The Anesthesia Challenge of Early Morning Starts
Summary: It is becoming more and more evident that, as cases move from the hospital to the surgery center, anesthesia staffing of the hospital becomes increasingly inefficient from a logistical and financial perspective.
One of the most significant challenges to hospital-based anesthesia practices is the need to make providers available to cover early morning starts. Typically, hospitals will define coverage requirements based on the number of early morning slots they want to make available to surgeons. The reason this turns out to be a problem is that these first-case-of-the-day-starts do not result in a line-up of to-follow cases. In fact, based on a review of a sample of HCA hospitals, 90 percent of the time surgeons perform only one case in the morning. They may then return to their offices to see other patients or take the rest of their line-up to an outpatient facility. The result is low levels of OR utilization in the hospital and an unprofitable situation for the anesthesia practice.
The percentage of surgical procedures now being performed in outpatient ambulatory facilities is increasing. Surgeons will often take their sicker Medicare and Medicaid patients to the hospital while they use the ambulatory facilities for their commercial patients. The resulting bifurcation of care is proving to be a major challenge for anesthesia on multiple levels. First of all, it is increasing the number of anesthetizing locations that must be covered, which impacts the number of anesthesia providers needed. Second, this decreases the average number of billable units generated per anesthetizing location such that the practice cannot produce enough revenue to cover the cost of the providers. Because the Medicare population is inevitably growing and because Medicare payments are significantly discounted, the revenue potential for hospital-based anesthesia care is eroding—all of which results in the need for ever larger subsidies.
In today's competitive healthcare environment, hospitals are looking at various options to lure surgeons to their facility. The most common enticement is the ability to offer surgeons early morning starts. In other situations, they will offer surgeons flip rooms. It used to be that one hoped that, if the surgeon brought his or her first case to the hospital, other cases would follow. Unfortunately, this is happening less and less frequently, based on the above-referenced HCA study. Unless the anesthesia practice also covers the outpatient facility, the rest of the surgeon's cases are of no consequence to the practice.
The table below represents a study of a hospital where a competitor has built an ambulatory facility literally across the street. The data was compiled for the ten most productive surgeons at a client hospital based on their actual case activity for the months of May and June 2022—in other words, for a period of 43 weekdays (Memorial Day was excluded). The purpose of the study was to assess the overall impact of early starts by looking at the percentage of cases booked during the first hour of the day, typically between 7 and 8 AM, and the average number of cases performed per day. The data is sorted based on the fifth column, the percentage of cases booked for the first slot of the day. Based on this sample, the CV surgeon, the neurosurgeon and the endoscopist had the highest percentage of early starts. It must be noted that this kind of analysis at other facilities might yield slightly different results depending on the specific market in which the facility operates.
It should be noted that CV and neurosurgeons usually start their cases early because their cases are generally long cases, especially in a facility with a limited cardiovascular case load. It also appears that endoscopy is not a significant line of business in this facility. Although the endoscopist performed 13 cases during this period, they were mostly early cases. Of particular interest was the impact of public payers, Medicare and Medicaid. For this facility, it clearly does appear that a disproportionate percentage of patients are covered by public payers. The exception is the endoscopist who does not appear to treat Medicare patients.

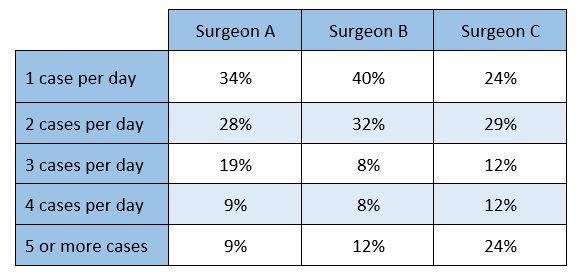
As a drill-down, we then examined the performance of the top three general surgeons at the facility. The question we really wanted to address was how much of the time they performed a single case and then went elsewhere. As the table below indicates, for all three surgeons, long line-ups of cases were the exception, rather than the rule. With one exception, surgeon C, only 20 percent of the days involved a line-up of four or more cases. It should be noted that this is consistent with an operating room utilization analysis that shows that, based on an eight-hour shift from 7 AM to 3 PM, the average room only generated about 3 hours of billable anesthesia time, which is well below the optimum productivity metrics. One can only conclude that, as is true in so many facilities, there is an inconsistency of operating room utilization.

This is a limited study of data from one facility, but the patterns appear to be consistent with other facilities served by our client anesthesia practices. So long as hospital administrators only think about trying to lure surgeons to their facility, they will have to pay for the inefficiency of the operating rooms with higher subsidies. Until there is a reconciliation of marketing strategy and economic reality, anesthesia practices will be continually challenged—especially given the current manpower shortage—to meet the expectations of administration. If you would like further information, please feel free to contact your account executive or email info@anesthesiallc.com.