The Anesthesia Strategic Challenge
With changes in hospital profit margins, it is time for anesthesia practices to take greater hold of their own financial reins. This will necessarily involve a different approach to their relationships with the administration.
Routine can be a good thing. It keeps us on track and hopefully continuing on a positive path. Every morning, you make up the bed. Every evening, you walk a mile. It's just what you do. Yes, routine is fine, as long as it doesn't become a rut or perhaps something even worse. Doing what we've always done before, in the same way we've always done it, can potentially be detrimental to our long-term wellbeing given the fact that the world around us is constantly changing. Perhaps we should do a little changing, too.
Just as it may be a good idea to occasionally reassess and readjust our daily routine, so should anesthesia practices reconsider the way in which they currently operate within the hospital system. Is the current arrangement with the administration still beneficial to the group? Will it foster future success? Today's article looks at the strategic challenges facing today's anesthesia practices.
What Is Wrong with This Chart?
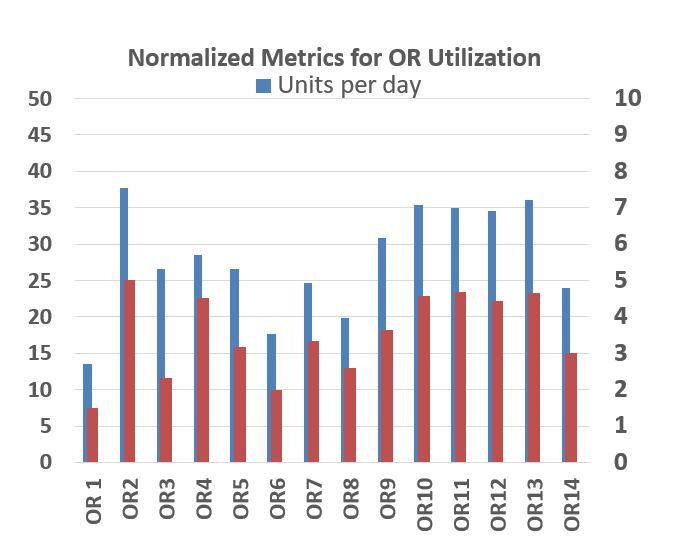
The below chart shows average billed units and billed hours of anesthesia care per location day for each of the 14 operating rooms in this hypothetical practice hospital. The problem is that, even with a reasonable payer mix and the resulting average yield per ASA unit billed, the operating rooms cannot generate enough revenue to cover the cost of providing the service, irrespective of staffing model. Conventional wisdom holds that a well-managed operating room should generate about 7 hours of billable anesthesia time or about 50 ASA units. Clearly, the practice presented here does not even come close to those levels of production. Obviously, this would be an unsustainable arrangement without a significant level of financial support from the facility. That is the option that most practices will choose. With each renewal of the contract term, they will try to project how much subsidy would be required to maintain a viable practice, where viability is defined as the ability to recruit and retain a sufficient number of qualified providers to meet the coverage and call requirements of the facility.
The problem is that the amount of subsidy needed is a moving target. What is true at one point in time—when the contract is being negotiated—may not be true later. The past two years of the pandemic have reminded us all just how variable and unpredictable operating room utilization can be. There is a saying in this business: "Anyone can get the number right today, but it will probably be wrong tomorrow."

The Historical Approach
Every time a hospital anesthesia contract comes up for renewal, both the anesthesia practice and the hospital brace themselves for a lengthy and often contentious negotiation. The facility wants to keep the process simple. For them, the cost of anesthesia is a line item in their annual budget. They want anesthesia to assume the risks for variability in OR and OB utilization. Their perspective is defined by what is often referred to as an FMV (Fair Market Value), which is often calculated by an independent consulting service. In the early days, hospital subsidies tended to be fixed annual payments to the department of anesthesia. More often than not, now they are defined as revenue guarantees—a kind of insurance that is intended to protect the practice from low collection months. There are examples of more creative approaches that involve formulas which relate to actual coverage and utilization, but these often frustrate and confuse the hospital's legal team.
