just the start.
Once Walmart became a bigger and bigger and even biggest part of a supplier’s business, Walmart continued putting the pressure on. They knew that the supplier was so dependent upon Walmart for their huge volume and reach, that they could push even harder for really low prices, and then for really lower prices, and then for really lowest prices.
In a very real sense, far beyond the colloquial, many manufacturers became “owned” by Walmart. The twist ties that bound them to Walmart got tighter and tighter. Their margins were on a starvation diet, but quantities were super-sized. And, if they lost the giant chain’s distribution, the shock of the resulting excess capacity might pull them under.
Are You a Metaphorical Walmart Supplier?
If you’re the leader of an anesthesia group, it’s often much the same story. That is, if you’ve allowed your business to become dependent upon a single hospital or even a single system of hospitals.
If that’s the case, then who really owns your group? Is it really you and your partners? Or, in essence, does the hospital or the system “own” your group in the same way that Walmart “owns” the suppliers who’ve become dependent upon their business?At the extreme end of the continuum, if the hospital or system administrator were to tell you that they’ve decided that it’s in their best interest that, as of a month from next Tuesday, all anesthesia services will be provided by Best PowerPoint Anesthesia Group or through the anesthesia department of Nearby Giant University, so you’d better go cut employment deals, what other viable alternative would you have? Likely, none.
Short of that doomsday event (but one that happens more often than you might imagine), the same dynamic plays out whenever a hospital makes a demand on a dependent group. From “we’re cutting your stipend” to “we want you to expand coverage,” what choice do you have other than to say “yes”? The alternative, of course, whether spoken or understood, is that you’ll soon be an “ex-vendor.”
Should you attempt to sell your group, if you’ve become that dependent on one large source of business, what sort of a discount will the buyer demand due to your huge, “baked in” fragility?
The real question is, have you, in essence, given away the ownership of your practice entity by falling into the “Walmart” trap?
Do you and your fellow physician “owners” really own what you think you own?
Mark F. Weiss, JD is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He is also the co-founder of a healthcare mergers and acquisitions advisory firm, Steering Advisors. He can be reached by email at markweiss@advisorylawgroup.com or at markweiss@steeringadvisors.com. -
Coronavirus: A Game-Changing Event
Just when we thought we had seen it all and successfully managed innumerable practice management challenges, along comes a virus so insidious and so contagious that every aspect of the economy will be affected. Americans have been laid off in record numbers. Surgical case volumes have dropped precipitously. Once well-managed anesthesia practices are scrambling to cobble together a strategy for survival. As your business partners, we are exploring all options and will be updating you with our research and insights. This collection of articles is just a small sample of the wisdom of our eminently qualified industry experts.
Kate Hickner, Esq. discusses one of the most interesting policy developments to come out of this crisis: new guidelines for telemedicine. While it is not entirely clear how this will impact anesthesia providers, these new guidelines are sure to be a preview of coming developments. Clearly, treatment paradigms are going to change.
Will Latham draws our attention to the importance of group governance in a very interesting discussion of some of the most common governance problems groups face. He shares the insights of his years of experience managing all manner of practices. His piece consists of many very practical suggestions for today’s practices.
Mark Weiss, JD poses a very intriguing question: who really owns your anesthesia group? However valuable your contract at a given facility, he submits that, in many ways, groups have sold out to the facilities they serve. Is it any wonder that so many practices have decided to sell their practices? It is a very thought-provoking piece.
One of our ever-loyal contributors, Kelly Dennis, presents some interesting thoughts with regard to the potential of an audit and the specific requirements of medical direction. It is hard to imagine that payers will be turning to audits in the current environment and yet audits tend to peak when money is short. This is a timely reminder.
ABC’s own Kendall Lutz sheds some light on one of the most fundamental questions in anesthesia: is it better to be a generalist or a specialist? His piece on boutique anesthesia practices raises some interesting questions about the value of focusing on a niche or boutique market.Michael Bronson, MD of Mission Viejo Anesthesia Consultants and our own Jody Locke provide a fascinating profile of a ketamine clinic in southern California. This is a line of business that many practices are considering but few, as yet, are pursuing. We believe this is a very timely and relevant case study for your review.
Who knows how long the current crisis will last and what its lasting impact will be on the specialty of anesthesia. The rate of infection continues to rise and, despite government intervention, it is entirely unclear how most practices will survive the economic implications of the current environment. Just know that we are all in this together. Your success is our success.
With best wishes,
Tony Mira
President and CEO -
Governance Traps and Tricks
Will Latham, MBA, President
Latham Consulting Group, Inc., Chattanooga, TNIn today’s challenging times, effective group governance takes on even greater importance. If a group cannot develop plans, make decisions and implement its plans, someone else will choose the course of the group.
Following are some governance challenges that clients have approached us with over the last year.
Speed Bump
The Problem:
“Our group revisits issues over and over again. We have members of the group who, if they do not get their way in the first vote, raise the issue over and over again to either torture the group into changing the decision, or to paralyze the group.”The Solution:
One way to reduce the use of this “torture” technique is to implement a “speed bump” for items to return to the agenda for discussion.
For example, the group could implement a policy that requires 30 percent of the shareholders to sign a document asking to bring an item back to the floor for re-discussion once a decision has been made (it is important that they sign a document, rather than someone say “I had 30 percent of the people say they’d like to re-discuss this issue”).
