eAlerts
-
What Determines the Cost of Anesthesia Care?
Jody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services Anesthesia Business Consultants, LLC, Jackson, MI The cost of anesthesia care has become one of the most significant issues in the management of today’s anesthesia practices. This is not to say that quality of care is not important, but it has become a given. Ultimately the essential challenge facing virtually all practices is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the needs of the facility or facilities being served. The problem is that the options for generating more revenue are limited to three: enhancing fee-for-service collections; generating additional revenue from new services, such as nerve blocks and ultrasonic guidance for postop pain management; and negotiating subsidy support from the facility. None of these constitutes a quick or definitive fix.
The cost of anesthesia care has become one of the most significant issues in the management of today’s anesthesia practices. This is not to say that quality of care is not important, but it has become a given. Ultimately the essential challenge facing virtually all practices is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the needs of the facility or facilities being served. The problem is that the options for generating more revenue are limited to three: enhancing fee-for-service collections; generating additional revenue from new services, such as nerve blocks and ultrasonic guidance for postop pain management; and negotiating subsidy support from the facility. None of these constitutes a quick or definitive fix.The largest expense for any practice is the cost of providers. The most obvious way to reduce the cost of care is to either reduce the number of providers needed or modify the staffing model. Physician-only practices may want to consider bringing on CRNAs. Care-team practices may want to consider increasing the number of CRNAs. Although changing the configuration of the team might appear simple, especially to those hospital administrators who don’t want to increase the stipend, there are many considerations that must be carefully weighed. Reducing the number of one category of provider in order to increase the number of another can be very disruptive and become the anesthesia equivalent of voting members off the island. Such adjustments to the staffing model really only work when they are implemented over time, based on attrition.
Practical and logistical considerations aside, how should one evaluate the impact of a given staffing model? What is the appropriate metric? How should it be calculated? What is a reasonable benchmark? Since one cannot manage what one cannot measure, the logical place to start is with a calculation of cost. To be useful this must represent a normalized metric, such as cost per anesthetizing location day.
Suppose the coverage requirement consists of seven locations (four ORs, two Endo rooms and one OB), Monday through Friday, and three on the weekend (an elective room on Saturday, plus one call person each night). Given the current environment, there are three basic staffing options: a physician-only model; a traditional medical direction model, with one physician medically directing three CRNAs; and a non-medical direction model, where one physician may oversee five or six CRNAs—a model that is becoming more common in the 17 opt-out states. The financial implications of each model are summarized in the three tables below. It should be noted that in any particular practice scenario there may be multiple variables that could change the outcome. A physician cost of $475,000 may be high in some markets and low in others. Similarly, CRNA compensation varies considerably across the country. Staffing models may also vary. Obviously, the more providers that are required, the higher the cost per provider day will be. A number of factors determine the staffing model, but historical precedent is often the most significant. Changes in staffing model occur most often when a contract changes hands and a new staffing entity proposes a new staffing model.
In any pro forma model the assumptions are critical and can have a significant impact on the result of the calculations. This model assumes a small community hospital where some of the ORs may run late but where the average room runs about eight hours. OB is unpredictable but tends not to be very busy.The key to the validity of any analytical model is the reasonableness of the assumptions. The models presented below make some simple and generic assumptions for purposes of demonstrating the dramatic impact staffing changes can have on a practice but the reality of any specific practice analysis, especially those that are larger, and especially those that cover a variety of venue types, can be far more complex.
The Physician-Only Model
The first question is what is the optimum number of providers? The typical full-time anesthesiologist now gets an average of eight weeks of vacation. Thus, they are available for 215 days per year (365 minus 104 weekend days, 40 vacation days and 6 holidays). There are two ways to calculate the number of physicians needed: the simple method is based on the number of provider days needed divided by 215. A more refined model is based on hours of coverage divided by 21,500 or 10 hours per day. Most claim they work at least fifty hours per week, although this may not adequately allow for the impact of call. CRNAS, by contrast, typically get six weeks of vacation and work five eight-hour shifts, or a total of 40 hours per week.
The physician-only model (Table 1) is based on this calculation and an assumption that the average total compensation package, which includes the cost of malpractice and benefits, is probably about $500,000 nationwide at the current time. This is what groups need to offer to recruit and retain qualified providers. As the calculations indicate, a physician-only practice is a very expensive model. To support this staffing model, the providers would need to consistently generate 60 billable units a day at a net yield of $40 per unit, which is well beyond what most anesthesiologists actually generate. A shortfall would necessitate the need for financial support from the facility, and very few are willing to subsidize a physician- only staffing model.
The Medical Direction Model
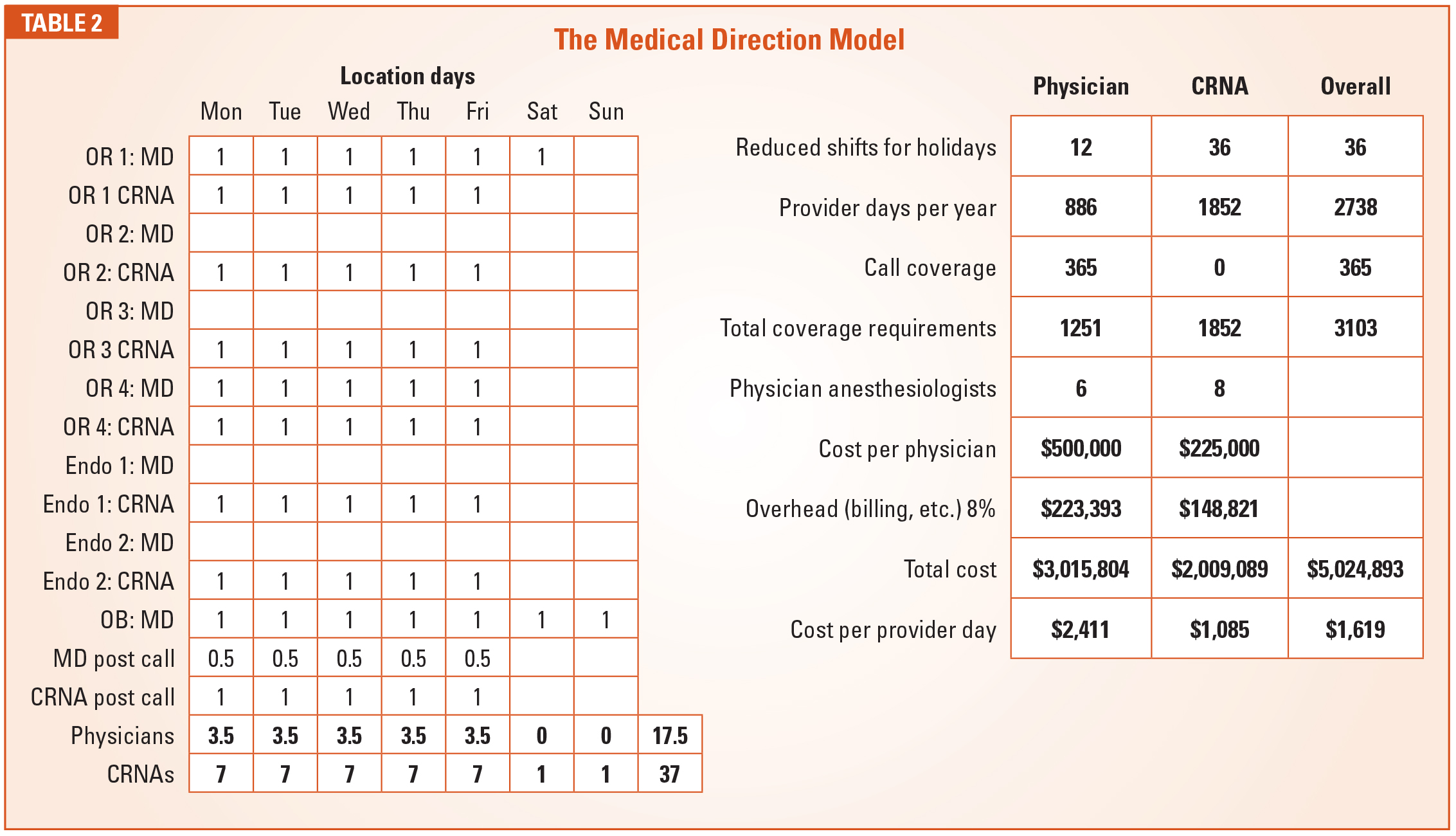
There are some ways to reduce the cost of care for a physician-only model. Including non-shareholder providers who get paid at a lower rate may help some. The use of independent contractors who only have to be paid when they work may also be helpful.At least 75 percent of all anesthesia care provided in the United States is administered by CRNAs, and the majority of these are medically directed by physicians. Traditional medical direction guidelines limit the number of CRNAs a physician anesthesiologist may manage at any point in time to four. As a practical matter, most medically directing anesthesiologists routinely oversee between two and three CRNAs at a time. The more a physician’s time is leveraged, the more cost-effective the model; but practical and logistical considerations are usually the rate-limiting factor.
