The Medical Direction Team and Comparisons in Clinical Work Measures
Amr Abouleish, MD, MBA, Department of Anesthesiology, University of Texas Medical Branch
When an anesthesiology group is small and covers only one facility, the issue of “who is working hard” is moot. In a small setting, everyone can “see” everyone, and all the members take the same call and take the same time off. In contrast, as a group grows and begins to cover more than one facility, invariably there will be members of the group who think they do more work and should be paid more. In this situation, the group will need to reevaluate its compensation plans and how it measures “work done,” the majority being clinical work.
For clinical anesthesiology work, several categories of measurements can be used – all reflect the different types of compensation plans that exist in private-practice.i,ii Listed in order of prevalence, the systems used are based on (1) shift-worked (includes revenue split up equally), (2) charges or billed ASA units, (3) time billed,iii or (4) a combination. (I do not list “revenue-collected” since this is a measure of financial productivity, and not clinical productivity.)
 Each of these categories values work slightly differently and devalues different types of work. Briefly, shift-worked values availability to work and assumes everyone’s daily caseload will even out in the end (since it gives no value to the actual charges billed). Charges or billed ASA units values actual charges but those billed units are dependent on OR scheduling, surgical duration, and type of surgery.ivTime billed values anesthesia time with a patient and not total time worked (since any turnover time and down time are non-billable). And finally, a combination represents a group’s attempt to minimize the downsides of each category.
Each of these categories values work slightly differently and devalues different types of work. Briefly, shift-worked values availability to work and assumes everyone’s daily caseload will even out in the end (since it gives no value to the actual charges billed). Charges or billed ASA units values actual charges but those billed units are dependent on OR scheduling, surgical duration, and type of surgery.ivTime billed values anesthesia time with a patient and not total time worked (since any turnover time and down time are non-billable). And finally, a combination represents a group’s attempt to minimize the downsides of each category.
One factor that is essential to consider is the effect of anesthesia care team model on any comparisons of work done. When a group begins to consider measuring individual work, the group will invariably look at measuring work done “per doctor” or in business “per FTE” (where FTE = full-time equivalent). For a physician-only group, there is no problem with this methodology since the work done is done only by each member. On the other hand, once you introduce anesthesia care team model, then each doctor will be producing units billed in more than one room and the issue of staffing ratios becomes important to consider. It should be noted that this issue of staffing ratio is only important if billed units – either total ASA units/charges or time-billed – are used as the measurement of work.v
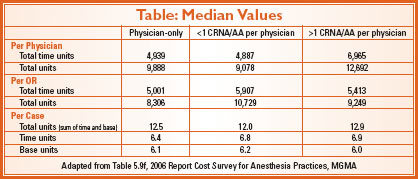
Since 2005, the MGMA has published an annual anesthesia survey entitled “Cost Survey for Anesthesia Practices.”vi In one of the breakdowns of the data, the data is presented by staffing models: physician only, 1 CRNA/AA per physician. The effect of staffing models is seen clearly when one looks at the data in these surveys. From the 2006 report, time and total units per case are almost identical among the three staffing models. (See Table) On the other hand, there is a marked differences between the models (especially between physician-only and >1 CRNA/AA per physician) when looking at time and total units billed per physician. This is not surprising since the medical direction groups bill more than one OR per physician while the physician-only group bills one OR per physician. On the other hand, when one takes the staffing model out of the equation, the work “per OR” shows fewer differences.
 Within a group that covers more than one facility, differences in staffing models may confound comparisons of any measurements similar to the survey data. For instance, if a group covers a traditional inpatient facility and a newer ambulatory surgical center (ASC), the group may choose to cover the inpatient facility with 1:2 to 1:3 MD: CRNA ratio but 1:4 in the ASC. In this situation, billed units per FTE will favor the ASC due to the increased staffing ratio. Another example is the way some groups cover cardiac anesthesia cases with physicians only, and other cases with medical direction. In this situation, the differences in staffing models would confuse comparisons using “units per FTE”. In conclusion, measuring and comparing clinical productivity is difficult. It is not surprising that so many anesthesiology groups choose to split the money up evenly or only track shifts worked. If a group does choose to use units billed as a measure, staffing ratio differences should be reviewed. Even if the group does not use units billed for compensation, they may use them to track group productivity.vii
Within a group that covers more than one facility, differences in staffing models may confound comparisons of any measurements similar to the survey data. For instance, if a group covers a traditional inpatient facility and a newer ambulatory surgical center (ASC), the group may choose to cover the inpatient facility with 1:2 to 1:3 MD: CRNA ratio but 1:4 in the ASC. In this situation, billed units per FTE will favor the ASC due to the increased staffing ratio. Another example is the way some groups cover cardiac anesthesia cases with physicians only, and other cases with medical direction. In this situation, the differences in staffing models would confuse comparisons using “units per FTE”. In conclusion, measuring and comparing clinical productivity is difficult. It is not surprising that so many anesthesiology groups choose to split the money up evenly or only track shifts worked. If a group does choose to use units billed as a measure, staffing ratio differences should be reviewed. Even if the group does not use units billed for compensation, they may use them to track group productivity.vii
NOTE: The Cost Survey for Anesthesia Practice is sent out every Spring, and the report is published in the late fall. The 2007 report has just been released. It is available at a discount for ASA members. Even better, every group completing the survey receives a copy of the final report free of charge. This article discusses only a small portion of the comprehensive survey.
i Abouleish AE et al. Measurement of individual clinical productivity in an academic anesthesiology department. Anesthesiology 2000;93: 1509-16
ii Blough GG, Scott SJ. Presentation of AAA survey on practice patterns at the ASA Practice Management Conference in San Antonio, Texas, on January 31-February 2, 2003
iii Feiner JR et al. Productivity versus availability as a measure of faculty clinical responsibility. Anesth Analg 2001;93:313-8
iv Abouleish AE et al. The effects of surgical case duration and type of surgery on hourly clinical productivity of anesthesiologists. Anesth Analg 2003;97:833-838
v Abouleish AE et al. Comparing clinical productivity of Anesthesiology groups. Anesthesiology 2002;97:608-616
vi Medical Group Management Association. Cost Survey for Anesthesia Practices: 2006 Report Based on 2005 Data. (Denver 2006)
vii Abouleish AE et al. Organizational Factors Affect Comparisons of Clinical Productivity of Academic Anesthesiology Departments. Anesth Analg 2003;96: 802-812