This policy doesn’t close the door to re-discussing an issue (if more than 30 percent want to re-discuss an issue, the group probably should). However, it will typically reduce the number of times this “torture” technique is used.
Reduce Disruptive Behavior
The Problem:
“Our group has several disruptive physicians and we have not been able to deal with or even confront them. This job falls to the group leadership, and it’s the last thing they want to deal with. Even if they take on the disruptive physician, it is often an argument over who should decide what appropriate behavior should be.”
The Solution:
One way to address this situation is for the group to develop a “Code of Conduct.”A Code of Conduct indicates the agreed upon standards of behavior expected of a member of the group. It sets out, in general terms, the standards and duties which are reasonable to expect a member of the group to observe.
Properly developed, this document can be used to effectively reign in problematic physician behavior. Everyone has fair warning about what the agreed upon expectations are. Toleration for outliers is reduced. Group leadership can act because an intervention is no longer seen as one person’s opinion versus another’s.
We believe that the group should set expectations in a number of areas, to include:
- Relations/interactions between group physicians.
- Relations/interactions with group employees.
- Relations/interactions with those outside the group.
- Patients and patient care.
- Participation in practice management responsibilities.
- Confidentiality of practice information.
- Support of group decisions, established goals and policies.
For each area the group should answer the following questions:
- What behaviors do we expect of each other? What is acceptable to us?
- What is inappropriate?
- What are some of the “unwritten rules” that guide our behavior?
- What are the rights and responsibilities of each physician?
An example Code of Conduct can be found in Exhibit 1.
Use Committees to Share the Load
The Problem:
“Our Board is overloaded. Most of the shareholders are uninvolved, except to veto items or complain. We have committees, but they don’t function well.”
The Solution:
We have found that the best medical group Boards use their committees to process information prior to the Board addressing an item. When an item is raised at the Board level, their first step is often to send it to a committee to:
- Define the scope of the issue.
- Gather needed data.
- Analyze the data.
- Recommend a solution.
Once the committee has developed a solution or recommendation, this information should be presented to the Board. However, the Board must be extremely careful to not redo the work of the committee. If the Board feels the committee has not completed the assignment, it should be sent back to the committee for further work.In addition, the Board should make every effort to accept the committee’s recommendation. Why? If the Board always rejects the committees’ recommendations or re-does the work, the committees will reach the conclusion that their thoughts are not being considered and stop doing the work.
Conflict Avoidance and Voting
The Problem:
“Our meetings go on and on forever. Some group members keep talking and talking, while others sit in silence. And when we vote, people seem reluctant to raise their hand and express their true opinion.”
The Solution:
In our experience physicians tend to be conflict avoiders when it comes to their peers. Sometimes discussions go on and on because people don’t want to raise their hands to vote and possibly enter into conflict with those that don’t agree with them. This can make meetings last much longer than they need to.
To deal with conflict avoidance, we are seeing more and more groups move to using “secret ballots” for their voting process. Most groups use secret ballots for electing their Board and officers, but some groups use them when they need to vote on controversial issues, or in some cases, all issues.
Why are secret ballots useful?
- They allow the individuals to “vote their conscience” with less fear of retribution.
- They avoid one physician “bullying” another physician into changing their vote.
- They often speed up a meeting because people don’t delay voting to put off conflict.
There are several ways to implement secret ballots—here are two:
- Use 3 x 5 cards as the secret ballots.
- I have observed some groups starting to use “audience response systems.” Some of these are apps on smartphones while others utilize dedicated voting devices. A group we worked with recently moved to using such a voting system for all issues. They found that this has cut 25 - 50 percent off the time of every meeting by using secret ballot.
Authority
The Problem:
“We have created an Executive Committee of three physicians and given them significant authority. However, they will not make decisions within the bounds of their authority because they are afraid of second guessing by the other physicians. What can we do?”
The Solution:
There’s no doubt about it, serving as a leader in a physician group is a tough job. Decisions will be second-guessed, and some people will not like any decision that is made. Here are several suggestions:
- First, the leadership must recognize that criticism comes with the job—if they can’t take it or expect it not to exist, they should avoid serving as a leader.
- The leadership must help each other develop the mindset that it is their job to make these tough decisions, and then stick up for each other in front of the larger group.
- If the larger group continually second guesses the authority of the leadership, the group at large should re-discuss what level of authority they are truly willing to give the leadership.
- In some cases, leaders are afraid to make decisions because any decision can be recalled to the larger group for another vote by the members at large. Naturally, this defeats the purpose of a governance structure. For group’s with this problem, they should consider a provision that requires a two-thirds majority of the shareholders to even bring up for discussion an issue decided within the authority of the leadership.
Critical Time
These are unprecedented times for anesthesiology groups. The challenges are greater than ever, as is the need for effective group governance.
If your group suffers from any of the problems mentioned in this article, we suggest you seriously consider implementing the solutions offered. The anesthesiology groups that have implemented these ideas have found their ability to make decisions and move forward to be greatly strengthened.
For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at WLatham@LathamConsulting.com. -
Internal Audits: Process and Frequency
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I
Perfect Office Solutions, Inc., Leesburg, FLMany practices are too busy with day-to-day work to keep track of how often they should conduct internal audits. However, if your practice has a compliance plan, it generally outlines the required audit frequency. Do you know what your compliance plan requires?