The model (Table 2) assumes two physicians medically directing six CRNAs in the ORs and the endoscopy units, and one working alone in Obstetrics. The table lays out the proposed coverage pattern and the calculation of the number of providers needed. What this shows is that the use of CRNAs allows for an offset to the daily cost of a physician. The CRNA cost of $1,085 dramatically impacts the overall cost per anesthetizing location day from $2,411 to $1,619 or an overall cost savings of $1,417,433.
A Caveat
There are two primary reasons why care-team practices may not realize the savings indicated above. First, they may have too many physicians, meaning that the cost of each physician is not offset appropriately by the cost of the CRNAs. Second, they may have too many one-to-one or one-to-two scenarios. The real cost savings is only realized at levels of one MD to three CRNAs.
With the introduction of the concept of opt-out states we now see a third model: the physician oversight model. Since CRNAs in opt-out states no longer need to be medically directed, an increasing number of practices, especially in the West, are allowing CRNAs to work independently with minimal physician oversight and no strict medical direction. This allows for the reduction of the number of physicians in the model.
The Physician Oversight Model
As the data (Table 3) demonstrates, modification of the staffing model can have a dramatic and meaningful impact on the cost of anesthesia care. It explains why hospital administrators who are negotiating with physician-only practices always ask first if the practice has considered a CRNA option. Sometimes, the CRNA approach will save money, but sometimes it is simply not applicable to the type of care required or consistent with the culture of the institution. This is when practices have to start thinking outside the box and look for other ways to reinvent their group configuration and financial model.
The most common problem is that coverage requirements have outstripped the revenue potential of the practice. Hospitals tend to see availability to surgeons, which is an expensive commodity for the anesthesia practice that incurs the cost of a provider every time a room is opened whether or not the room is productive. Let’s pick a number, say 50 ASA units per location day. Suppose the hospital minimizes the number of rooms that do not meet this target. If minimizing the number of unproductive rooms allows for a reduction in anesthesia staffing, the result could be significant.
We often say that the anesthesia department has more and better data about what happens in the operating rooms each day than any other department in the hospital. The question is whether the practice is using this data effectively to help the administration run the operating rooms more efficiently. This is becoming one of the new frontiers for the specialty. Sharing operating room utilization data is not going to be a quick fix to under-utilization, but its value cannot be ignored. Anesthesia providers need to be seen as team players in the management of the operating rooms and delivery suites. The more active a role they play, the more it will ultimately benefit their practice. This is the kind of out-of-the-box thinking that anesthesia practices should be pursuing as the cost of care becomes an ever more important factor in determining where patients get directed for the procedures they need.
Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com. -
Anesthesia Tips for the New Decade
I am happy to share with you another issue of our quarterly Communiqué. As in the past, we have compiled a most interesting collection of authors and topics. These are challenging times for anesthesia practices across the country, and who knows what the new year will bring?
We begin with a very thoughtful piece by Mark Weiss, JD about the impact of the company model. His article, New Cases, New Tools in the Fight Against the “Company Model” Kickback Scheme, is just one more example of how non-anesthesia practices try to profit from their relationship with their anesthesia provider. It is a critical topic, and Mark’s piece is particularly insightful.
Our own Jody Locke penned the second article, What Determines the Cost of Anesthesia Care?, which examines a critical component of today’s anesthesia practice. Increasingly, cost has become the key determinant in hospital contract negotiations. Obviously every situation is unique, but there are some good templates here for your consideration.
Returning author, Will Latham, offers some very practical ideas for strategic planning in Chaos to Clarity: Resolving Strategic Issues. Will brings such a vast body of experience in the management of anesthesia practices. If you have never held a strategic planning retreat, this is a great place to start.
New first-time author, Justin Vaughn, tackles the timely challenge of succession planning with Passing the Baton: Grooming the Next Generation of Group Leaders. So many practices have great leadership and management today, but who will lead and manage them in the future? This is one of the truly critical issues most anesthesia groups need to address.
Funding a Private Investment Opportunity: Practical Tips for Physicians is brought to us by Cary Zimmerman, Esq. and Kathryn Hickner, Esq. They have offered a most interesting set of suggestions and considerations for investment opportunities for our readers. There is a plethora of good advice here.We hope you enjoy this issue and these different perspectives. That is our goal—to keep you informed with regard to the ever-changing anesthesia landscape and up to date with insights and strategies that will help you survive and thrive in 2020. As always, if there are specific topics that you would be interested in seeing in the Communiqué, please let us know.
Will you be at the American Society of Anesthesiologists Practice Management Conference 2020 in Las Vegas? We will be there in booth #317. Stop by and say hello!
With best wishes,
Tony Mira
President and CEO -
Chaos to Clarity: Resolving Strategic Issues
Will Latham, MBA
President, Latham Consulting Group, Inc., Chattanooga, TNAnesthesiology groups operate in a rapidly changing environment. The specialty faces many challenges, including pressure on reimbursement, hospital consolidation and the threat of consolidators.Amazingly, many anesthesiology groups attempt to navigate these troubled waters without an agreed-upon plan. In most cases, most of a physician’s livelihood (his or her work, his or her compensation) is tied up in their practice, yet many resist spending one day a year developing an agreed-upon plan for the future of their organization.
So, let’s review what groups work on at such planning retreats, and then discuss how groups approach a planning process.
Key Issues
Although groups face a number of similar challenges and key issues, their answers to such issues and their plans differ based on their particular situation. Here are some of the issues that we see anesthesiology groups wrestle with:
- Independence: Is it our goal to remain independent? If so, what strategies will we need to implement to continue to be independent? If not, what criteria should we use to select a partner?
- Current Relationships: What is the status of our relationship with those we provide service to? Could such relationships be strengthened? If so, how?
- Geographic Coverage: What geographic area do we intend to cover as a group? What are the benefits of pursuing new business? What is our approach to new business: avoid opportunities, respond to requests, vigorously pursue?
- Size of the Group: How large will the group become? Will we grow to fill the service needs of the market, or will we set an upper-end limit on the number of physicians in the group?
- Mergers: Should the group consider/ pursue mergers with other anesthesiology groups in the region? What advantages would such mergers provide?
- Recruitment: Where do we stand in regards to our staffing needs and work/life balance? Are we “fat,” or are we “thin”? Are we where we want to be in regards to staffing? Should we consider alternative work arrangements?
- Shareholder Track: Will the group continue to add anesthesiologists on a shareholder track, or will it have long-term employed physicians? Will the group limit the number of shareholders? What expectations (beyond quality clinical care) will be required to become a voting shareholder?
- Governance: Does our current governance system meet the needs of our current organization? Do we need to give authority to a smaller group to make certain decisions? What authority should be given? Do we have effective means to deal with disruptive physicians? How can we improve communication? Do we have a succession planning process in place?
- Compensation/Call: Is our compensation system achieving the goals of the group? Is our call fair and reasonable?
Two things to note:
- These are not all the issues that we see discussed, only the most common ones.
- You will note that the questions have been provided but not the answers. As previously mentioned, the answers depend on your situation. Getting to the answers for your group is what a strategic planning process is all about.
Strategic Planning Process
Most groups’ strategic planning effort revolves around a weekend retreat of one or two days, where the members of the group meet to discuss and resolve key issues and map out a plan for the future.
The time at the retreat is the most valuable time (getting everyone together is often a challenge) and the most expensive (multiply the number of people in the room times an estimated hourly rate); and, therefore, it is essential that the group utilize the time at the retreat effectively. To do so, the physicians should be interviewed or surveyed prior to the meeting, asking them the following questions:
- What do you see as the major strengths of the group? What is working well?
- What are its major weaknesses? What is not working well?
- What is going on in the environment that might represent opportunities for, or threats to, the group?
- How do you expect the local healthcare market to change over the next five years and how should your practice operate in that environment?
- What issues do you think the group should address at the planning retreat?
Those leading the planning process should review the results of the interviews/surveys for common themes, identify the key issues to be addressed and develop a set of work papers to guide the retreat.
The retreat itself typically follows the schedule as shown in Exhibit 1. There are two parts of this process to emphasize—ground rules and decisions.