The fundamental problem in all such negotiations is that each party has different objectives. In a competitive market environment, hospitals are competing for surgeon loyalty, which means that that are selling availability. The goal is to provide as many seven-thirty starts as a key surgeon might want. This is often the curse of the anesthesia department, which must dedicate staff to each early morning start regardless of whether the location will generate enough revenue to cover the cost of the providers. The chart above is a perfect example of this phenomenon. Opening 14 operating rooms may be good for surgeons, but it is a disaster for anesthesia.
What this means is that, if the hospital wants to provide this kind of availability, it must be willing to pay for unused operating room time. While many a facility has agreed to do that in the past, the economics of medicine have undergone a fundamental transformation over the past few years. Most hospitals are not as profitable as they once were, and this has greatly impacted their willingness to subsidize anesthesia to the extent they have in the past. This is the new reality that both parties must now address.
The New Paradigm
What needs to change? For starters, the anesthesia team and the hospital administration need to get on the same page with regard to the economics of anesthesia. The reality is that what creates value for anesthesia is the same thing that creates value for the facility. The more cases performed, the more revenue that is generated. Anesthesia just wants more cases to be performed in fewer anesthetizing locations. Getting surgeons to accept time slots that are convenient for anesthesia is the fundamental challenge here. Few administrators want to jeopardize the revenue potential of a loyal and profitable surgeon.
The good news is that the anesthesia department usually has more and more specific data about what actually generates revenue in operating rooms than the facility. Refining and sharing this data must be the first step is changing the paradigm. In short, the goal of anesthesia must be to become part of the solution rather than the problem. There is often a tendency to view the anesthesia department as captive to the goals and objectives of the facility. As is so often said in strategic planning, the truth is that the beliefs and strategies that got us to where we are today will not get us to where we need to be tomorrow. The key to success is a partnership approach to operating room management, and data is the key component.
The fact is that if the anesthesia providers and the hospital administrators are looking at the same utilization data; and, if they understand and accept its validity, they are more likely to come to the same conclusions as to what it means and what needs to be done. This must be an educational process, which takes time, patience and commitment. We all know that anesthesia providers can be very impatient; there are few clinical issues in the provision of anesthesia care that they cannot resolve within seconds or minutes. Working with administrators involves a different perspective and time frame. It involves focus and discipline.
What Needs to Happen?
Partnerships involve regular and consistent communication. Although this is less often the case than it used to be, many anesthesia practices only meet with administration to review contract terms when it is time to discuss a contract renewal. This is a perilous strategy. Trust is an essential component. The anesthesia team must commit itself to educating the administration and maintaining a dialogue focused on profitability and long-term success. The administration must accept the anesthesia management team as a key advisor and consultant. The very best practices have a member on the board of trustees of the hospital.
Contractual agreements must be based on an alignment of incentives. Three elements are critical to long-term success: accountability, collaboration and innovation. The group must have useful data to share and provide it regularly to administration. Many practices now have a standard utilization report they deliver monthly to the COO. It is particularly useful for the group's practice manager to meet with, and get to know, the key players in the hospital administration.
Anesthesia should be routinely identifying rate-limiting steps or process issues and proposing solutions. This is the best way to gain credibility with the key decision-makers. This is how collaboration should look: a productive dialogue to improve the operational performance of the operating room suites.
The point is the contract and its terms and provisions should be reflective of an ongoing dialogue and not a surprise. Key to the success of today's anesthesia practices is an understanding and appreciation of the hospital's customer service expectations. The practice needs to constantly validate that customer service expectations are being met.
What This Means
Anesthesia providers have long been the unsung heroes of the medical community. They have quietly and diligently provided an invaluable service. The time has come, though, for anesthesia to step out of the shadows and take more control of the essential factors that determine its members' income and lifestyle. It is a significant shift, but one that is essential and necessary for ongoing survival and success.
If you would like assistance in the strategies described above, please contact your account executive. You can also reach us by going to the following link: info@anesthesiallc.com.