If your anesthesiology practice is still using the compliance plan outline published in September 1997 by the American Society of Anesthesiologists™ in Compliance With Medicare and Other Payor Billing Requirements, your practice is required to review pre-submissions (claims reviewed before filing to the insurance carrier) on a quarterly basis, and post-submission (claims reviewed after filing to the insurance carrier) at regular intervals, such as semi-annually. You may also want to consider updating your compliance plan to ensure it meets current standards.How to Prepare for Audit
Having anesthesia records available as you start your internal audit will make the review process easier. If anesthesia records are not available, you should obtain them from the hospital’s medical records department.
An internal audit is simply an objective review of the anesthesia services billed to monitor the accuracy and suitability of claims. It should be performed by a qualified employee—such as the office administrator, manager, a certified coder (other than the employee who coded the services), the compliance officer, a physician or a combination of staff members.
Each practice determines the number of charges or percentage of claims to be reviewed for each provider. It also determines how to make appropriate corrections and, depending on the internal audit results and compliance plan requirements (when applicable), whether to contact legal counsel. Although the standard compliance plan requires the practice to discuss all claims monitoring with legal counsel, the practice may modify the plan to require legal counsel consultation only during external audits.
A simple pre-submission review should compare the codes and modifiers billed with the documentation on file. Because the auditor reviews this information before submitting the claim, corrections are made during the review process, and corrective actions are taken and conveyed to staff. For example, a review determined the coder mistook “TKA” for a total knee arthroscopy (01400, base value - 4), rather than a total knee arthroplasty (01402, base value - 7). The practice must take several corrective steps:
- Change code, if applicable. Make certain what procedure was performed as different clinical staff may be using different acronyms;
- Ensure acronyms in your practice are clearly defined; and
- Request a report of 01400 and 01402 claims filed to verify accuracy. Choose your time frame based on payer policy and timely filing requirements, such as one year or 90 days.
A post-submission review is more complex and should include a review from the time the claim is entered all the way through resolution. Choose a date within the past six months; and, in addition to checking codes and modifiers used, review payment processes to ensure correct payments were received and appropriate adjustments were taken. Each practice should know exactly what payment to expect from each payer. Medicare pays by location and the amount is standard; other payers may be contracted using various amounts and time calculation techniques, so a matrix of expected reimbursement is helpful. At the very least, a form listing annual expected amounts is necessary.
Payment will be made at the medically directed rate if the physician medically directs qualified individuals (all of whom could be CRNAs, anesthesiologists’ assistants, interns, residents or combinations of these individuals) in two, three, or four concurrent cases and the physician performs the following activities.
The physician must document in the medical record that he or she performed the pre-anesthetic examination and evaluation. Physicians must also document that they provided indicated post-anesthesia care, were present during some portion of the anesthesia monitoring and were present during the most demanding procedures in the anesthesia plan, including induction and emergence, where indicated. (Source: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf)
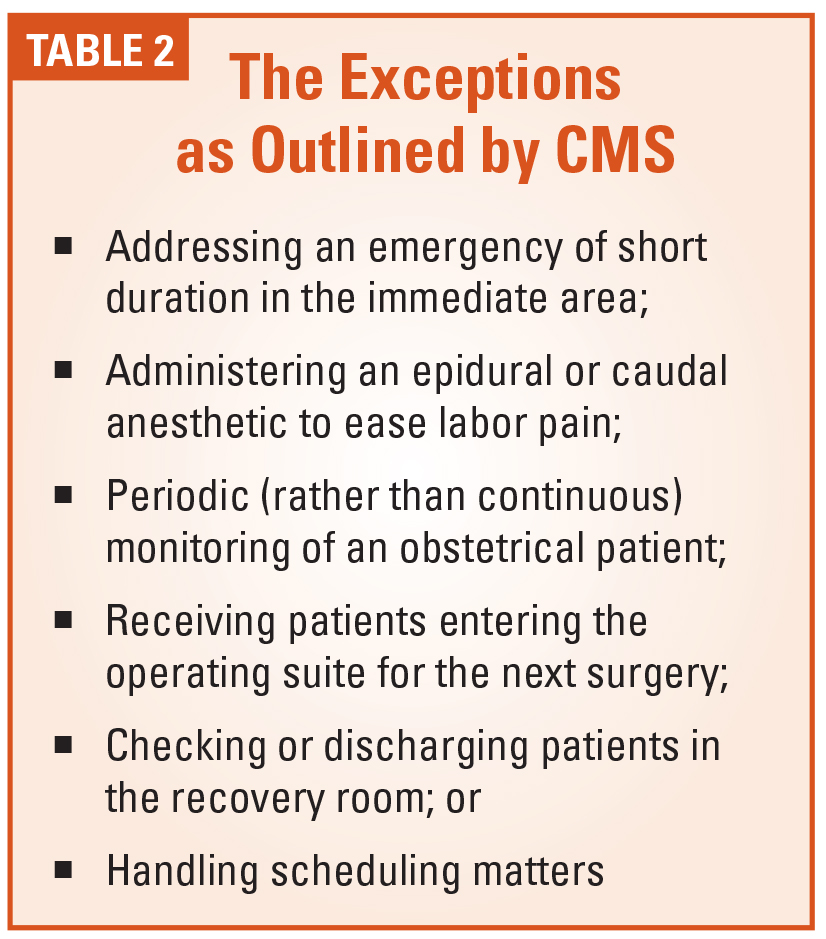
An important area to review is concurrency and documentation of medical direction criteria. (See Tables 1 and 2). Depending on the software concurrency reporting capabilities, it may be necessary to review an entire day of concurrency if your practice includes residents, certified registered nurse anesthetists, anesthesia assistants or student registered nurse anesthetists. It is important to understand that concurrency calculations must include all patients, regardless of type of insurance. While some carriers allow a combination of up to four concurrent cases, graduate medical rules differ and allow up to two cases when residents or SRNAs are involved.
