The Proposed 2020 MPFS: What Anesthesiologists Can Expect
Summary
The recently released Proposed Medicare Physician Fee Schedule for 2020 contains several revisions to the E/M and QPP (MIPS) requirements, but little will change for the average anesthesia practice—except in the area of acute pain.
In the final days of July, the Centers for Medicare and Medicaid Services (CMS) released a preview of its proposed changes to the Medicare Physician Fee Schedule (MPFS) for 2020. The release also contained proposals that would affect the Quality Payment Program (QPP) for next year. Together, these recommended provisions constitute 1,704 pages of government-speak that will take some time to review and fully clarify. Nevertheless, we felt it important to provide you with our initial assessment of the "proposed rule," along with some of the highlights gleaned thus far. Here, then, is our first take on what's in store for anesthesia practices in 2020.
Conversion Factor
Each year, medical practitioners wait with bated breath for the release of the updated Medicare conversion factor (CF). After all, this is one of the key determinants of the level of reimbursement they will receive for their services. That said, the proposed CF for 2020 will most likely generate a collective yawn, for precious little will change. The proposed non-anesthesia CF provides an increase of only five cents—from $36.04 to $36.09 in rounded-off numbers. Furthermore, the rule recommended only a fractional increase to the anesthesia CF for next year, keeping it at the current rounded rate of $22.27.
Keep in mind that these are national conversion factors. The specific anesthesia CF applicable to your practice will vary based on your locality.
Impact of RVU Revisions
Regardless of the near negligible increase in the 2020 CF, practices may experience varying degrees of financial impact based on CMS' tweaking of various relative value units (RVU) components within each specialty code set. According to the American Society of Anesthesiologists (ASA), the payment impact for anesthesiology—based on RVU adjustments to the anesthesia code set—is expected to be negligible, while chronic pain providers may see an overall payment increase of one percent.
Anesthesia Coding Update
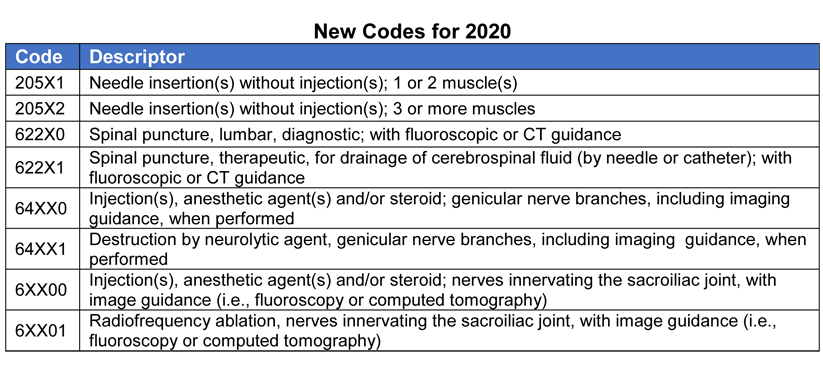
While there are no new or revised anesthesia-specific codes, the proposed rule does include new and revised codes for certain pain procedures. The rule also provided for a lowering of the RVUs for certain somatic nerve injections (CPT code range 64400 – 64450), meaning some of these codes will pay less in 2020. A full description of these RVU changes can be found beginning on page 331 in the current version of the rule.
The code for ultrasonic guidance (USG), CPT 76942, was only mentioned twice in the proposed rule. Those references indicated that (a) USG was used well over 50 percent of the time in tandem with many of the above-referenced injection codes, and (b) the American Medical Society's Relative Value Scale Update Committee (RUC) is considering recommending that USG be bundled with these injection codes beginning in 2021.
A list of some of the new codes that may be of interest to anesthesia or chronic pain practitioners is provided below.

The proposed rule also lists several new codes for "manual preparation and insertion of drug-delivery device," as well as codes for "removal of drug-delivery device."
More Changes for E/M
As you may recall, CMS had previously proposed significant changes to the way in which certain evaluation and management (E/M) services were to be documented and paid. However, those proposals were either altered or delayed in the 2019 final rule. With the proposed 2020 rule, CMS is once again moving the goal posts by proposing new revisions to their E/M documentation and payment policies, which include the following:
- Adopt revisions in E/M code descriptors, beginning January 1, 2021. The AMA's CPT Editorial Panel developed these new descriptors in an attempt to better capture the intention and requirement of each code.
- Table the previous plan to base payment on a blended rate for E/M levels two through four (2-4). Instead, CMS proposes to retain a separate payment amount for each individual level of service.
- Revise work and practice expense RVU calculations based on recommendations by the AMA Relative Value Scale Update Committee. Generally, E/M visits will provide increased reimbursement based on this re-weighting of RVUs, beginning in 2021.
- Retain five levels of coding for established patients, but reduce the number of levels to four for office/outpatient E/M visits for new patients.
- Revise the time component associated with each E/M code.
- Revise the medical decision-making process for all E/M codes.
- Require performance of history and exam only where medically appropriate.
- Allow clinicians to choose the visit level based on either (a) medical decision making, or (b) time.
Quality Payment Program
The Quality Payment Program (QPP) was enacted by Congress under MACRA and contains two sub-programs that seek to measure quality and cost: the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs). With that background in mind, here are some of the suggested program revisions for 2020 (most dealing with MIPS):
- Increase in the performance threshold [the minimum number of points an eligible clinician (EC) must attain to avoid a negative payment adjustment] from 30 points in 2019 to 45 points in 2020 and 60 points in 2021.
- Exceptional performance threshold to be increased to 80 points in 2020 and 85 points in 2021.
- Weight of the Quality performance category to be lowered to 40 percent in performance year 2020, 35 percent in 2021, and 30 percent in 2022.
- Increase weight of the Cost performance category: 20 percent in the 2020 performance year, 25 percent in 2021, and 30 percent in 2022.
- Implementation of a new MIPS Value Pathways (MVPs) reporting option, beginning with the 2021 MIPS performance year. Those ECs opting to participate via the MVPs framework would report a smaller set of measures that are specialty-specific, outcome-based, and more closely aligned to APMs.
- The low-volume threshold, EC types, MIPS performance periods, CEHRT requirements, and small practice bonus levels remain unchanged in the proposed rule.
- The MIPS Quality reporting threshold to increase from 60 percent of eligible cases per measure to 70 percent of eligible cases.
- Addition of a Multimodal Pain Management measure to the Anesthesiology Measure Set.
- Eligible clinicians or practices who fail to participate in MIPS in 2020, or to meet the 45-point threshold, may incur a negative nine percent payment adjustment in 2022.
The Proposed MPFS for 2020 will officially be published in the Federal Register later this month. Comments on the proposed rule should be submitted to CMS by September 27, 2019. Legal and compliance specialists at Anesthesia Business Consultants will continue to analyze the proposed MPFS and provide updates to our client-partners in the weeks ahead or as warranted.