Ground Rules
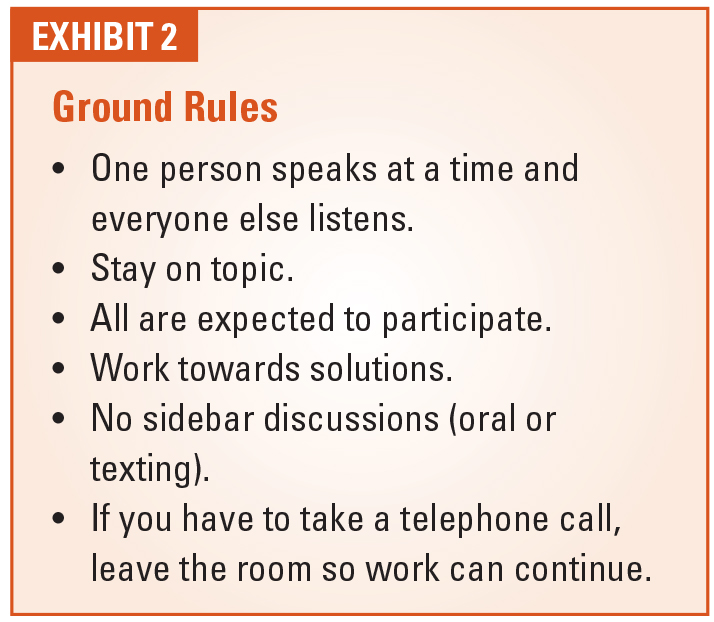
Most group meetings of anesthesiologists do not work very effectively. Discussions get sidetracked. Some individuals dominate the conversation, while others do not speak at all. People make telephone calls or do other disruptive activities during the meeting. Therefore, it is critical that one of the first things the group should do is agree on a set of rules that the “meeting manager” will use to manage the meeting.
We have found the ground rules as shown in Exhibit 2 to be those that are most essential. Notice that all of these are “observable behaviors”—behaviors that can be seen rather than guessed at (how do you really tell that someone is being “open-minded”?).
Decisions
It is unlikely that all members of the group will agree on all issues. So, what do you do when all do not agree?
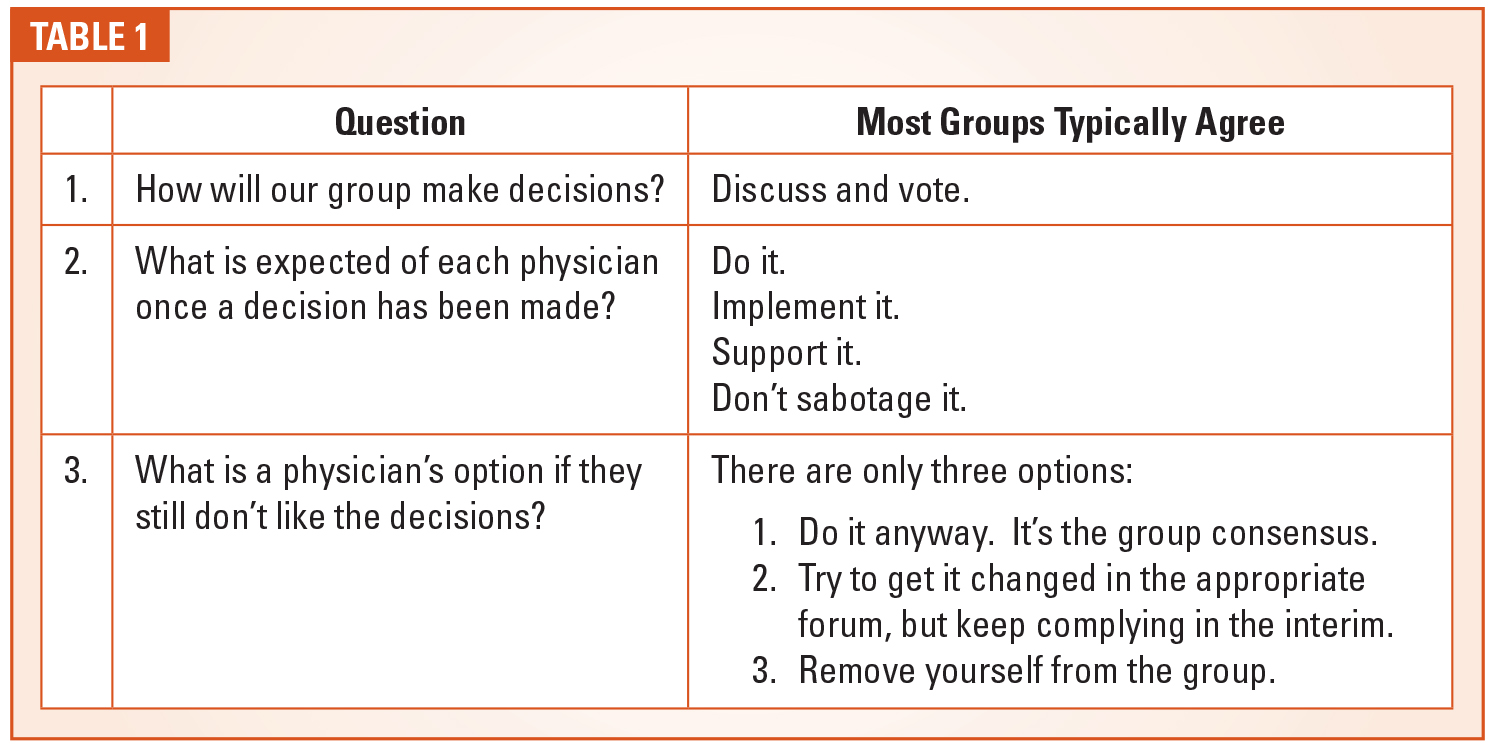
We believe that a group needs to pre-commit that all members of the group will support the decisions the group makes whether they agree with the decision or not. To do so, the group should ask and answer the following three questions as shown in Table 1.
(As a note, you are likely to find that 90-95 percent of the members of your group will completely agree with the thoughts in the “Most Groups Typically Agree” column. The remaining doctors may or may not agree or fulfill such commitments, but this gives the group the ability to challenge them if they don’t.)
Then, at the meeting, if consensus cannot be reached, the group should vote on the issue and move forward with the majority or super-majority position.
Large Groups
Larger anesthesiology groups (>30 – 40 shareholders) face a challenge when it comes to developing a strategic plan for their organization. There is a natural tension between shareholder involvement in the process and the ability to have the needed in-depth discussion to address key issues.
On the one hand, groups typically want to involve all the shareholders in the planning process, recognizing that the shareholders are more likely to support and adhere to the group’s plans if they have some input in the process.
However, trying to include dozens of shareholders in the detailed discussion to develop the plan is typically counterproductive. If a large group does this, one of the following typically happens:
- A smaller group of the attendees dominate the conversation (and most others “tune out”).
- Break-out groups are used to discuss specific issues. This can work well, but typically you cover less ground in these discussions and, at some point, you want to bring the whole group together to adopt the ideas of the small group.
- You choose a small number of topics with predefined motions that can be discussed and debated by the larger group in a very controlled manner.
As an alternative, we have worked with a number of groups that have followed a different path in developing their strategic plan—a path that balances inclusion and the ability to have in-depth discussion.In order to develop a physicianendorsed and useful strategic plan for a group of the size and diversity of most large groups, the planning effort includes a process to obtain feedback from all shareholder physicians (either through interviews or surveys). This is followed by a “planning retreat process” where the group leadership (the Board and selected others—20 or less individuals) will meet to discuss key issues, develop/update a group mission/vision, and develop overall objectives and goals for the group for the planning horizon. Finally, a full group meeting will be held where the plans will be reviewed and explained, and where the shareholders will be able to provide additional input to the plan.
A Final Word
Running the gauntlet of challenges and opportunities that can be found in today’s anesthesia business environment requires strategic vision and successful planning. Anesthesia groups must take deliberate steps to ensure the planning process is sufficiently inclusive and ultimately effective. The principles and recommendations outlined above may prove helpful in the achievement of these goals.
For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at WLatham@LathamConsulting.com. -
New Cases, New Tools in the Fight Against the “Company Model” Kickback Scheme
Mark F. Weiss, JD
The Mark F. Weiss Law Firm, Dallas, TX, Los Angeles and Santa Barbara, CAIt was a morning like any other. That is, until Pat, the president of Some City Anesthesia Group, Inc., got the call from Tracy, the president of Local G.I. Medical Group and its affiliate, Last G.I. Center Before Freeway, the ASC owned by Local G.I.’s seven gastroenterologists.
“Pat, your team does great work. I mean, you’ve covered every single one of our cases for the past seven years. The few times that there were problems, you solved them almost immediately,” Tracy said.
“Thanks,” Pat replied. “I really appreciate that. What can I do for you?”
“Well, we had our monthly meeting last night at the center, and the guys decided they need more control over anesthesia. You know, to make sure we have the right coverage from the right providers. Our management company told us that’s the right move. They’ve helped us set up Kick Back and Relax Gastrothesia, our own anesthesia group.”
“I don’t understand,” Pat said. “You just told me that we’ve provided great coverage for the past seven years.”
“Uh, yeah. Look, I’m not saying that your guys can’t keep working at the center. They can subcontract under Kick Back and Relax. It’ll pay Some City Anesthesia $1,100 a day for each of your guys on the schedule. Does that work? Heck, it’s win-win!”