A physician who is concurrently furnishing services that meet the requirements for payment at the medically directed rate cannot ordinarily be involved in furnishing additional services to other patients. Nevertheless, engaging in activities described in Table 2 do not substantially diminish the scope of control exercised by the physician and do not constitute a separate service for the purpose of determining whether the requirements for payment at the medically directed rate are met.(Source: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf)
Whether conducting a pre- or postsubmission review, keep documentation of all steps taken in a compliance file. Even if your practice only reviews once a year, make certain the time frame agrees with the written compliance plan, when applicable. The adage, “It is better not to have a compliance plan, than to have one and not follow it,” is particularly true for anesthesia practices, as anesthesia billing rules are often vague and ambiguous.
Note: Novitas and other Medicare Administrative Contractors may allow additional exceptions. For example, Novitas indicates “An anesthesiologist may perform and, if otherwise eligible, seek reimbursement for procedures (such as arterial line insertions, central venous catheter insertions, pulmonary artery catheter insertions, and epidural, spinal, and peripheral nerve blocks) performed in an area immediately available to the operating room when performance of such services does not prevent him/her from being immediately available to respond to the needs of surgical patients.”
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I, has over 36 years of experience in anesthesia coding and billing and speaks about anesthesia issues nationally. She has a Masters Degree in Business Administration, is a certified coder and instructor through the American Academy of Professional Coders. Kelly is an Advanced Coding Specialist through the Board of Medical Specialty Coding and served as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November 2001. She can be reached at kellyddennis@attglobal.net. -
Profile of an Anesthesia Ketamine Clinic
Michael Bronson, MD
Co-founder and Chief Executive Officer, Wellness Clinic of Orange County, Laguna Beach, CAJody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services, Anesthesia Business Consultants, LLC, Jackson, MIKetamine as a Treatment Modality for Depression
Ketamine has been well known to anesthesia providers for years. As an anesthetic agent it has been used mainly for starting and maintaining anesthesia. It induces a trance-like state while providing pain relief, sedation and memory loss. The active ingredient is similar to that in LSD. More recently its value is coming to be appreciated as an effective treatment for depression.While the treatment of depression has traditionally been the purview of psychiatry, the use of ketamine as a treatment modality has now attracted the attention of anesthesia providers who have become quite familiar with its pharmacological properties. The administration of drug infusions is a standard practice in the treatment of surgical patients. Given anesthesia provider experience in the administration of such powerful agents, the migration from the operating room to the clinic is a slight difference of degree, but not of kind.
The typical ketamine clinic patient receives an initial 60-minute infusion. They are placed into comfortable reclining chairs and may be given headphones and an eye mask. Vital signs are monitored as they would be for a surgical patient. About 15 minutes into the infusion, patients start to experience euphoria-heightened perceptions and a floating or dream-like state. Usually these symptoms resolve within 15 minutes after the completion of the infusion.
After a second session the patient should be experiencing significant mood elevation and pain relief. If the patient reports improvement, up to four subsequent sessions will be scheduled. If they are not responding, then they are considered a ”non-responder,” and they are referred back to the referring physician.
Following a successful treatment series of up to six sessions, they may return in two to four month intervals for a booster infusion. The advantages of ketamine infusion in the treatment of depression and mood disorders can be significant. Ketamine does not lead to addiction and most patients report positive results. A range of 70 to 80 percent of patients report significant improvement.
Should an Anesthesia Practice Consider a Ketamine Clinic?
The history of the Ketamine Wellness Clinic of Orange County (www.ketamineoc.com) provides an interesting and relevant case study. As is true in evaluating any new business ventures, there are many considerations. One thing is clear though: any new venture requires a champion with a clear vision and a supportive team of stakeholders. Mission Viejo Anesthesia Consultants in Mission Viejo, California has consistently distinguished itself as an organization open to exploring business options that are consistent with the mission and values of the practice.The clinic was founded in 2016 after a thorough review of current scientific and clinical studies. During the 1990s, clinical research clearly suggested a role for N-methyl-D-aspartate receptor (NMDA) antagonists in the treatment of depression. In the early 2000s, the first double-blinded, placebo-controlled studies that gave patients ketamine and followed their results showed rapid and significant improvement in symptomology after a single dose of ketamine. Subsequent studies reproduced the same results and demonstrated that multiple infusions of ketamine lead to more long-term results. As the investigation of ketamine expanded, it was found to be an effective treatment for other mood disorders and chronic pain.
An initial team of group members carefully reviewed the research available to develop the basic elements necessary to start the clinic: flow charts, clinical protocols, clinic notes, consents referral forms and a website. The clinic remains a work in progress and all aspects of the operation are constantly being refined to optimize the patient experience and the consistency of positive outcomes. Since 2016, the clinic has provided services to over 500 patients who have received thousands of infusions. The current team of providers consists of anesthesiologists, behavioral health nurses and various support staff.
