2018 CPT Coding and Key Reimbursement Changes Pain Management and Anesthesia
- • The 2018 CPT edition includes 170 new CPT codes, 60 revised codes and 82 deleted codes along with two new modifiers. It is important to understand the changes and what should be documented to support the utilization of these codes.
- • The majority of the changes for 2018 were new CPT codes added to the Surgery section, Pathology/Laboratory section and the Category III section. Just to list a few of the changes, new codes for Esophagectomy (43286-43288) include the amount of esophagus removed (total/near total/distal two-thirds) along with approaches to code properly. Some of the Nervous System sections have been revised to include clarifying definitions for partial corpectomy services on the spine. Another area in the Nervous System is the Neurostimulator codes (64553, 64555, & 64561) which have been revised to include the placement for temporary or permanent percutaneous electrode arrays as the review resulted in the same work and practice expense for either temporary or permanent placements. CPT has added a parenthetical note stating the PENS (Biowave) and PNT are to be coded with the unlisted nervous system code, 64999 along with the application of the TENS unit CPT code, 64550. The detailed description of the actual service performed should be what is documented in the patient's medical record. CMS has also made changes to work RVUs for some services but the RBRVU information has not been published yet. Once it is published, the pertinent changes will be shared.
- • Office of Inspector General (OIG) has recently changed the bi-annual/annual Work Plan publication to a monthly update notification on its website. Under Reports & Publications there is an option for all reports and publications which has a Work Plan link under Strategic Communications. The details of the Work Plan and any changes/additions are listed for the public to view.
- • 2018 Anesthesia and Resource Based Relative Value System (RBRVS) Conversion Factors

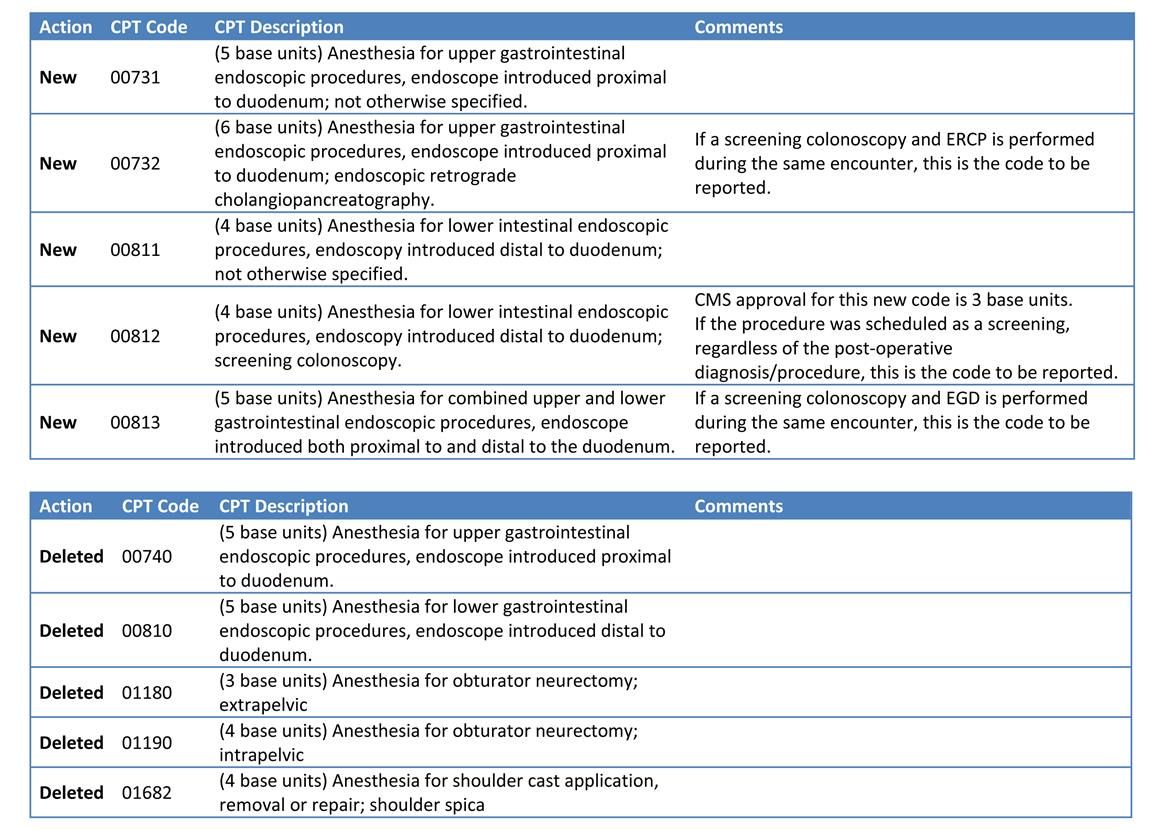
- • The two year streak of no changes to the Anesthesia CPT code set has come to an end. One of the major changes to Anesthesia is the deletion of the upper and lower endoscopic codes (see table below). This change greatly affects Anesthesia groups who perform anesthesia for gastrointestinal services. Not only have the two endoscopic codes been deleted, but five new codes have been created with a change in the base units from the deleted codes. Anesthesia providers should ensure that they understand the impact of potential revenue or compensation changes due to additions or revisions to the ASA 2018 CROSSWALK (Please refer to Appendix A - Summary of Additions and Revisions in the 2018 ASA CROSSWALK, for a complete list of the additions or revisions). These changes include CPT to ASA cross changes and alternative ASA code changes. Due to these changes the base unit values have been increased/decreased based on the change itself.
A Few Reminders Regarding Your Clinical Documentation