"But Tracy, Pat stammered, "that's less than it costs us to staff the facility.”
“Sorry, Pat, but that’s more than what Kick Back and Relax has contracted to pay some independent contractors,” Tracy replied. “So, I’m just letting you know that the end of the month is your group’s last day. That’s when Kick Back and Relax takes over.”
You wake up sweaty and startled. What a nightmare!
Your cell phone rings. You glance at the screen. It’s that G.I., Tracy. You wonder what he wants.
The Company Model
As in the nightmare above, in its most direct form, the so-called “company model of anesthesia services” involves the formation, by the surgeon-owners of an ASC, sometimes in concert with others such as a hospital or a management company, of an anesthesia services company to provide all of the anesthesia at the facility.
In the typical scenario, prior to the formation of the company, all anesthesia services were provided by anesthesiologists, alone or in concert with CRNAs, either for their separate accounts or for the account of their anesthesia group. After the formation of the company, the anesthesiologists and CRNAs are employed or subcontracted by the company, with a significant share of the anesthesia fee being redirected to the company model’s owners, i.e., the surgeons.
There are other variants of the model, such as that in which the facility itself directly employs the anesthesia providers or controls the company that, in turn, employs them. However, for purposes of this discussion, the issues are relatively the same.
New Tools to Fight Back
In general terms, we can divide the fight against the company model into two major battlegrounds. The first is the litigation-focused battleground, chiefly False Claims Act (i.e., “whistleblower”) lawsuits and governmental action, including, but not limited to, criminal prosecution. We’ll call that “Domain 1.”
Anesthesiologists can certainly participate in Domain 1 as whistleblowers. However, for most groups the more fertile goal is to prevent, as opposed to prosecute, which leads us to the second battleground, “Domain 2.” It occurs at the scheme’s infancy. That’s when well thought out, smart and strategic attacks can quash the planned company model arrangement before it’s implemented, preserving the group’s business opportunity, professional independence and patient relationships.Of course, the strategies involved in Domain 2 are largely, although in truth not completely, based on the happenings in Domain 1.
This article focuses on the import of two relatively recent events, two new tools in the battle against the company model. The first is the situation that I’ll refer to as “Daitch and Frey” involving millions paid in settlement and prison time. The second is an announced $66 million settlement by Tenet Healthcare.
But, first, it’s essential that you understand the key compliance issues underlying an attack on the company model, as well as some of the prior, foundational events.
The Key Compliance Issues
For most anesthesia groups, the key compliance issue in the fight against the company model centers on its violation of the federal anti-kickback statute (AKS) and its state law counterparts.
The AKS prohibits the offer of, demand for, payment of, or acceptance of any remuneration for referrals of patients whose care is covered by federal healthcare programs such as Medicare, Medicaid and TriCare (among many others).
There are exceptions, known as “safe harbors,” that describe certain arrangements not subject to the AKS because they are unlikely to result in fraud or abuse.
The ability to fit with a safe harbor is voluntary. In other words, the failure to qualify for a safe harbor is not fatal for the parties to the arrangement; rather, a detailed analysis of the statute itself and of the facts of the deal is then required.
The AKS is a criminal statute. Violation can, and does, lead to fines and imprisonment. The submission of claims to federal healthcare programs in violation of the AKS serves as the trigger for violation of the False Claims Act. Additionally, in the situation in which a hospital is a co-owner of a facility at which a company model scheme is deployed, the same fact pattern can trigger a Stark Law violation by the hospital and the participating surgeons.
Broad OIG Guidance
The Office of Inspector General (OIG) of the U.S. Department of Health and Human Services is the agency charged with regulating and enforcing the AKS.The OIG has issued broad guidance applicable to the analysis of company model deals: its 1989 Special Fraud Alert on Joint Venture Arrangements, which was republished in 1994, and its 2003 Special Advisory Bulletin on Contractual Joint Ventures.
Note that the term “joint venture,” as used by the OIG in the alerts, is not limited to the creation of a legal entity; rather, it covers any arrangement, whether contractual or involving a new legal entity, between parties in a position to refer business and those providing items or services for which Medicare or Medicaid pays.
The OIG has made clear that compliance with both the form and the substance of a safe harbor is required in order for it to provide protection. The OIG demands that if one underlying intention is to obtain a benefit for the referral of patients, the safe harbor would be unavailable and the AKS would be violated.
Although each alert is illustrative of the regulatory posture of the OIG, the 2003 Special Advisory Bulletin is particularly on point in connection with analyzing company model structures. In it, the OIG focuses on arrangements in which a healthcare provider in an initial line of business (for example, a surgeon) expands into a related business (such as anesthesiology) by contracting with an existing provider of the item or service (anesthesiologists or CRNAs) to provide the new item or service to the owner’s existing patient population.
The 2003 Special Bulletin lists some of the common elements of these problematic structures in general—neither of the alerts are anesthesia-specific (or, for that matter, specific to any medical specialty). In the points that follow, I have substituted words such as “surgeon” and “anesthesiologist,” all in brackets, for the broader terms used by the OIG.
- The surgeon expands into [an anesthesia business] that is dependent on direct or indirect referrals from, or on other business generated by, the owner’s existing business [such as the surgeon’s practice or ASC].
- The surgeon does not operate the [anesthesia] business—the [anesthesiologist] does—and does not commit substantial funds or human resources to it.
- Absent participation in the joint venture, the [anesthesiologist] would be a competitor [of the surgeon’s anesthesia company], providing services, billing and collecting [for the anesthesiologist’s own benefit].
- The [surgeon] and the [anesthesiologist] share in the economic benefit of the [surgeon’s] new [anesthesia] business.
- The aggregate payments to the [surgeon] vary based on the [surgeon’s] referrals to the new [anesthesia] business.
Specific OIG Guidance
In addition to broad industry guidance such as fraud alerts, the OIG also issues specific guidance, that is, advisory opinions, upon request of parties to an actual or actually planned arrangement.Technically speaking, advisory opinions are binding only on the specific party requesting the opinion, called the “requestor.” However, they are used in the compliance context, including in connection with Domain 2 strategy, for their insight into the thinking of the federal enforcers of the AKS, that is, of the OIG.
Advisory Opinion 12-06
The OIG’s first pronouncement directly on the propriety of the company model came in June 2012, when it issued Advisory Opinion 12-06.
The anesthesia group requesting the opinion presented two alternative proposed scenarios, one of which was a company model structure in which surgeons, or their ASC, would set up an anesthesia company to hold the exclusive anesthesia contract at the surgeons’ ASC. The anesthesia company would engage the anesthesia group at a negotiated rate as an independent contractor to provide the actual anesthesia care and certain related services. The anesthesia company would retain any profit.
In its Opinion 12-06, the OIG stated that there was no safe harbor available in respect of the distributions that the surgeons would receive from their anesthesia company. The ASC investment safe harbor does not apply to protect distributions of anesthesia profits.
Even if the safe harbor for payment to employees applied, or if the safe harbor for personal services contracts applied, those safe harbors would protect payments to the anesthesiologists. But they would not apply to the company model profits that would be distributed to the surgeons, and such remuneration would be prohibited under the AKS if one purpose of the remuneration is to generate or reward referrals for anesthesia services.
Because, as mentioned above, failure to qualify for a safe harbor does not automatically render an arrangement in violation of the AKS, the OIG then turned to an analysis pursuant to the 2003 Special Advisory Bulletin and found that the physician-owners of the proposed company model entity would be in almost the exact same position as the suspect joint venture described in the bulletin: that is, in a position to receive indirectly what they cannot legally receive directly—a share of the anesthesiologists’ fees in return for referrals.
Therefore, the OIG stated that the proposed company model venture could potentially generate prohibited remuneration under the AKS, and the OIG potentially could impose administrative sanctions on the requestor. In other words, the OIG declined to approve the arrangement.
Advisory Opinion 13-15
On November 12, 2013, the OIG released Advisory Opinion 13-15 dealing with a situation closely akin to a “company model” deal. [Note to reader: In full disclosure, the author was counsel to the anesthesia group in its request for Advisory Opinion 13-15.]
Underlying 13-15 was a proposed arrangement whereby a psychiatry group performing electroconvulsive therapy (ECT) procedures at a hospital would capture the difference between the amount it collected for anesthesia to ECT patients and the per diem rate it would pay to the anesthesia provider.
Initially, an anesthesia group held the exclusive contact to provide all anesthesia services at a hospital (Hospital).
Then, in late 2010, a psychiatry group with a practice centering on performing ECT procedures relocated to the Hospital. “Dr. X,” board certified in both psychiatry and anesthesiology, is one of the psychiatry group’s owners.