Initially the clinic was set up in a large room at the hospital with only a curtain to provide privacy to patients. That initial venue was staffed by a single physician and nurse. Since 2016, the clinic has grown significantly. The current location is a six-room office-based facility that is not affiliated with the hospital. This has required some investment on the part of shareholders, but this has allowed the clinic to realize its market potential.
How the Clinic Works
All patients must be referred by a treating physician to come to the Ketamine Wellness Clinic of Orange County. The referring physician provides comments on prior medications and/or interventions to ensure ketamine is an appropriate next step in therapy. The clinic also use this interaction to establish a relationship with the referring provider, as they consider themselves one part of a collaborative team to treat each patient. All potential patients are then screened by an anesthesiologist for medical appropriateness and any contraindications to ketamine therapy. Contraindications to ketamine therapy include uncontrolled blood pressure, unstable heart disease, intracranial mass or acute psychotic hallucinations.
Patients are given a scale to fill out prior to initiation of ketamine therapy to establish an objective baseline. They then complete the same scale at the end of the series to gauge response to treatment. Most patients are able to realize a 50 percent reduction in their baseline scale by the end of the treatment. These results are also communicated to their referring physician to “close the loop.” At this point, some patients are then able to work with their treating physician to decrease or eliminate some of the chronic medications they were taking before the ketamine therapy. The clinic also tracks these scales with a database which is used to run statistics to help fine-tune protocols. It is typical to fluctuate between a 70-80 percent response rate to infusions.
The Economics of a Ketamine Clinic
While the management of an office-based practice providing infusion therapy is similar to the management of an anesthesia practice, in some ways it is quite different. In both cases the volume of services provided and the ability to get paid for those services are essential keys to success. Perhaps the biggest difference, however, is that the anesthesia practice is captive to the facilities it serves for surgical case volume and payer mix while the clinic-based practice has much greater potential to control and manage both volume and sources of payment. It should also be noted that physicians will typically manage up to six infusions concurrently, which is similar to the management of multiple labor patients in the OB suite.
It is the number of variables that have to be managed that can make a clinic practice riskier. The goal must be to manage the business as efficiently as possible. Management and financial reporting must be specifically tailored to the unique nature of the services being provided. Payer rules for infusion therapy are quite different than those pertaining to payment for surgical and obstetric anesthesia. Contracting with insurance is not necessarily the best strategy for a ketamine clinic. While it is true that patients are expected to pay at time of service, many can also submit claims to their insurance that may reimburse them for the monies they have paid.
One of the complicating factors is the coding of infusions. In the office setting (POS 11), there is a code for intravenous infusion: 96365. This applies to intravenous infusion, for therapy, prophylaxis or diagnosis; initial, up to 1 hour. Code 96366 should be added for each additional hour. These codes are not applicable in the facility setting (POS 22, 24, etc.) where a E/M visit code must be used. Based upon the face-to-face time documented, it is suggested to use 99354 for prolonged evaluation and management or psychotherapy service(s) (beyond the typical service time of the primary procedure) in the office or other outpatient setting requiring direct patient contact beyond the usual service; first hour (list separately in addition to code for office or other outpatient evaluation and management or psychotherapy service).Many insurance plans do pay for the infusion codes, excluding the VA, depending on the patient’s benefit level. The clinic has not seen an unusual percentage of denials for these services, although in some markets pre-authorization may be required. In the case of this clinic, the practice chooses to bill patients first as a matter of expediency.
The Value of a Ketamine Clinic
As anesthesia practices explore alternative lines of business, should they be investigating a ketamine clinic? The answer is yes, but there are a number of critical criteria that should be met first.
- Is there a market for infusion therapy in your area? Ideally, the practice should be providing a service that is not otherwise available in the immediate area. Some market research will be necessary to determine this.
- Is this a buy or make decision? In other words, does the practice wish to develop a clinic from scratch or become affiliated with an existing clinic practice? Affiliating with an existing and established practice minimizes some of the start-up challenges, but may diminish some of the potential returns.
- Are existing providers interested in providing such a service? Without willing and available providers such an enterprise cannot be undertaken.
- Is there a champion for the service? A member of the group or a small group of members needs to take ownership of the enterprise. This person needs to research the options and orchestrate the project. This could be an opportunity for a younger member of the group to exercise leadership.
- What is the practice’s tolerance for risk? Is it willing to make an investment and live with the consequences?
- What are the business objectives for the venture and how will they be measured? Any new venture should contribute to the value of the practice. This value is either financial or strategic. There needs to be accountability and transparency for the venture to be successful.
Anesthesia practices in the current environment need to be exploring ways to expand and diversify their practices. Options are limited, but they do exist. Although it is easy to get paid for ketamine infusions in the right market—patients simply scan their credit cards and start treatment—getting payment from insurance can be tricky. This is why it is so important to establish a fee schedule that is appropriate to the market and the patient population. Mission Viejo is a particularly affluent area; nevertheless, there is obviously a need for the service. A properly managed clinic should have great potential in almost any market.
