The Evolution of Acute Pain Management in Anesthesia
Incorporation of acute pain modalities within anesthesia practices has greatly expanded over the years, and this has brought positive changes in patient care and physician payment. However, where new techniques become "standard of care," adjustments in payment often follow.
As the preeminent provider of outsourced anesthesia billing and management services in America, we are always interested in how anesthesia providers are modifying their practices to take advantage of new pain management modalities and changing patient expectations. Anesthesia is not just focused on the operating room and the delivery suite. It is increasingly concerned with the entire perioperative episode. That includes the diagnosis and treatment of the patient's post-operative pain.
Locke's Law
Seventeenth-century English economist John Locke is often credited with being among the first to describe the interplay between (a) the supply-popularity dynamic of a good or service, and (b) price. This "law of supply and demand" extends to the healthcare industry, as well. In other words, the more pervasive or routine a service becomes, the more the cost—and thus provider reimbursement—tends to decrease over time. To a large extent, however, acute pain has been an exception to this microeconomic maxim. The use of ultrasonic guided nerve blocks administered for the enhanced management of post-operative pain provides one of those unique opportunities to increase the quality of care and the financial viability of the practice, at least for now.
An Evolving Standard
The use of carefully targeted nerve blocks to provide an extended period of pain relief after emergence from anesthesia is not a new phenomenon. Interscalene blocks (ISBs), for example, have been a recommended option for shoulder surgery for more than 20 years. Historically, though, performance of this procedure was the exception rather than the rule. Not all anesthesia providers were equally competent in, or comfortable with, ISB administration. Now, however, it is safe to say that it is the exceptional shoulder procedure that does not include an interscalene block—usually administered with ultrasonic guidance (USG).
A Growing Revenue Stream
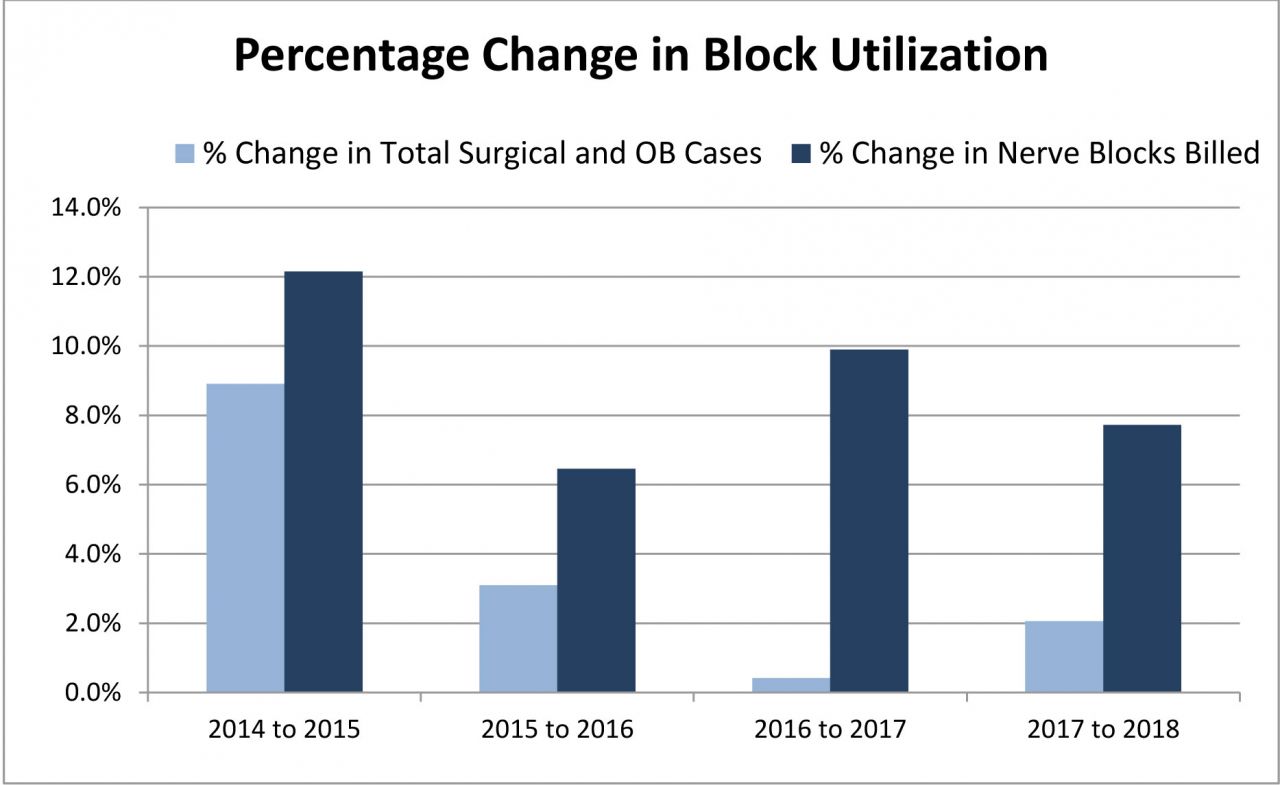
A review of nerve block usage by 17 of our clients across the country, over a five-year period, has revealed some interesting trends. The sample client list represents more than 500,000 cases performed, per year, in 13 states. Clearly, as seen in the following table, the use of postoperative pain blocks has increased relative to surgical and obstetric case volumes, which have tended to flatten in the past few years.