In 2011, the anesthesia group began negotiating with the Hospital for the renewal of its exclusive contract. The Hospital demanded an initial carve out: Dr. X would be allowed to independently provide anesthesia services to ECT patients.
The following year, when negotiating the 2012 renewal, the hospital demanded amendments to the carve-out provision:
Dr. X would be allowed to provide anesthesia services to ECT patients and the anesthesia group would be required to provide coverage for Dr. X.
Pursuant to what was called the “Additional Anesthesiologist Provision,” the psychiatry group would determine if an additional anesthesiologist was needed for ECT anesthesia. If so, the anesthesia group would negotiate to provide those services. If the anesthesia group and the psychiatry group did not come to terms, then the psychiatry group or Dr. X could contract with an additional anesthesiologist.
Subsequently, the psychiatry group informed the anesthesia group that an additional anesthesiologist was needed. The parties began negotiating. .
Under the proposed arrangement presented to the OIG, the anesthesia group and the psychiatry group would enter into a contract pursuant to which the anesthesia group would provide the additional ECT anesthesia services. The anesthesia group would reassign to the psychiatry group its right to bill and collect for the services. The psychiatry group would pay the anesthesia group a per diem rate. The psychiatry group would retain the difference between the amount collected and the per diem rate.
OIG’s Analysis
The OIG has stated on numerous occasions that the opportunity to generate a fee could constitute illegal remuneration under the AKS, even if no payment is made for a referral. Under the proposed arrangement, the psychiatry group would have the opportunity to generate a fee equal to the difference between the amount it would bill and collect and the per diem rate paid to the anesthesiologists.The OIG found that the proposed arrangement would not qualify for protection under the AKS’s safe harbor for personal services and management contracts.
That safe harbor protects only payments made by a principal (here, the psychiatry group) to an agent (here, the anesthesia group); no safe harbor would protect the remuneration the anesthesia group would provide to the psychiatry group by way of the discount between the per diem rate their group would receive and the amount that the psychiatry group would actually collect.
Because failure to comply with a safe harbor does not render an arrangement per se illegal, the OIG then analyzed whether, given the facts, the proposed arrangement would pose no more than a minimal risk under the anti-kickback statute.
The OIG flatly stated that “the proposed arrangement appears to be designed to permit the psychiatry group to do indirectly what it cannot do directly; that is, to receive compensation, in the form of a portion of the anesthesia group’s revenues, in return for the psychiatry group’s referrals of patients to the anesthesia group for anesthesia services.”
The OIG concluded that the proposed arrangement could potentially generate prohibited remuneration under the AKS and that the OIG could impose administrative sanctions in connection with the proposed arrangement. In other words, the OIG declined to approve the arrangement.
Advisory Opinion 13-15 demonstrates a fact lost to many when discussing “company model” deals: they generally do not fit into an available safe harbor—either the personal services and management contract safe harbor or the employee safe harbor. Not only is this because payment is not set in advance and will vary with the value or volume of referrals, but even more fundamentally because those safe harbors apply only to payments from the principal to the agent, not to payments, that is, remuneration, from the agent to the principal. In 13-15, the discount that permits the referral source to profit from the arrangement is remuneration to the principal.
Second, although failure to fit within a safe harbor is not ipso facto fatal, the OIG illustrated that being put in a position to profit from one’s referrals raises significant concerns of prohibited remuneration—that is, of violation of the AKS. Note that payment of so-called “fair market value,” the supposed holy grail of anti-kickback analysis, is not a panacea. Deals that place the referral maker in the position of profiting from its referrals are highly suspicious even in the face of valuation studies and valuation opinions.
New Cases. New Tools.
With that background, let’s turn to our focus on the import of two relatively recent events, two new tools in the battle against the company model.
The first is the situation concerning two Florida pain medicine physicians, Drs. Daitch and Frey and their related entities, including an anesthesia “company.” The second is an announced $66 million settlement by Tenet Healthcare of a whistleblower action that involved a company model entity deployed at a surgical hospital.
Daitch and Frey
Jonathan Daitch, MD, an interventional pain management specialist, and Michael Frey, MD, a physiatrist and pain medicine physician, co-owned both a professional practice in Fort Myers, Florida, Advanced Pain Management Specialists, P.A. (Advanced Pain), and a facility, Park Center for Procedures, LLC (Center).
The two also formed a company model entity, Anesthesia Partners of SWFL, LLC (Anesthesia Partners), to be the exclusive provider of anesthesia services for Advanced Pain. Anesthesia Partners contracted with CRNAs to provide the anesthesia services.
In 2015, a CRNA at the Center filed a False Claims Act lawsuit, U.S. ex rel. Christine H. Oha, et al. v. Advanced Pain Management, etc., et al., alleging that Daitch, Frey and other defendants had engaged in various kickback schemes. Among the allegations were that Daitch and Frey unnecessarily ordered, and Anesthesia Partners unnecessarily performed, MAC and general anesthesia on patients undergoing pain management procedures.
Subsequently, the U.S. Government, via the Department of Justice, intervened in the case for the purposes of settlement.
Dr. Daitch got off relatively lightly. That is, lightly only in the sense the resolution involved a financial civil settlement, not criminal prosecution or the loss of his freedom. And, note that civil settlements are just that, settlements—they are not an admission of guilt.
According to the Department of Justice’s December 2018 press release, the government entered into a $1.718 million civil settlement with Daitch, which included the additional allegation that Anesthesia Partners contracted with CRNAs at contracted rates and then profited by billing the full amount to Medicare and Tricare.
Of course, that’s the same analysis as the OIG used in Advisory Opinion 13-15. If we substitute “the surgeon” (in other words, Daitch) for “psychiatry group” as used in that advisory opinion, the government’s position is that the company model is “designed to permit the [surgeon] to do indirectly what [the surgeon] cannot do directly; that is, to receive compensation, in the form of a portion of the anesthesia group’s revenues, in return for the [surgeon’s] referrals of patients to the anesthesia group for anesthesia services.”
In the words of the Department of Justice, “this arrangement resulted in improper remuneration to Dr. Daitch as one of the owners of Anesthesia Partners. The United States contends that Dr. Daitch’s ownership interest in Anesthesia Partners, and the remuneration he received through this ownership interest, induced him to refer his patients for anesthesia services to Anesthesia Partners.”Frey was not as lucky as his partner.
In a pre-packaged set of criminal charges and a simultaneous plea agreement, Frey pleaded guilty to two of the allegations against him. In return for his admitting guilt as to two counts of conspiracy to receive healthcare kickbacks, the U.S. government agreed not to charge him with additional criminal offenses relating to, among other things, “kickbacks related to his ownership of Anesthesia Partners”—in other words, for his involvement in the company model scheme.
In February 2019, Frey was sentenced to 18 months in federal prison and ordered to pay $472,112.88 in restitution, plus other fines and penalties.
In addition to the above mention of consistency with Advisory Opinion 13-15, the combined facts of the settled civil case against Daitch and the guilty plea in the criminal case against Frey are entirely consistent with the OIG’s position in Advisory Opinion 12-06. In that opinion, the OIG stated that there was no safe harbor available in respect of distributions that the surgeons would receive from their anesthesia company, and such remuneration would be prohibited under the AKS if one purpose of the remuneration is to generate or reward referrals for anesthesia services.
Tenet
In Tenet Healthcare Corporation’s November 2019 10-Q filing with the SEC (for the quarter ended 9/30/19), it disclosed that it reached an agreement in principle with the United States Department of Justice to pay $66 million and other costs to settle a whistleblower suit involving, among other serious allegations, its participation in a company model arrangement. Again, as mentioned above, civil settlements are not an admission of guilt.
The underlying False Claims Act lawsuit, entitled U.S. ex rel. Wayne Allison, etc., et al. v. Southwest Orthopaedic Specialists, PLLC, et al., centers around numerous Oklahoma orthopedic surgeons, their practice, Southwest Orthopaedic Specialists (SOS), the surgical hospital they created, Oklahoma Center for Orthopaedic and Multispecialty Surgery (OCOM) and the corporate entities that purchased and/or control the surgical hospital, Tenet Healthcare and its subsidiary, USPI.
Among other things, the suit alleges that SOS and other defendants, including Tenet and USPI, entered into an anesthesia company scheme under which they formed and operated an entity called Anesthesia Partners of Oklahoma, LLC, to which OCOM granted the exclusive anesthesia contract. The complaint alleges that, as a result, anesthesia company profits were distributed to those owners in a manner directly related to the volume and value of referrals by the SOS surgeons.
These allegations are of additional interest because they’re not along the traditional line of company model scheme attack. The common attack involves an allegation that there’s an inherent, forced kickback in the relationship between the surgeon or facility-controlled anesthesia company and the anesthesiologists and/or CRNAs it employs or engages. That’s the “discount” analysis discussed above in regard to Advisory Opinion 13-15 and Drs. Daitch and Frey.
