Effective Hospital-Anesthesia Group Contracting: Understanding the Relationships Between Finance, Operations, and Compliance
Preparing for negotiations requires an appreciation of the other side’s needs, wants, values and constraints. Anesthesiologists who have contracts with their hospitals or surgery centers are in a continuous cycle of negotiations—as soon as one contract is signed, it is time to start working toward the next agreement. One good place to start in understanding the facility’s position is to look at the advice hospitals are receiving from their consultants. Below is an article recently written for that audience by ABC Vice President for Regulatory Affairs & Research Joette Derricks, CPC, CHC, CMPE, CSSGB. This article addresses hospital employment of physicians who bill using RBRVS Relative Value Units, and of course anesthesiologists use the Relative Value Guide’s Base and Time Unit methodology and typically have group exclusive contracts to provide services to the hospital’s patients, but the discussion below can be read with the differences in mind. It is important to know that hospitals may not even realize that anesthesia services have a unique relative value system. Relative Value Units are billed for pain medicine, critical care, and invasive monitoring lines.
There is no better place to start a discussion on effective hospital-physician contracting than jumping into the compensation model. Like the old time vaudeville act of spinning plates atop a stick—maintaining the right balance in your compensation system to please all parties is a hard act to perform. Each compensation model has its own risks and challenges. One methodology that is growing in popularity is a base compensation formula set on work Relative Value Units (“wRVUs”). The financial piece may be easy to deal with but a common pitfall from the operational/compliance side of the equation is the lack of understanding on how wRVUs are impacted by coding and billing decisions. The physician may perform four different services at the same encounter and generate 50 plus wRVUs but what happens when only 15 are reimbursed? Were the others “worthless work” as they are “bundled” with the base procedure and generated no additional compensation? Or perhaps the physician’s work effort was genuine quality work but the payer views this “quality” work as experimental and non-covered.
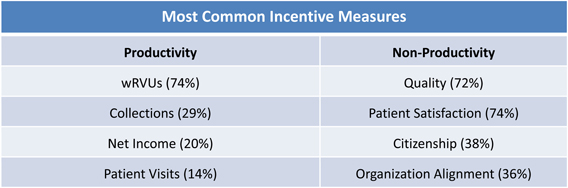
According to Sullivan, Cotter & Associates, Inc., 2011 Physician Compensation and Productivity Survey 86% of physician employers use incentive based pay system with 80% of the salary coming from some type of base formula and the remaining 20% comes from incentive payments. Incentives may be based on a wide range of factors and often incorporate multiple incentives. For example, 72% incorporate some incentive for quality into the compensation formula whereas only 38% consider a citizenship factor. The following chart, from the same Sullivan, Cotter report shows the most common factors used to incentivize physicians:
So what does quality look like? Does it mean the physician did the right thing at the right time and took care of the patient in the most efficient and effective manner? Isn’t this what the physician is supposed to do? What constitutes the reward? How is it measured? What changes are required to operations in term of the practice management or electronic medical record to document quality, bill for quality, track quality, and educate everyone on what quality is or isn’t?
The goal of every hospital-physician compensation system is to be competitive in the marketplace; fair and sustainable; easy to understand; consistently administered, and goal oriented to make the provider strive to reach and obtain a bigger and better target. The realities of every compensation system are: What is a physician really worth today? How do you reward individual and group performance in a highly complex regulatory world when the rules change before the ink is dry? “Easy to understand” is nearly impossible considering the tri-objectives of the finance, operations, and compliance forces that contribute to disclaimers and disclosures clogging the contract language.
Another aspect of the finance/compensation matrix that requires getting your hands around is data, data, and more data! You may have it but do you understand it? In developing reasonable and fair market value the question is are you using sound data? More physicians are seeking employment and more hospitals are employing physicians. Over 70% of hospitals have increased the size of their physician workforce in the last year and they all plan to continue doing so in the coming year. Coupling this trend with physicians’ desires to seek broader business opportunities in terms of ancillary services, joint ventures, medical homes, accountable care organization; most physicians, however, are no longer willing to provide services without their due compensation.
