 One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
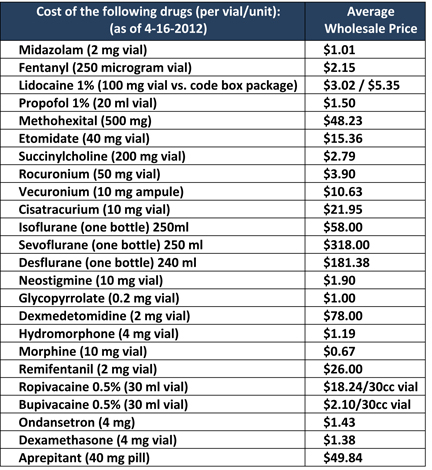
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...  It’s a tough world out there for anesthesiologists. At least, that’s what many anesthesiologists think.
Many believe that hospital employment is the panacea: the new “safe” career option. And why not—that’s the song that hospitals are singing loud and clear, and it’s the one they’re encouraging you to sing, too, via “alignment.”
Are anesthesiologists being guided into a safe harbor from the storm of uncertainty, or are they being lured by the siren song of a creature lethal to physician success?
Siren Song
In Greek and Roman mythology, sirens lured mariners to their deaths. Lethal creatures that they were, they didn’t kill with knives, spears, or other observable weapons; they didn’t even give rise to a threat.
Instead, they used their enchanting voices in song to lure their victims’ ships aground on the rocky shore.
Today, there are a number of trends creating a storm in the sea of medical practice....
It’s a tough world out there for anesthesiologists. At least, that’s what many anesthesiologists think.
Many believe that hospital employment is the panacea: the new “safe” career option. And why not—that’s the song that hospitals are singing loud and clear, and it’s the one they’re encouraging you to sing, too, via “alignment.”
Are anesthesiologists being guided into a safe harbor from the storm of uncertainty, or are they being lured by the siren song of a creature lethal to physician success?
Siren Song
In Greek and Roman mythology, sirens lured mariners to their deaths. Lethal creatures that they were, they didn’t kill with knives, spears, or other observable weapons; they didn’t even give rise to a threat.
Instead, they used their enchanting voices in song to lure their victims’ ships aground on the rocky shore.
Today, there are a number of trends creating a storm in the sea of medical practice....
Most practicing anesthesiologists know that the federal anti-kickback statute prohibits hospitals, ambulatory surgical centers and others from asking for something of value in exchange for the referral of patients for anesthesia services. Paying for the anesthesia franchise violates the statute. So does soliciting payment for the franchise.
As simple as this general principle would seem, the Department of Health and Human Services Office of the Inspector General (OIG) periodically finds it necessary to spell out the parameters again. Most recently, anesthesiologists who had an exclusive hospital contract requested and received an advisory opinion (No. 13-15) from the OIG stating that a proposed arrangement involving reassignment of fees to a psychiatry group and a per diem payment to the anesthesiologists “could potentially generate prohibited remuneration under the anti-kickback statute and that the OIG could potentially impose administrative sanctions." In other words, the parties would proceed with the arrangement only at their peril.
The...
The Centers for Medicare and Medicaid Services (CMS) does not conjure up the relative value units (RVUs) on which payment for individual procedures is based, although it may sometimes seem that way. A consensus group of physicians representing all the major specialties, convened by the American Medical Association (AMA), meets three times a year to develop recommendations for RVU adjustments. The recommendations from the consensus group (the Relative Value Scale Update Committee, or RUC) are sent on to CMS, which considers the information as it prepares its annual update to the Physician Fee Schedule. In recent years, CMS has adopted between 87.4 and 95 percent of the RUC’s recommendations, depending on which source you accept, Health Affairs or the RUC, respectively. The former figure represents 2,419 out of 2,768 recommendations that the RUC proposed between 1994 and 2010.Composition of the RUCThe RUC consists of 31 members, 28 of whom are eligible...
Last spring, we alerted readers to a proposed payment policy (“Local Coverage Determination,” or “LCD”) under which Noridian Administrative Services, LLC, the Medicare Administrative Contractor (“MAC”) for nine Western states, would have denied coverage for blocks and epidurals placed pre-operatively for the management of post-operative pain. In Proposed "Medical Necessity" Restrictions on Post-Anesthesia Pain Blocks, we criticized the proposed LCD for confusing the timing and the purpose of post-operative pain procedures and explained the process by which MACs propose, revise and finalize LCDs. We encouraged readers to use the process, and their representatives on the Carrier Advisory Committees of practicing physicians, to speak up for patients and help prevent undue restrictions on the availability of post-operative pain management services.
Unfortunately, although Noridian quickly corrected the section of the proposed LCD on “Nerve Blockade: Somatic, Selective Nerve Root, and Epidural” that would have prevented payment to anesthesiologists for performing procedures before or...