Taking Charge of Anesthesia Drug Costs
One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One recent research study found a 10-fold variation in the costs of intra-operative medications used in total knee arthroplasty cases. Douglas Hester, MD, assistant professor of anesthesiology at Vanderbilt University Medical Center, presented data showing that anesthetic costs ranged widely among providers, from $7.99 to $81.77. The median cost for 449 cases was $22.98 ($24.29 at one of the two institutions studied, with 229 cases, and $20.23 at the second institution, with 220 cases). (Wide Swings in Drug Costs among Anesthesia Providers. Anesthesiology News, September 2012.)
According to Dr. Hester, who presented the research at the 2012 Annual Meeting of the American Society of Anesthesiologists (Abstract 165), “The wide variations in drug use, and consequent costs, among anesthesia providers during similar cases are both an opportunity to minimize waste and a teaching opportunity.”
In an earlier study, led by Roy G. Soto, MD, associate professor of anesthesiology at Stony Brook University School of Medicine, residents, attendings and nurse anesthetists were asked in a survey to estimate the anesthetic costs for three routine cases of one, two and three hours in duration and involving the use of a total of ten anesthetic agents available as generic products. As reported in Anesthesia Providers Muff Drug Cost Test in the October 2007 issue of Anesthesiology News, the survey found widely varying estimates within each group but general consistency among them. All cost estimates were many times greater than the actual cost, with the total estimated costs ranging from four to 10 times the actual figures. Dr. Soto and his colleagues presented their findings at the 2007 ASA Annual Meeting (Abstract A1192).
Lack of knowledge as to anesthetic agent costs is not limited to the academic setting by any means. Franklin M. Dexter, MD, PhD (Economics of Anesthetic Agents) and others have noted “poor cost consciousness of anesthesia providers, particularly for expensive drugs.” Attention to spending generally takes a back seat to concerns for patient safety and the quality of care in inpatient and ambulatory surgery settings everywhere—fortunately. There is a growing awareness, however, that some spending on drugs may not be necessary. Variation in utilization that is not explained by differences in procedures or patients drives examination of clinical practices in general, and it must also drive assessment and understanding of appropriate utilization vs. inappropriate waste of anesthetic agents and other medications.
Basic drug costs are the product of unit costs and quantities utilized (the costs of preparing syringes, maintaining satellite pharmacies, ensuring safety and compliance, etc., are important but are beyond the scope of this Alert). As part of an exceptionally valuable tool available on the American Association of Medical Colleges website, a package of materials for introducing residents to the costs associated with anesthetic drugs (Ibinson J, Metro D. The Cost of Anesthesia Drugs Workshop. MedEdPORTAL; 2012. Available from: www.mededportal.org/publication/9212), Drs. Ibinson and Metro of the University of Pittsburgh Department of Anesthesiology provide the following average wholesale prices as of April 16, 2012 for common anesthesia drugs:
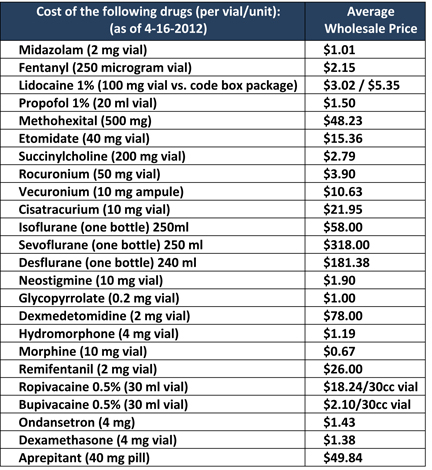
These prices should be considered an approximation or a starting point; they are 1.5 years old, and the prices negotiated at particular institutions are apt to be different from the average wholesale figure. They are nevertheless quite useful for purposes of raising awareness. The senior director of the Department of Pharmacy at Scott & White Healthcare, in Temple, Texas, was quoted thus in Keeping an Eye on Anesthesia Drug Costs (Pharmacy Practice News, November 2013): “we periodically will take the top 10 to 20 drugs used by anesthesia along with the acquisition cost and set it up in a table format, and place copies inside the lid of the anesthesia kit so everyone (anesthesia providers) can see current prices. It is a good practice to keep everyone aware of the costs because they change frequently with different manufacturers, or we switch from a branded to generic product, or a drug shortage occurs and the compounded price is typically considerably higher.”
Anesthesiologists may have little influence on drug acquisition costs, but familiarity with these costs and with ways to influence the quantities used will enable them to partner with their hospitals and ambulatory surgery centers to reduce excess spending, whether in TIVA, inhalational anesthesia or regional anesthesia. Cost savings are of benefit not just to the healthcare facilities but can be passed through to payers and to patients.
One established strategy to reduce the number of units of anesthetic agents used is reducing wastage of inhalation anesthetic agents, e.g., by minimizing excessive fresh gas flows. Others include drawing drugs into smaller syringes, using multidose vials, thus reducing waste, and:
- Alter the inhalational agent
- Add/remove muscle relaxant and reversal
- Change nausea prophylaxis
- Use dexmedetomidine instead of propofol TIVA and/or regional case
- Use bupivicaine instead of ropivicaine for regional case
(Ibinson & Metro.)
It is important to distinguish between measures that achieve savings in the short term and in the long term. Reducing waste and using less expensive medications are the only short-term changes that can reduce cost. They are also the simplest. (“Providing feedback to anesthetists of their overall mean fresh gas flows reduced consumption by 15% and 26% … Most of the benefit is from small reductions in flows for the many cases with rates < 3 liters per minute, not from changing the behavior of few providers with very big flows,” Dexter.) Reducing the amount of opened and unused drugs is simple conceptually and entails no adverse consequences for patients.
Drugs can also influence anesthetic times, and agents with higher acquisition costs can save money by reducing OR or PACU time. The calculation here is less simple, since, as Dexter puts it, “Translation of time into $ is sensitive to the percentage of costs that are fixed.” If a small number of minutes can be shaved from cases predictably, over a period of time, though, it may be possible to close a room or to reduce staffing in the PACU. Drug-selection strategies for achieving such long-term savings include (1) running patients “light” so that phase I PACU can be bypassed, and (2) administering a nerve block in the holding area, cutting OR time by approximately 12 minutes. (Dexter; Ibinson & Metro.)
The strategies noted are obviously not self-implementing. Simulation analysis at the individual institution is critical.
As Paul G. Barash, Bruce F. Cullen, Robert K. Stoelting, Michael Cahalan, M. Christine Stock observed in Clinical Anesthesia (Lippincott Williams & Wilkins 2012),
Anesthesia drug expenses represent a small portion of the total perioperative costs. However, the great number of doses actually administered contributes substantially to aggregate total cost to the institution in actual dollars. Prudent drug selection combined with appropriate anesthetic technique can result in substantial savings. Reducing fresh gas flow from 5 L/min to 2 L/min wherever possible has been estimated to potentially save $100 million annually in the United States.
In this era of accountability, the importance of evaluating cost-effectiveness in making clinical decisions is undeniable. Anesthesiologists can demonstrate their value through the thoughtful selection not just of anesthetic agents, but also of other drugs used throughout the perioperative episode such as pre- and post-op antibiotics and beta-blockers. Along with our forward-looking readers, we will be watching for more information and for new tools to share in this forum.
Find out more about our anesthesia billing and accounts receivable services.