Here, however, the allegations essentially attack the existence of the exclusive contract with the captive anesthesia company as an AKS violation (the SOS surgeons controlled approximately 2/3 of the OCOM’s revenue—their anesthesia company got the contract).
They also attack the fact that the surgeons’ referrals to OCOM were referrals to their anesthesia company; the surgeons’ profit distributions from the anesthesia company depended directly on the volume and value of their referrals to OCOM, another theory of AKS violation.
Today’s Bottom Line on the Company Model
The term “company model” is an industry descriptor of certain types of arrangements. It’s not the case that any specific law or regulation renders the company model per se illegal.
The AKS is a criminal statute, and, as such, intent to provide/accept remuneration to induce referrals must be proven. That means that the analysis is highly fact specific.
In similar fashion, when an alleged company model scheme underlies a federal False Claims Act (i.e., whistleblower) lawsuit, specific facts relating to the kickback-tainted claims for payment must be pleaded with particularity, although there is some variance among the federal court Circuits as to the required degree.However, those are Domain 1 issues, that is, challenges on the litigation and enforcement battlefront. The battle to be played out in Domain 2, that is, in connection with the strategy of defeating proposed company model arrangements into which surgeons or facilities attempt to force you, is not as unforgiving.
That’s because even if the “chance” of criminal conviction, or of civil judgment on the False Claims front, may be low, the criminal penalties (jail time, civil monetary penalties and debarment from participation in federal healthcare programs) and trebled civil damages judgments pursuant to the False Claims Act are high. Low odds, times high penalties, equals high risk.
Daitch and Frey and Tenet, combined with OIG pronouncements and other support, form a potent set of Domain 2 tools that, in the right hands, can be used to defeat a proposed company model scheme before it’s implemented, preserving your group’s business opportunity, professional independence and patient relationships.
Mark F. Weiss, JD, is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He is also the co-founder of a healthcare mergers and acquisitions advisory firm, Steering Advisors. He can be reached by email at markweiss@advisorylawgroup.com or at markweiss@steeringadvisors.com. -
Passing the Baton: Grooming the Next Generation of Group Leaders
Justin Vaughn, MDiv, CPC
Vice President of Anesthesia Compliance, MiraMed Global Services, Jackson, MISports Illustrated recently featured LSU’s Joe Burrow on its cover, along with the caption, “The Greatest Story in College Football.” It is a great story, a Cinderella story. It’s the story of a small-town Ohio kid who went to a big-time football program in his home state and was told he wasn’t good enough to start. In Louisiana, however, he found a place where coaches were willing to give him the reins of leadership and to spend sufficient resources in developing that leadership. With the help of a new offensive coach and a fair amount of Cajun cooking, Joe Burrow grew from an above-average player last year to 2019’s Heisman Trophy winner. He has obtained mythical status in Louisiana and has fans all over Ohio wearing the purple and gold.Developing leaders. Securing the future. These are critical goals in the realm of sports and should be in the professional world, as well.
So many of the client groups we serve are fortunate to have strong and able leaders. We see evidence of this as we meet with our clients, listen to their aspirations, and see the fruits of their success. Running and growing a successful anesthesia practice requires a unique set of skills. Not every anesthesia provider is going to naturally gravitate to such a role. Most clinicians want to focus on their professional specialty. They don’t necessarily wish to be saddled with the extra burden of being business managers. However, in most groups, there are those few (or that one) who have both the desire and acumen to take on the added mantle of leadership.
What happens, however, when that leader goes away? Let’s say you’re in a group that’s thrived under the stable leadership of a sole individual over the course of several years—the stalwart captain of a straight-sailing ship. He or she has been manning the helm year after year, but now that person is no longer there. People do step down. They retire. They resign their position. What happens now to your vessel? Does it suddenly veer toward the shoals of confusion, contraction or outright dissolution? The purpose of this article is two-fold: to bring your attention to the current need for leadership development within your group and to provide insight on how that might be accomplished.
Decide on a Model
Not every group has the same leadership model. Some have a long-term president who handles the majority of the daily decisions, drafts the meeting agendas, and provides a large measure of the strategic thinking on behalf of his or her colleagues. Other groups may operate on a more delegatory model where the various business-related responsibilities are shared among a core group within the larger entity. Still others have a practice administrator or, in the case of a hospital-employed group, a facility executive who takes on a large measure of the non-clinical tasks.
Regardless of the model employed, anesthesia groups cannot thrive or even survive without sound leadership. This involves more than mere management. Yes, it is important to have that person who can ably handle the group’s finances and schedule the important meetings and see to the details of daily business. Every entity needs a solid and reliable manager. Leaders, however, bring something more to the table. They have “the vision” and the capacity to cause others to catch that vision. So, ultimately, this is going to come down to putting the right people in the right positions. If your group model allows for promotion from within, then you need to implement a systematic training program to build up your leadership pipeline.
Develop a Program
Here, we will not be providing a simple five-step strategy, a one-size-fits-all training program, or a boilerplate “blueprint for better leaders.” While such items can be purchased from a consultant or obtained from a website, they are likely to prove ineffective and create future resistance to a program that will actually work.
Some time ago, the president of a large and growing “supergroup” based on the west coast went through several off-the-shelf leadership training modules. None of them worked—at least not for his group and their specific set of circumstances. So, he tried a different approach. He brought his colleagues together and asked for their suggestions and recommendations for a training program that would conform to the needs, structure, and dynamics of their group. In other words, he got buy-in from the very individuals who would go on to become the focus of the program. Together, the group hammered out a plan that was customized to their unique circumstances. The results were nothing short of staggering.
The two takeaways of this supergroup’s success story are that any leadership training program is going to need (a) group buy-in, and (b) customization. One size does not fit all, and getting others to weigh in gives them skin in the game. It creates unity, a spirit of joint-mission, and that leads to enthusiasm. This, alone, will help to reduce costly turnover and produce motivated learners.
Deliver the Goods
Ultimately, it is going to be up to the current group leadership to get this ball rolling. Personal interests will have to be subordinated to the greater good and long-term well-being of the group. So, what’s your game plan? How do you get this party started? Here are a few suggestions:
- List Your Own Ideas. Since you’re the leader, you probably already possess the gift for strategic thinking. I’m reminded of the scene in O Brother, Where Art Thou? where, in response to the question of who should take on the role of leader, Everett says, “Well, Pete, I figured it should be the one with the capacity for abstract thought.” If you’re the leader, chances are you’re already an idea person. Jot down those ideas on how to create a leadership training program. They may end up being among the best submitted.
- Outline Items to Discuss. Before calling a meeting of the group for the purpose of kickstarting a leadership training program, the current group leader should cobble together the meeting agenda, to include the purpose of the meeting and the general parameters to be discussed. Those might include:
- Proposal for a training program, generally
- Reason for such a program
- Program goals
- Best methodology for achieving program goals (e.g., shadowing current leader, mentoring program, monthly training sessions, committee appointments, attendance at business meetings)
- Timetables
- Balancing training with clinical responsibilities
- Compensation issues
- Discussion
- Next steps
- Consult with Others. Before calling a general group meeting, you—as the current leader—may want to share your plan, vision and ideas for the program with a select number of group members for their feedback. Once their input is received, you may decide a few tweaks to your ideas are in order. You are now ready to move forward with your recalibrated plan.
- Schedule and Hold a Group Meeting. Here is where you lay out the problem and your vision for resolving it. It will be up to the leader to determine the extent to which his/her own plan particulars should be considered. Again, to get buy-in, this meeting should include an adequate segment of time devoted to discussion, allowing the members to throw out their own ideas. You may want to consider including this meeting within a larger group retreat or long-term planning session.
- Finalize the Plan. The initial group meeting may not allow enough time for members to adequately consider and generate ideas relative to each of the program’s components. Ask them to submit their ideas by a certain date. You will then need to decide how the final shape of the program is to be determined (by you, group consensus, board vote?).
- Implement the Plan. Once the plan is finalized, pick a date for the commencement of the new training program. Start it. Stick with it. Don’t slack off on it. Consistency is the key. If you run into unanticipated kinks, don’t be afraid to adjust some of the program’s parameters.
Once more, the overall goal of such a plan is to build a cadre of up-and-coming leaders for that inevitable time of transition. Groups need to start grooming potential presidents and decision-makers from within their own ranks—individuals who have the right stuff and who can step in when the current captain steps down. This is a matter of long-term group prosperity, but it is up to current leadership to make it happen. As experts in the business of anesthesia, we encourage you in this effort and stand ready to assist in any way we can.
Justin Vaughn, MDiv, CPC, serves as vice president of anesthesia compliance for MiraMed Global Services. Mr. Vaughn has nearly 20 years of experience in anesthesia compliance and has been a speaker at multiple national healthcare events. He has written two books on compliance-related issues and is the author of numerous articles relevant to the anesthesia space. Justin can be reached at Justin.Vaughn@MiraMedGS.com.
