2014 CPT Coding and Key Reimbursement Changes
Joette Derricks, CPC, CHC, CMPE, CSSGB
Vice President of Regulatory Affairs & Research, ABC
The 2014 Current Procedural Terminology® (CPT) edition will have a total of 335 changes, including 175 new codes, 107 revised codes and 47 deleted codes for specialties.
No Anesthesia CPT codes were deleted, revised, or added for 2014. Changes to the 2014 CPT codes may impact some ASA 2014 CROSSWALK® determinations or base units. Anesthesia providers should ensure that they understand the impact of potential revenue or compensation changes due to additions or revisions to the ASA 2014 CROSSWALK (Please refer to Appendix A – Summary of Additions and Revisions in the 2014 ASA CROSSWALK for a complete list of the additions or revisions).
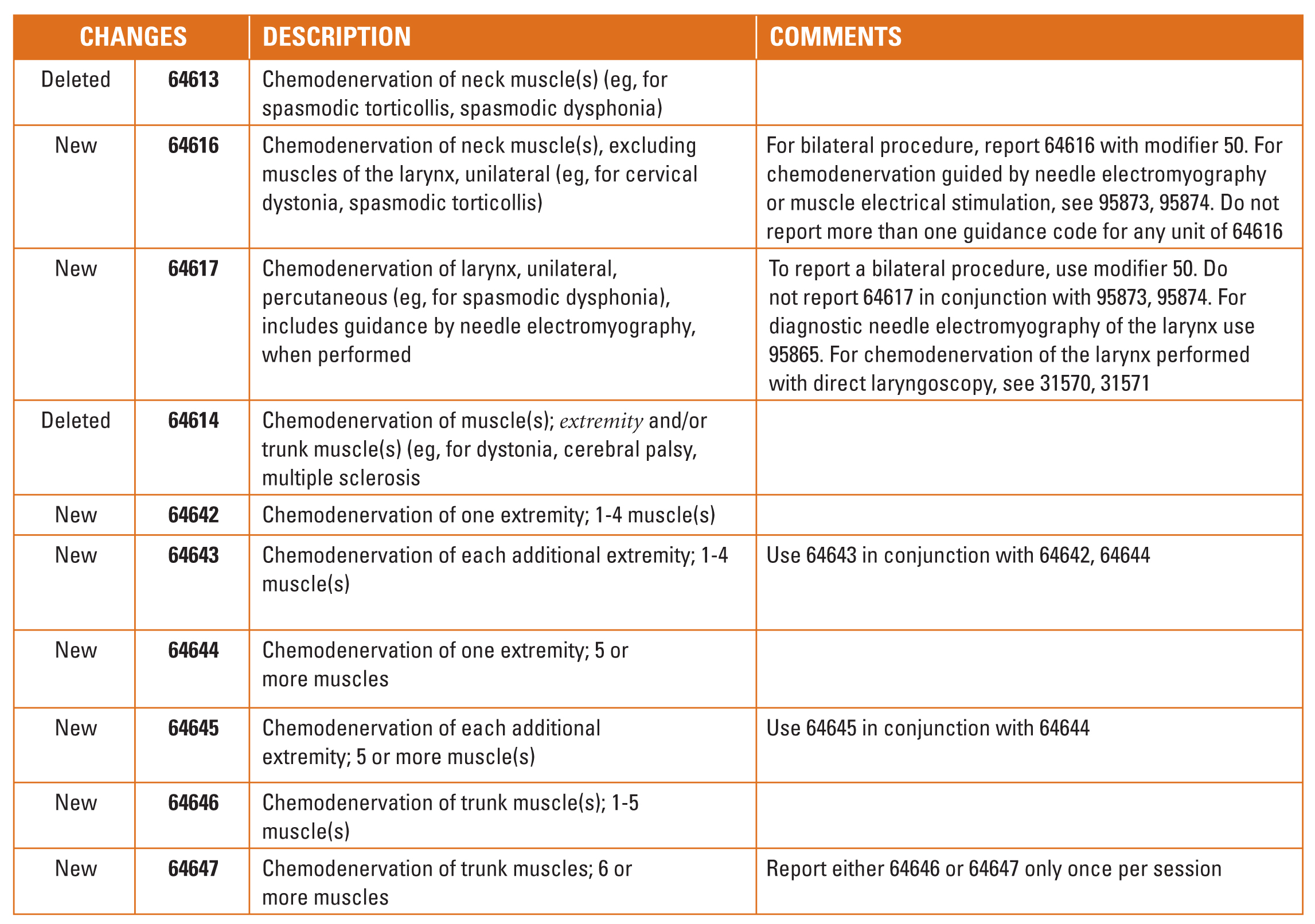
Pain management providers should take note of the additions and deletions in the chemodenervation subsection of the nervous system section of CPT 2014.
Nearly one-quarter of this year’s CPT code changes resulted from an ongoing two-year effort to revise gastroenterology codes to capture significant advances in endoscopic technology, devices and techniques. In recent years, miniaturization, powerful optical magnification and new imaging technologies have led to a wide variety of new applications for minimally invasive upper gastrointestinal endoscopic surgical procedures and improved diagnostic capabilities. Coding changes for lower gastrointestinal services can be expected for CPT 2015.
While the majority of CPT 2014 changes do not directly impact pain and anesthesia providers, it is important to note that changes to the CPT codes may result in changes in the work, practice expense, or malpractice relative value amounts and subsequent Medicare or other payer’s fee schedules. In 2014, Medicare made significant and substantial adjustments in these values that will result in reimbursement cuts beyond the 20.1% SGR cut. A few examples are shown in the table below.
A Few Remiminders Regarding Your Clinical Documentation
Moderate (conscious) sedation is billed based on the intra-service time which starts with the administration of the sedation agent(s), requires continuous face-to-face attendance, and ends at the conclusion of personal contact by the physician providing the sedation. Since moderate sedation is a time-based code the intra-service time must be documented in the medical record. In order to bill for the first 30 minutes of intra-service time, at least 16 minutes must be documented for 99144. An additional level, 99145, can be billed if 38 minutes of time is documented (each additional 15 minutes needs a minimum of 8 minutes).
When imaging guidance is not bundled in the surgical procedure it may be reported for the portion of the service that requires imaging as long as the documentation supports the medical necessity for imaging, and explains how it was used in the procedure, and that a permanent record of the image is maintained in the medical record.
Documentation of the patient’s physical status and any co-morbidities should be included on all anesthesia records. Often this information helps to support the medical necessity of the need for anesthesia and, more importantly, it may result in additional revenue.

Joette Derricks, CPC, CHC, CMPE, CSSGB serves as Vice President of Regulatory Affairs and Research for ABC. She has 30+ years of healthcare financial management and business experience. She is a member of MGMA, HCCA, AAPC and other associations and a regular speaker at practice management conferences. She can be reached at Joette.Derricks@AnesthesiaLLC.com.