A Day in the Life of a Chronic Pain Physician Assistant
Summary
What are the typical services performed by non-physician practitioners, such as physician assistants, within a chronic pain practice, and is there a way to optimize their value to the group? Those are the questions today's article will explore.
In last week's e-alert, we discussed the various policy issues associated with the use of nurse practitioners (NPs), physician assistants (PAs) and nurse anesthetists (CRNAs) in a chronic pain practice. That discussion raised a number of practical questions about the services that these non-physician practitioners (NPPs) actually provide and the economics of using these providers in a chronic pain practice. As a follow-up to that article, today's alert takes a deeper dive into the numbers. For the purpose of this discussion, we will focus solely on PAs.
Service Level Performed
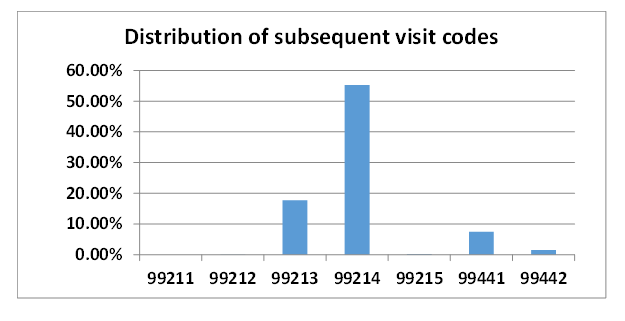
While many chronic pain practices do not employ PAs, some do. The following data is representative of those that do. About 82 percent of the typical day for a PA is spent on follow-up encounters with patients who were initially seen by the physicians. These encounters are represented by the seven codes listed below. The first five are for face-to-face services (99211-99215) and reflect the time spent with the patient and the complexity of the encounter. Codes 99441 and 99442 were allowed last year as a result of Covid and are for phone visits. The chart below is based on one month's activity: October 2020.

As you will recall from last week's alert, PA services can either be billed as incident to a physician's service or as a PA service, in which case the PA is paid at 85 percent of the physician payment. It is important to remember that, with incident-to services, the physician must have performed the initial work-up of the new patient, which the physician would then bill as either an initial visit or a consult.
Ancillary Service Opportunities
In addition to subsequent visit codes, PAs may also provide other services that might enhance the value of the practice. The following is a partial list of commonly provided services, although admittedly none of them will yield much actual revenue to the practice.

The use of PAs reflects the lower payment per hour for subsequent visits than the payment per hour for initial work-ups. While the physician will get paid between $150 and $200 for an initial work-up depending on the patient's insurance, the average payment for a follow-up visit is about $75, again depending on the payer mix for the practice. Presumably, the difference in payment is somewhat reflective of the difference in cost of the two categories of provider.
Impact on Practice
Ultimately, the financial impact of PAs is determined by their productivity. At $75 per encounter, the more encounters a PA can bill for, the more revenue they will generate for the practice. Based on our experience, optimum productivity is between 18 and 20 encounters per day. At this level, the average PA should be able to cover their cost to the practice. To some extent, this will serve as a barrier to entry for PAs. The practice must be able to provide sufficient activity to justify the cost of an additional provider.
As is true of most specialties, chronic pain physicians often talk about the potential value of PAs in their practice. In theory, it makes perfect sense. The physicians focus on the services that pay well, initial patient work-ups and procedural interventions, while the less profitable follow-up visits are covered by PAs. The fact is that very few clients have yet to work out the details of a mixed provider delivery model.
If you are interested in how to incorporate PAs into your pain practice, please feel free to contact your account executive or reach out to us at info@anesthesiallc.com. We will be happy to assess your productivity and profitability and make recommendations with regard to the potential integration of PAs.