 The cost of anesthesia care has become one of the most significant issues in the management of today’s anesthesia practices. This is not to say that quality of care is not important, but it has become a given. Ultimately the essential challenge facing virtually all practices is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the needs of the facility or facilities being served. The problem is that the options for generating more revenue are limited to three: enhancing fee-for-service collections; generating additional revenue from new services, such as nerve blocks and ultrasonic guidance for postop pain management; and negotiating subsidy support from the facility. None of these constitutes a quick or definitive fix.
The cost of anesthesia care has become one of the most significant issues in the management of today’s anesthesia practices. This is not to say that quality of care is not important, but it has become a given. Ultimately the essential challenge facing virtually all practices is to generate enough revenue to recruit and retain a sufficient number of qualified providers to meet the needs of the facility or facilities being served. The problem is that the options for generating more revenue are limited to three: enhancing fee-for-service collections; generating additional revenue from new services, such as nerve blocks and ultrasonic guidance for postop pain management; and negotiating subsidy support from the facility. None of these constitutes a quick or definitive fix. In any pro forma model the assumptions are critical and can have a significant impact on the result of the calculations. This model assumes a small community hospital where some of the ORs may run late but where the average room runs about eight hours. OB is unpredictable but tends not to be very busy.
In any pro forma model the assumptions are critical and can have a significant impact on the result of the calculations. This model assumes a small community hospital where some of the ORs may run late but where the average room runs about eight hours. OB is unpredictable but tends not to be very busy.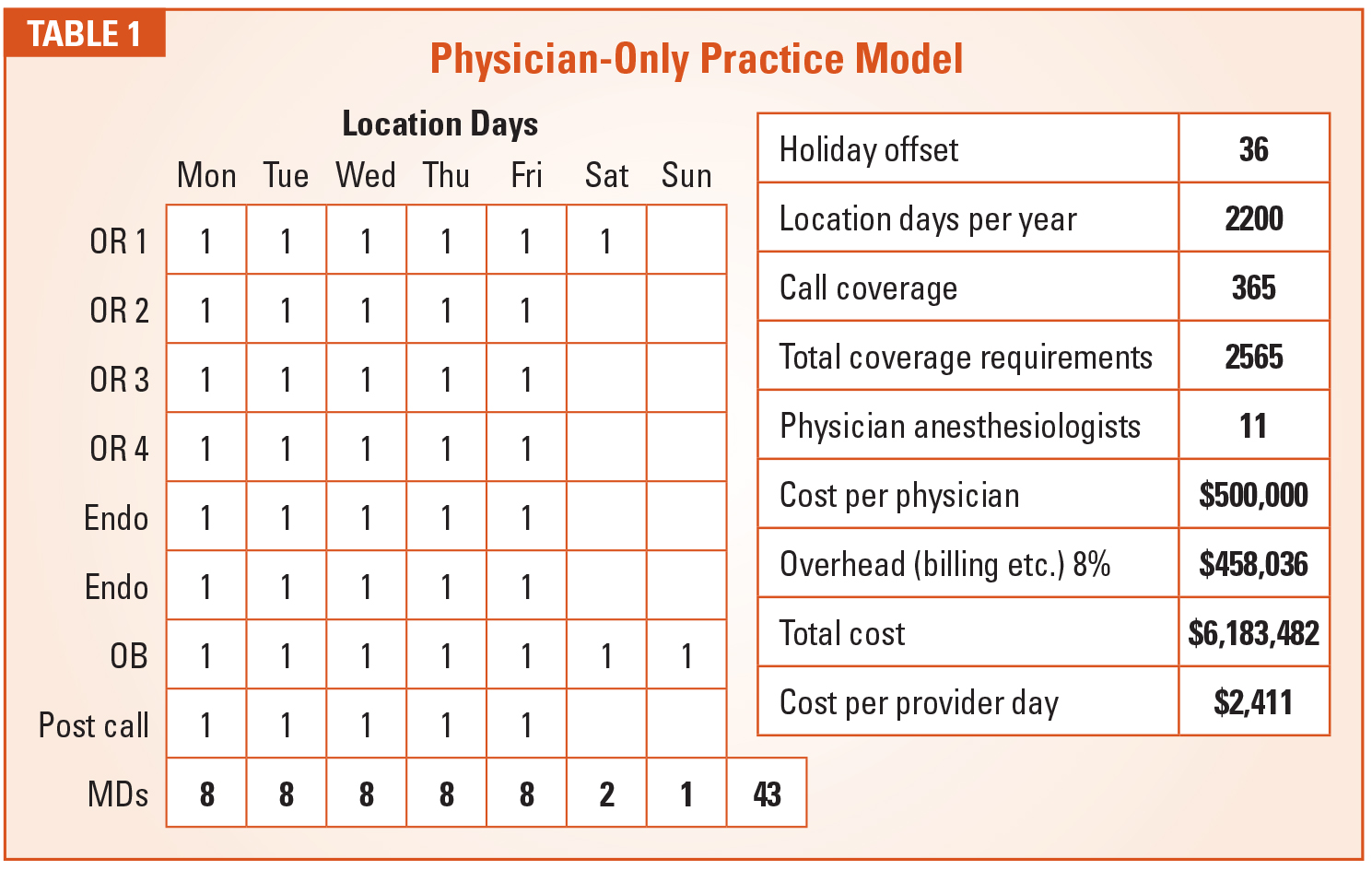
 There are some ways to reduce the cost of care for a physician-only model. Including non-shareholder providers who get paid at a lower rate may help some. The use of independent contractors who only have to be paid when they work may also be helpful.
There are some ways to reduce the cost of care for a physician-only model. Including non-shareholder providers who get paid at a lower rate may help some. The use of independent contractors who only have to be paid when they work may also be helpful.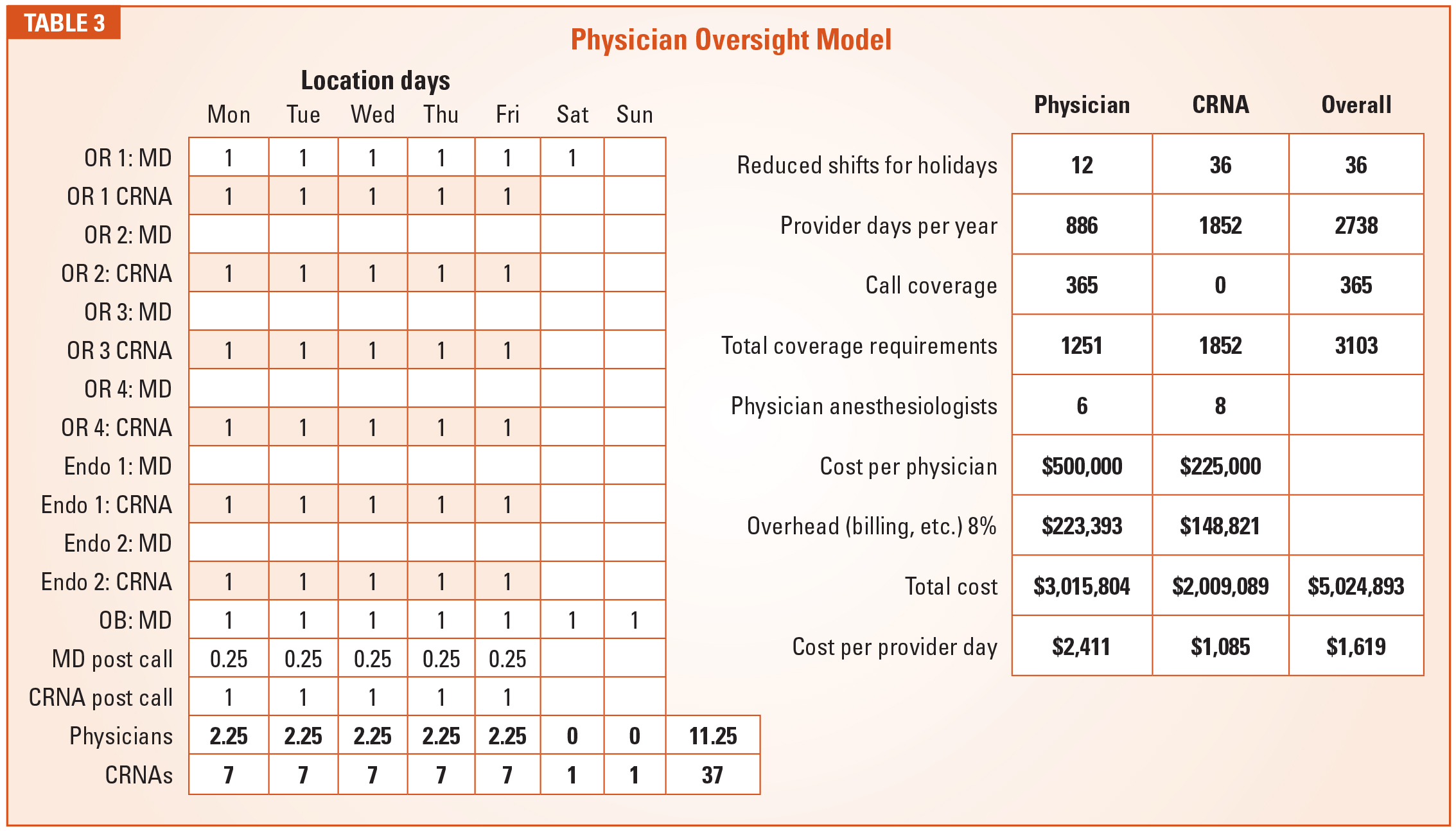
 We often say that the anesthesia department has more and better data about what happens in the operating rooms each day than any other department in the hospital. The question is whether the practice is using this data effectively to help the administration run the operating rooms more efficiently. This is becoming one of the new frontiers for the specialty. Sharing operating room utilization data is not going to be a quick fix to under-utilization, but its value cannot be ignored. Anesthesia providers need to be seen as team players in the management of the operating rooms and delivery suites. The more active a role they play, the more it will ultimately benefit their practice. This is the kind of out-of-the-box thinking that anesthesia practices should be pursuing as the cost of care becomes an ever more important factor in determining where patients get directed for the procedures they need.