We believe that at least five factors have fueled this growth in acute pain administration, and there may be other, more subtle, factors at play.
- The ubiquitous availability of USG in virtually all clinical venues makes the administration of nerve blocks more accurate, more consistent and altogether safer.
- Patients appear to respond very well to the use of blocks as they make the recovery period more tolerable, especially in the case of painful shoulder procedures.
- While not all anesthesiologists have expertise in the use of nerve blocks, this is a discipline that is now integral to the training of today's residents, who go on to train older physicians.
- There is a growing body of evidence suggesting that the use of nerve blocks can minimize the need for opioids during the recovery period.
- Virtually all payers recognize both nerve blocks and USG as valuable services.
Keeping Track with the Trend
The increasing usage and recognition of acute pain modalities are reflected in the ongoing changes we find in America's medical coding canon. The CPT manual identified three primary acute pain procedures up until two years ago when new codes were added for TAP blocks. These procedures were interscalene blocks, femoral blocks and sciatic blocks, with each being defined quite narrowly by CPT based on the primary nerve sheath injected. What we are seeing now, however, is a dramatic expansion of available acute pain codes based on new approaches and techniques. For example, while Code 64415 is defined as a brachial plexus injection, most anesthesia providers perform variations on the theme—which our coders are able to accurately interpret and capture. The table below provides an illustration of these coding nuances, as well as their historic utilization.

Current Stability
With the development of new clinical techniques or a change in existing protocols, there will typically be a market response. For example, as the use of epidural steroid injections by chronic pain specialists increased in the last decade, payer rates started to drop. One could connect the creation of new codes for endoscopy with their lower base values as yet another example of this same market-driven dynamic. How, then, do we explain the fact that payer rates for acute pain services, as listed in the below chart, have remained relatively stable? Obviously, payers still recognize the clinical relevance and value of these services because the erosion in reimbursement has been quite limited.

Future Devolution?
There is, however, one rather significant cloud on the reimbursement horizon. Two years ago, USG was bundled into four commonly used spinal codes, 62310, 62311, 62318 and 62319. When the new codes were introduced for TAP blocks, USG was included and thus no longer separately billable. As we noted in a recent alert, the proposed 2020 Medicare Physician Fee Schedule (MPFS) indicated an intention to bundle USG into certain acute pain codes, beginning in 2021. Currently, the payment for USG represents about 20 percent of the average yield in an acute pain encounter.
In conclusion, the general population has greatly benefited from the growing usage and sophistication of acute pain modalities. Anesthesia practices have benefited, as well. Management of post-operative pain often includes two paying components: the block and the ultrasonic guidance. However, what has been an increasing revenue stream for most groups over the last several years is now seen as standard of care. This is the point at which government and commercial payers may take another look at separate reimbursement of one or both of these components. Initially, this may involve a reconsideration of USG only. Groups may want to begin contingency planning for an eventual bundling of USG and the potential revaluing of acute pain services, in general.
If you would like an analysis of your practice's use of acute pain techniques, please contact your ABC account executive, who will be happy to benchmark your utilization against our extensive data base.