- • Radiology was a subject of change for 2016 with several code changes. The biggest change for anesthesia and pain management is the use of imaging guidance. A statement requirement has been added to the Introduction, Surgery and Medicine sections in the CPT 2016 Codebook and is still part of the CPT 2018 Codebook. The statement is "When imaging guidance or imaging supervision and interpretation is included in a procedure, guidelines for image documentation and report, included in the guidelines for radiology (including nuclear medicine and diagnostic ultrasound) will apply." The Radiology section also includes a statement for "written reports" which is "A written report (e.g., handwritten or electronic) signed by the interpreting individual should be considered an integral part of a radiologic procedure or interpretation. "Images" refer to those acquired in either an analog (i.e., film) or digital (i.e., electronic) manner."
- • The image interpretation and report should include the details of what the imaging was used for, the outcome of the use of the imaging, and the medical necessity and documentation that the image is on file/stored/saved, etc.
- • The dynamic technique, which is used throughout the procedure from initial vessel identification to the needle placement within the vessel, may be reported separately depending on CPT guidelines versus the static technique which is used only to identify the vessel and not used throughout the procedure. The static technique is not considered a reimbursable service.
- • CPT descriptors utilize imaging verbiage in different ways throughout the CPT code set. If imaging is required to perform the service (e.g., with imaging, including imaging, requiring imaging, inclusive of all imaging, etc.) the "written" requirement and image on file/stored/saved is still a documentation requirement. If the description verbiage "when performed" is included then the CPT code can be reported whether imaging is utilized or not. However, when it is utilized the same imaging documentation is required.
- • When Trigger Point Injections are performed, it is very important that the all muscles injected (by name) be documented along with laterality, because the coding is dependent on the number of muscles injected, not the number of injections.
- • Documentation of the patient's physical status and any co-morbidities are important to include on all anesthesia records. Often this information helps to support the medical necessity for anesthesia.
- • ICD-10: please remember to be as specific as possible in the diagnosis description when documenting and to include the condition, site/laterality, cause (how the injury/health condition happened, placed, activity, etc.), and qualifier (reason for, or due to, along with special details such as with/without bleeding/hemorrhage/obstruction, etc.) as applicable for each service performed. There is an ICD-10 hotline telephone number (1-800-544-6647 #1) as well as an e-mail address (ICD10.HelpDesk@Anesthesiallc.com) to assist with any ICD-10 related questions.