We often say that the anesthesia department has more and better data about what happens in the operating rooms each day than any other department in the hospital. The question is whether the practice is using this data effectively to help the administration run the operating rooms more efficiently. This is becoming one of the new frontiers for the specialty. Sharing operating room utilization data is not going to be a quick fix to under-utilization, but its value cannot be ignored. Anesthesia providers need to be seen as team players in the management of the operating rooms and delivery suites. The more active a role they play, the more it will ultimately benefit their practice. This is the kind of out-of-the-box thinking that anesthesia practices should be pursuing as the cost of care becomes an ever more important factor in determining where patients get directed for the procedures they need. Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management
Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management  Funding a Private Investment Opportunity: Practical Tips for Physicians is brought to us by Cary Zimmerman, Esq. and Kathryn Hickner, Esq. They have offered a most interesting set of suggestions and considerations for investment opportunities for our readers. There is a plethora of good advice here.
Funding a Private Investment Opportunity: Practical Tips for Physicians is brought to us by Cary Zimmerman, Esq. and Kathryn Hickner, Esq. They have offered a most interesting set of suggestions and considerations for investment opportunities for our readers. There is a plethora of good advice here. Anesthesiology groups operate in a rapidly changing environment. The specialty faces many challenges, including pressure on reimbursement, hospital consolidation and the threat of consolidators.
Anesthesiology groups operate in a rapidly changing environment. The specialty faces many challenges, including pressure on reimbursement, hospital consolidation and the threat of consolidators.
 As an alternative, we have worked with a number of groups that have followed a different path in developing their strategic plan—a path that balances inclusion and the ability to have in-depth discussion.
As an alternative, we have worked with a number of groups that have followed a different path in developing their strategic plan—a path that balances inclusion and the ability to have in-depth discussion. For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at
For more than 25 years, Will Latham, MBA, has worked with medical groups to help them make decisions, resolve conflict and move forward. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of more than 135 medical practices representing over 1,300 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty healthcare conferences. He can be reached at  It was a morning like any other.
It was a morning like any other.  Anesthesiologists can certainly participate in Domain 1 as whistleblowers. However, for most groups the more fertile goal is to prevent, as opposed to prosecute, which leads us to the second battleground, “Domain 2.” It occurs at the scheme’s infancy. That’s when well thought out, smart and strategic attacks can quash the planned company model arrangement before it’s implemented, preserving the group’s business opportunity, professional independence and patient relationships.
Anesthesiologists can certainly participate in Domain 1 as whistleblowers. However, for most groups the more fertile goal is to prevent, as opposed to prosecute, which leads us to the second battleground, “Domain 2.” It occurs at the scheme’s infancy. That’s when well thought out, smart and strategic attacks can quash the planned company model arrangement before it’s implemented, preserving the group’s business opportunity, professional independence and patient relationships. The Office of Inspector General (OIG) of the U.S. Department of Health and Human Services is the agency charged with regulating and enforcing the AKS.
The Office of Inspector General (OIG) of the U.S. Department of Health and Human Services is the agency charged with regulating and enforcing the AKS. In addition to broad industry guidance such as fraud alerts, the OIG also issues specific guidance, that is, advisory opinions, upon request of parties to an actual or actually planned arrangement.
In addition to broad industry guidance such as fraud alerts, the OIG also issues specific guidance, that is, advisory opinions, upon request of parties to an actual or actually planned arrangement. The OIG has stated on numerous occasions that the opportunity to generate a fee could constitute illegal remuneration under the AKS, even if no payment is made for a referral. Under the proposed arrangement, the psychiatry group would have the opportunity to generate a fee equal to the difference between the amount it would bill and collect and the per diem rate paid to the anesthesiologists.
The OIG has stated on numerous occasions that the opportunity to generate a fee could constitute illegal remuneration under the AKS, even if no payment is made for a referral. Under the proposed arrangement, the psychiatry group would have the opportunity to generate a fee equal to the difference between the amount it would bill and collect and the per diem rate paid to the anesthesiologists. In the words of the Department of Justice, “this arrangement resulted in improper remuneration to Dr. Daitch as one of the owners of Anesthesia Partners. The United States contends that Dr. Daitch’s ownership interest in Anesthesia Partners, and the remuneration he received through this ownership interest, induced him to refer his patients for anesthesia services to Anesthesia Partners.”
In the words of the Department of Justice, “this arrangement resulted in improper remuneration to Dr. Daitch as one of the owners of Anesthesia Partners. The United States contends that Dr. Daitch’s ownership interest in Anesthesia Partners, and the remuneration he received through this ownership interest, induced him to refer his patients for anesthesia services to Anesthesia Partners.” In similar fashion, when an alleged company model scheme underlies a federal False Claims Act (i.e., whistleblower) lawsuit, specific facts relating to the kickback-tainted claims for payment must be pleaded with particularity, although there is some variance among the federal court Circuits as to the required degree.
In similar fashion, when an alleged company model scheme underlies a federal False Claims Act (i.e., whistleblower) lawsuit, specific facts relating to the kickback-tainted claims for payment must be pleaded with particularity, although there is some variance among the federal court Circuits as to the required degree. Mark F. Weiss, JD, is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He is also the co-founder of a healthcare mergers and acquisitions advisory firm, Steering Advisors. He can be reached by email at markweiss@advisorylawgroup.com or at
Mark F. Weiss, JD, is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He is also the co-founder of a healthcare mergers and acquisitions advisory firm, Steering Advisors. He can be reached by email at markweiss@advisorylawgroup.com or at  Sports Illustrated recently featured LSU’s Joe Burrow on its cover, along with the caption, “The Greatest Story in College Football.” It is a great story, a Cinderella story. It’s the story of a small-town Ohio kid who went to a big-time football program in his home state and was told he wasn’t good enough to start. In Louisiana, however, he found a place where coaches were willing to give him the reins of leadership and to spend sufficient resources in developing that leadership. With the help of a new offensive coach and a fair amount of Cajun cooking, Joe Burrow grew from an above-average player last year to 2019’s Heisman Trophy winner. He has obtained mythical status in Louisiana and has fans all over Ohio wearing the purple and gold.
Sports Illustrated recently featured LSU’s Joe Burrow on its cover, along with the caption, “The Greatest Story in College Football.” It is a great story, a Cinderella story. It’s the story of a small-town Ohio kid who went to a big-time football program in his home state and was told he wasn’t good enough to start. In Louisiana, however, he found a place where coaches were willing to give him the reins of leadership and to spend sufficient resources in developing that leadership. With the help of a new offensive coach and a fair amount of Cajun cooking, Joe Burrow grew from an above-average player last year to 2019’s Heisman Trophy winner. He has obtained mythical status in Louisiana and has fans all over Ohio wearing the purple and gold. Justin Vaughn, MDiv, CPC, serves as vice president of anesthesia compliance for MiraMed Global Services. Mr. Vaughn has nearly 20 years of experience in anesthesia compliance and has been a speaker at multiple national healthcare events. He has written two books on compliance-related issues and is the author of numerous articles relevant to the anesthesia space. Justin can be reached at
Justin Vaughn, MDiv, CPC, serves as vice president of anesthesia compliance for MiraMed Global Services. Mr. Vaughn has nearly 20 years of experience in anesthesia compliance and has been a speaker at multiple national healthcare events. He has written two books on compliance-related issues and is the author of numerous articles relevant to the anesthesia space. Justin can be reached at