Michael Bronson, MD is co-founder and Chief Executive Officer of Wellness Clinic of Orange County which operates the Ketamine Wellness Clinic of Orange County. Mr. Bronson joined Mission Viejo Anesthesia Consultants (MAC) in 2013 after completing residency at UC San Diego where he served as Chief Resident. Bronson currently sits on the MAC Board of Directors, Mission Hospital Medical Executive Committee and function as the OR Director of Orthopedic and Neurosurgical services. Current projects include designing the infrastructure for a hybrid physical and virtual preoperative clinic as well as developing software to automate the daily anesthesia assignments. He can be reached at michaelpbronson@gmail.com. Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.
 Walmart is famous for its slogan “Save Money. Live Better.”
Walmart is famous for its slogan “Save Money. Live Better.” Manufacturers, as they began selling to Walmart, craved the large distribution the chain offered. They’d assess how much Walmart would buy, and look at how many stores Walmart would put their product in. In order to get access to the Walmart business and the tremendous distribution, the manufacturers would then sell to Walmart at reduced prices— in fact, at their lowest prices.
Manufacturers, as they began selling to Walmart, craved the large distribution the chain offered. They’d assess how much Walmart would buy, and look at how many stores Walmart would put their product in. In order to get access to the Walmart business and the tremendous distribution, the manufacturers would then sell to Walmart at reduced prices— in fact, at their lowest prices. If that’s the case, then who really owns your group? Is it really you and your partners? Or, in essence, does the hospital or the system “own” your group in the same way that Walmart “owns” the suppliers who’ve become dependent upon their business?
If that’s the case, then who really owns your group? Is it really you and your partners? Or, in essence, does the hospital or the system “own” your group in the same way that Walmart “owns” the suppliers who’ve become dependent upon their business? Mark F. Weiss, JD is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He is also the co-founder of a healthcare mergers and acquisitions advisory firm, Steering Advisors. He can be reached by email at
Mark F. Weiss, JD is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He is also the co-founder of a healthcare mergers and acquisitions advisory firm, Steering Advisors. He can be reached by email at  ABC’s own Kendall Lutz sheds some light on one of the most fundamental questions in anesthesia: is it better to be a generalist or a specialist? His piece on boutique anesthesia practices raises some interesting questions about the value of focusing on a niche or boutique market.
ABC’s own Kendall Lutz sheds some light on one of the most fundamental questions in anesthesia: is it better to be a generalist or a specialist? His piece on boutique anesthesia practices raises some interesting questions about the value of focusing on a niche or boutique market. “Our group revisits issues over and over again. We have members of the group who, if they do not get their way in the first vote, raise the issue over and over again to either torture the group into changing the decision, or to paralyze the group.”
“Our group revisits issues over and over again. We have members of the group who, if they do not get their way in the first vote, raise the issue over and over again to either torture the group into changing the decision, or to paralyze the group.” One way to address this situation is for the group to develop a “Code of Conduct.”