Other operational concerns that impact the financial picture of the hospital/physician contracting arena is fitting the gears of the quality, productivity, performance spectrum together so the physician enterprise actually runs smoothly. The hospital wants efficiency and cost effectiveness while the physicians want to see patients and not to worry about whether they ordered to many or too few tests or services for a particular patient. In addition to paying for quality, physicians are requesting payment for on-call for supervising mid-levels, and, of course, for those often problematic medical directorships.
Looking at the compliance side of this triangle hospital/physician contracts have a myriad of issues and risks to take into consideration. It is common knowledge that government regulations are growing along with government investigations. The Justice Department is aggressively pursuing fraud under False Claims Act, Anti-Kickback and Stark statutes. They are aggressive taking a firm stance on fair market value (FMV) issues. In fiscal year 2011, according to a Department of Justice news release, $5.6 billion in civil settlements and judgments were recouped—the largest recovery ever in a single year (more than double the recovery in 2008). Since January 2009, $15 billion has been recovered and according to the Justice Department for every dollar spent by them they recoup seven dollars in fraud recovery. What are the costs of potential non-compliance in terms of your hospital/physician contracts? The impact of non?compliance includes criminal, civil, and administrative exposure including potential for permissive exclusion from participating in all Federal Programs. Not to mention the harm to reputation and service lines impacted by any investigation/remediation and the costs associated with making it right. The hard costs of non-compliance include legal fees, consultant fees, administrative and executive time and resources.
Some of the red flags to watch for in terms of the compliance aspect of hospital/physician contracting that interplay with the financial and operational disciplines are:
- Declining financial performance with less conservatism in contracting
- No action plan to monitor impact of new legislation or market shifts
- High turnover in senior leadership
- Frequent, significant changes in estimates/costs/budgets
- Complex arrangements not well understood
- Arrangements appearing to serve little practical purpose
- Rapid expansion of activities/services without market changes
- Inconsistent contracting processes
- Lack of transparency
- Total compensation exceeds FMV
- Multiple contracts for individual or group
- Excluding pay for call, directorships or other duties in FMV evaluation of total cash compensation
- Unsigned or expired contracts
- The “impossible day”
- Providing excessive escalation in compensation models with high base compensation and graduated payment formulas
- Crediting physicians for services rendered by non?physician providers
- Contracts that “owned” by certain executives with no compliance review
The best advice is to pay attention to early warning signs and to ask questions! Two of the most important questions that should be asked by top executives and Board members with any physician contract are:
- Does this contract serve a legitimate business purpose?
- Has management provided sufficient data to understand the contract’s purpose and to make an informed decision regarding the legitimate business need for the contract?
Both questions require a resounding YES in order to proceed.
The relationship among finance, operations, and compliance disciplines within the hospital and the physician enterprise is critical—and often misunderstood. It is a complimentary relationship not a contradictory one. Organizational integration of these disciplines and effective compliance oversight of contracting process serves as the “safety net” for Board, Executives, Medical Staff and patients. In summary, effective hospital/physician contracts happen when all of the following questions have been considered:
- Who has oversight of physician compensation?
- What is your physician compensation philosophy?
- What is your contracting review and approval process?
- What arrangements are covered by the oversight process?
- Does compensation comply with fair market value and commercial reasonableness requirements?
- What are your documentation standards?
- How do you monitor or audit compliance with statutes, regulations, your process and your philosophy?
- How will physician compensation change in your organization with healthcare reform?
Measuring and compensating quality and value are challenges common to most, if not all, relationships between anesthesia groups and their hospitals. The interaction between financial, operational and compliance issues is critical internally within groups as well as in their hospital contracts. The bullet lists are directly applicable or adaptable to many of the ongoing professional relationships in which anesthesiologists and pain physicians engage.