2023 Medicare PFS Final Rule: A Deeper Dive
Repetition and addition—that's the formula for effective learning, especially when it comes to mastering a second language. You go over what you previously practiced and then add new vocabulary words or additional grammar nuances as you progress each day. At some point, you may even be provided various charts showing verb conjugation and noun declension. All these teaching strategies are aimed at helping the student gain a better understanding of the material.
Since its release last month, we have provided intermittent alerts on the 2023 Medicare Physician Fee Schedule (PFS) Final Rule (FR). In each alert, we have repeated some of the key takeaways, as well as add new details with each new publication. This alert is no different. We will build on information provided in our last article on the FR by diving even deeper into the details—especially as they pertain to the practice of chronic pain. We'll even throw in a few charts! There you go: repetition and addition.
General Coding Changes
The below chart reflects the number of changes found within the 2023 CPT manual, a publication of the American Medical Association (AMA). It should be remembered that PFS final rules typically follow the codes, code descriptors and parenthetical notes as found in each new edition of CPT. The FR for 2023 is no different in this regard. The CPT changes were verified and confirmed with the RVS Update Committee (RUC), as well as Medicare, before being finalized.

You'll notice that, while there were no coding changes relative to the specialty of anesthesiology, there were significant changes in evaluation and management (E/M) codes. We will look at these changes in more detail below.
E/M Highlights:
The first thing to note is that the entire set of codes reflecting Observation Care has been deleted. To specify:
- The Initial Observation Care code set (99218-99220) has been deleted. These services will now be reported with the Initial Inpatient E/M code set 99221-99223. The descriptors of the 99221-99223 have been revised to include initial hospital inpatient or observation care.
- Subsequent Observation care codes 99224-99226 have been deleted. These will now be reported with the Subsequent Inpatient E/M code set 99231-99233. The descriptors for 99231-99233 have been revised to include subsequent hospital inpatient or observation care in the description.
- Observation Care discharge code 99217 has been deleted. Hospital observation care discharge will now be reported with 99238-99239. The descriptors for 99238-99239 have been revised to include observation discharge.
When patient status is observation, the place of service (POS) will still be reported as 22 for on-campus outpatient hospital.
As it concerns non-observation E/M services, readers should note that the level one office and inpatient consultation codes, 99241 and 99251, have been deleted. This change was due to identical Medical Decision Making (MDM) criteria for levels one and two for these codes.
To further expand on a previous alert wherein we stated that E/M code level determination for 2023 will be based on either (a) time or (b) MDM (while requiring only a medically appropriate history and/or examination), we direct you to the below chart showing MDM and time requirements for Inpatient/Observation and Inpatient Consultations.
Inpatient/Observation/Consultation

Prolonged Services
A new add-on code (+99418) will be effective beginning next year to represent prolonged inpatient or observation E/M services. Below is the CPT description of this new code:
Prolonged inpatient or observation evaluation and management service(s) time with or without direct patient contact beyond the required time of the primary service when the primary service level has been selected using total time; each 15 minutes of total time (list separately in addition to codes 99223, 99233, 99236, 99255, 99306, 99310)
It is important to note that this code only applies to the highest level of visit per code set.
Endoscopic Bariatric Device Procedures
Codes 43290 and 43291 have been added to report esophagogastroduodenoscopy with deployment and removal of an intragastric bariatric balloon device(s). Code 43290 describes the procedure for deployment of the intragastric balloon and code 43291 describes the removal of the intragastric balloon. The above were previously reported with an unlisted CPT code.
Paravertebral Clarification and Guidance
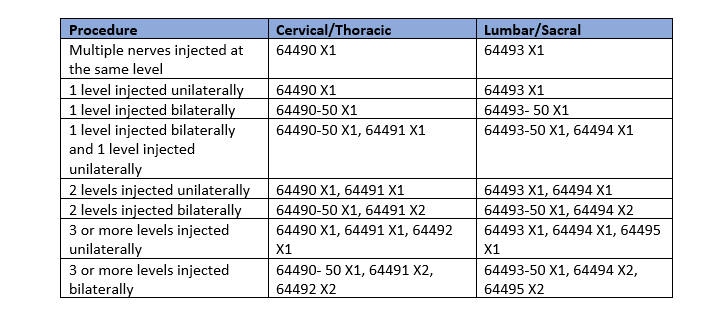
AMA/CPT provided additional guidance on the leveling of the paravertebral block procedures. CPT included guidelines and the chart below:
When the procedure is performed bilaterally at one level and unilaterally at a different level(s), report one unit of the primary procedure for each level and append modifier 50 for the bilateral procedure. If the procedure is performed unilaterally at different levels, report one unit of the primary procedure and the appropriate add-on code(s).

For unilateral paravertebral facet injection of the T12-L1 and L1-L2 levels or nerves innervating that joint, use 64490 and 64494 once. For bilateral paravertebral facet injection of the T12-L1 and L1-L2 levels or nerves innervating that joint, use 64490 with modifier 50 once and 64494 twice.
For more information on the 2023 PFS FR, please visit the CMS website. If you have questions for us, please contact your account executive or go to info@anesthesiallc.com.