One way to address this situation is for the group to develop a “Code of Conduct.”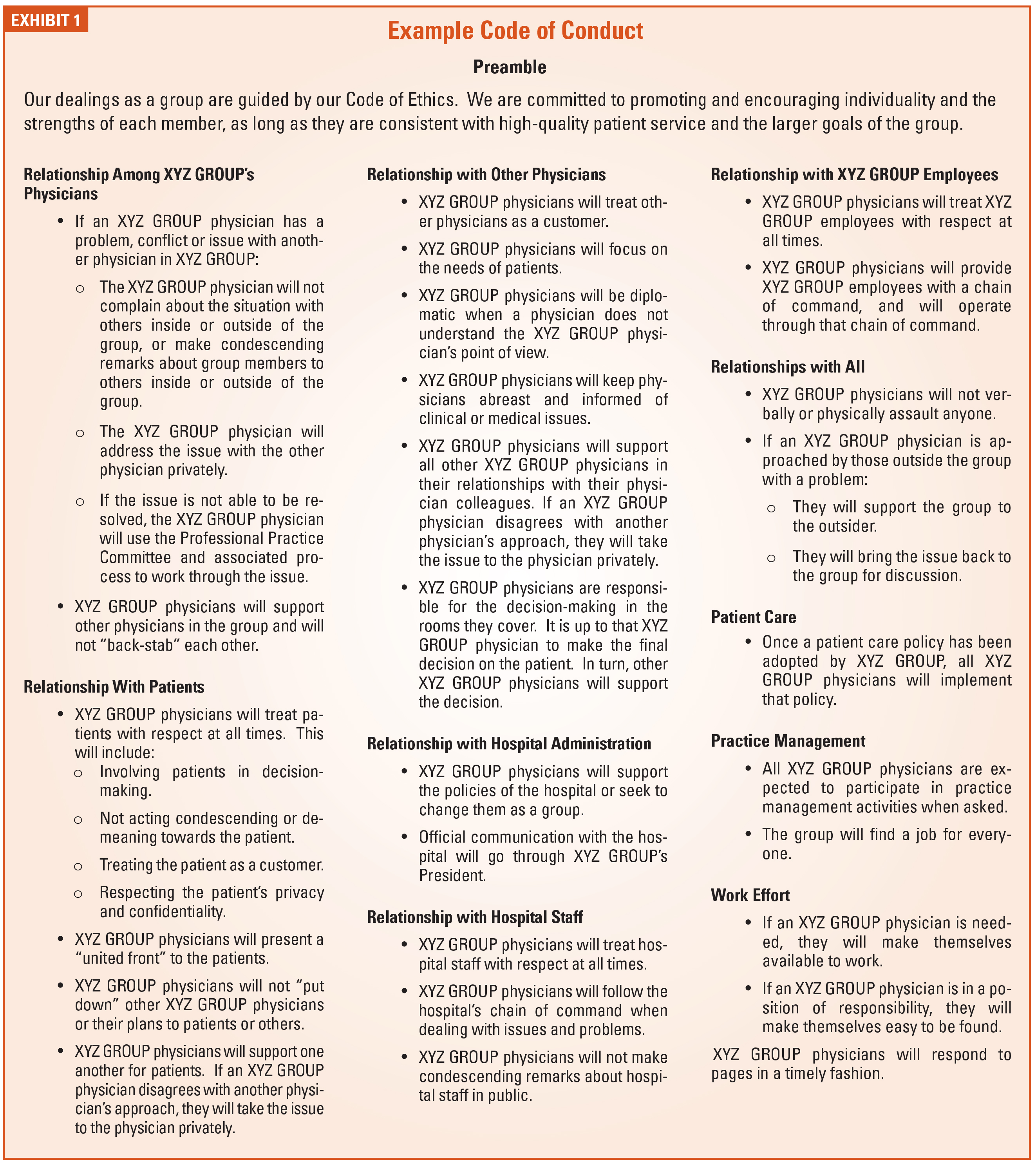
 Once the committee has developed a solution or recommendation, this information should be presented to the Board. However, the Board must be extremely careful to not redo the work of the committee. If the Board feels the committee has not completed the assignment, it should be sent back to the committee for further work.
Once the committee has developed a solution or recommendation, this information should be presented to the Board. However, the Board must be extremely careful to not redo the work of the committee. If the Board feels the committee has not completed the assignment, it should be sent back to the committee for further work.
 For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at
For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at  If your anesthesiology practice is still using the compliance plan outline published in September 1997 by the American Society of Anesthesiologists™ in Compliance With Medicare and Other Payor Billing Requirements, your practice is required to review pre-submissions (claims reviewed before filing to the insurance carrier) on a quarterly basis, and post-submission (claims reviewed after filing to the insurance carrier) at regular intervals, such as semi-annually. You may also want to consider updating your compliance plan to ensure it meets current standards.
If your anesthesiology practice is still using the compliance plan outline published in September 1997 by the American Society of Anesthesiologists™ in Compliance With Medicare and Other Payor Billing Requirements, your practice is required to review pre-submissions (claims reviewed before filing to the insurance carrier) on a quarterly basis, and post-submission (claims reviewed after filing to the insurance carrier) at regular intervals, such as semi-annually. You may also want to consider updating your compliance plan to ensure it meets current standards.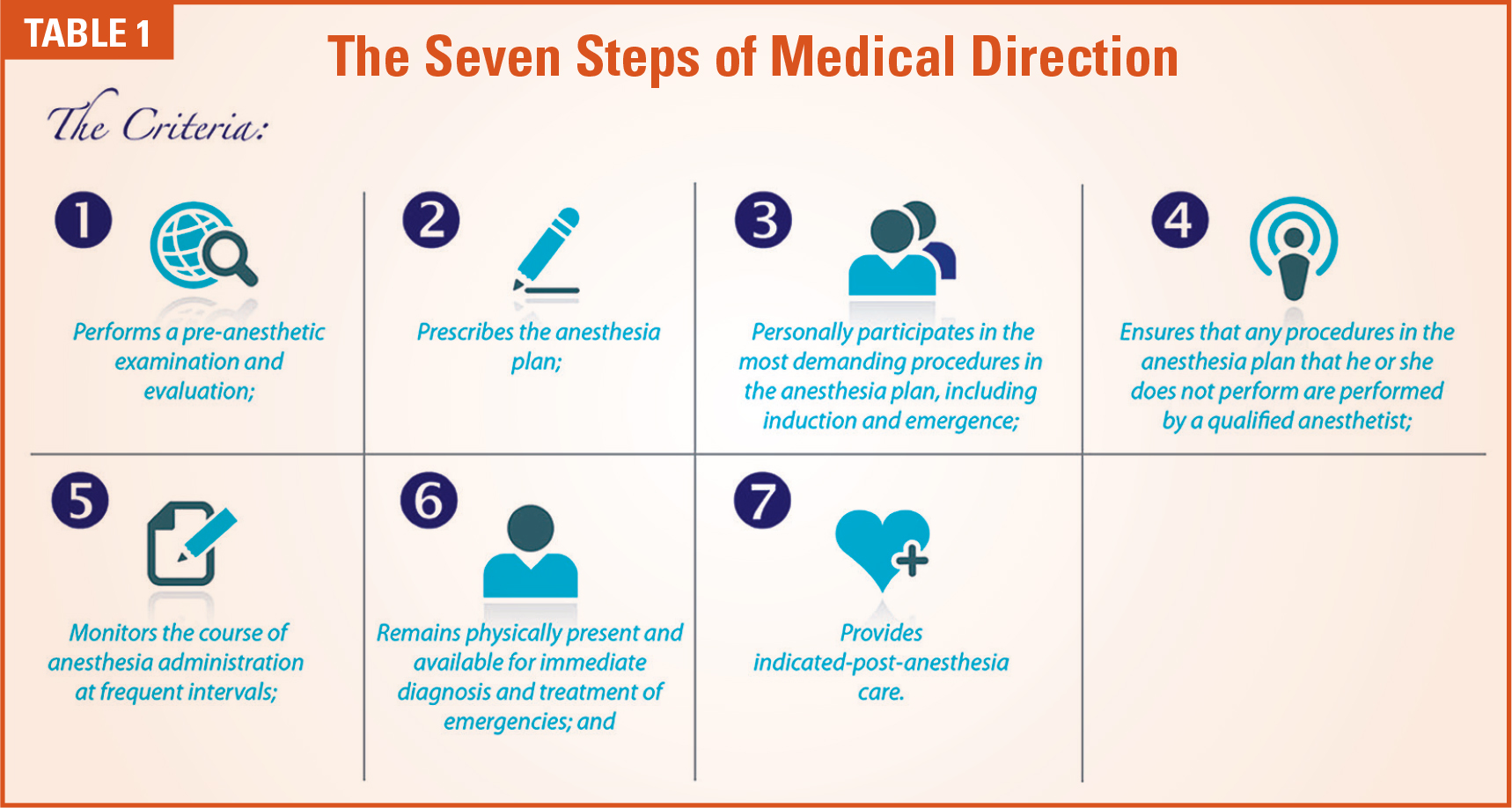
 Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I, has over 36 years of experience in anesthesia coding and billing and speaks about anesthesia issues nationally. She has a Masters Degree in Business Administration, is a certified coder and instructor through the American Academy of Professional Coders. Kelly is an Advanced Coding Specialist through the Board of Medical Specialty Coding and served as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November 2001. She can be reached at
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I, has over 36 years of experience in anesthesia coding and billing and speaks about anesthesia issues nationally. She has a Masters Degree in Business Administration, is a certified coder and instructor through the American Academy of Professional Coders. Kelly is an Advanced Coding Specialist through the Board of Medical Specialty Coding and served as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November 2001. She can be reached at  Ketamine has been well known to anesthesia providers for years. As an anesthetic agent it has been used mainly for starting and maintaining anesthesia. It induces a trance-like state while providing pain relief, sedation and memory loss. The active ingredient is similar to that in LSD. More recently its value is coming to be appreciated as an effective treatment for depression.
Ketamine has been well known to anesthesia providers for years. As an anesthetic agent it has been used mainly for starting and maintaining anesthesia. It induces a trance-like state while providing pain relief, sedation and memory loss. The active ingredient is similar to that in LSD. More recently its value is coming to be appreciated as an effective treatment for depression. The history of the Ketamine Wellness Clinic of Orange County (
The history of the Ketamine Wellness Clinic of Orange County ( One of the complicating factors is the coding of infusions. In the office setting (POS 11), there is a code for intravenous infusion: 96365. This applies to intravenous infusion, for therapy, prophylaxis or diagnosis; initial, up to 1 hour. Code 96366 should be added for each additional hour. These codes are not applicable in the facility setting (POS 22, 24, etc.) where a E/M visit code must be used. Based upon the face-to-face time documented, it is suggested to use 99354 for prolonged evaluation and management or psychotherapy service(s) (beyond the typical service time of the primary procedure) in the office or other outpatient setting requiring direct patient contact beyond the usual service; first hour (list separately in addition to code for office or other outpatient evaluation and management or psychotherapy service).
One of the complicating factors is the coding of infusions. In the office setting (POS 11), there is a code for intravenous infusion: 96365. This applies to intravenous infusion, for therapy, prophylaxis or diagnosis; initial, up to 1 hour. Code 96366 should be added for each additional hour. These codes are not applicable in the facility setting (POS 22, 24, etc.) where a E/M visit code must be used. Based upon the face-to-face time documented, it is suggested to use 99354 for prolonged evaluation and management or psychotherapy service(s) (beyond the typical service time of the primary procedure) in the office or other outpatient setting requiring direct patient contact beyond the usual service; first hour (list separately in addition to code for office or other outpatient evaluation and management or psychotherapy service). Michael Bronson, MD is co-founder and Chief Executive Officer of Wellness Clinic of Orange County which operates the Ketamine Wellness Clinic of Orange County. Mr. Bronson joined Mission Viejo Anesthesia Consultants (MAC) in 2013 after completing residency at UC San Diego where he served as Chief Resident. Bronson currently sits on the MAC Board of Directors, Mission Hospital Medical Executive Committee and function as the OR Director of Orthopedic and Neurosurgical services. Current projects include designing the infrastructure for a hybrid physical and virtual preoperative clinic as well as developing software to automate the daily anesthesia assignments. He can be reached at
Michael Bronson, MD is co-founder and Chief Executive Officer of Wellness Clinic of Orange County which operates the Ketamine Wellness Clinic of Orange County. Mr. Bronson joined Mission Viejo Anesthesia Consultants (MAC) in 2013 after completing residency at UC San Diego where he served as Chief Resident. Bronson currently sits on the MAC Board of Directors, Mission Hospital Medical Executive Committee and function as the OR Director of Orthopedic and Neurosurgical services. Current projects include designing the infrastructure for a hybrid physical and virtual preoperative clinic as well as developing software to automate the daily anesthesia assignments. He can be reached at  Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management
Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management