January 13, 2014
As legal and regulatory obstacles dissipate and efficiency becomes ever more critical, telemedicine will be find uses beyond connecting rural clinics and hospitals with urban providers.
It is time for us to begin to familiarize ourselves with the role of telemedicine in anesthesiology. The concept is not entirely new; there have been several articles published on preadmission anesthesia or critical care consultations conducted through telemedicine. The results of a Canadian pilot study that appeared in Anesthesiology in 2004 showed “that preadmission anesthesia consultations using telemedicine technology can be successfully performed. Patients and consulting and attending anesthesiologists are very satisfied with telemedicine consultation.”
Tele-ICU systems are now able to monitor remotely about 10 percent of intensive care unit patients nationwide, as reported in the New York Times on April 14, 2013. We suspect that there may be more extensive applications right around the corner, and we hope to lay the groundwork for understanding these new applications as they arrive.
“Telemedicine” is commonly defined as the delivery of medical services and the sharing of medical knowledge between different locations using telecommunications systems. According to Girish P. Joshi, M.D. (Global Perioperative Patient Care Through Clinical Pathways, ASA Newsl. 2010 [74:8] 10-12),
Telemedicine is expected to play an increasingly important role in outpatient settings (e.g., home health care, remote patient monitoring, chronic disease management and rural health care) as well as in hospital settings (e.g., emergency department and ICU). Other applications of telemedicine include battlefield medicine, maritime medicine and aviation health care. Telemedicine provided in the critical care setting is commonly referred to as e-ICU. e-ICU has been proposed as a potential means of bringing the expertise of critical care specialists to hospitals with inadequate access to intensivists. Since e-ICU practice is still in its infancy, several areas of practice are not yet clearly delineated. . . . The practice of telemedicine may also be applicable to anesthesiology in which an anesthesiologist stationed in a room (within the operating area) could monitor multiple operating rooms. The telemedicine concept combined with automated anesthesia systems or closed-loop systems may further improve patient safety.
Although telemedicine and telehealth are still in their infancy, the industry is growing fast. An article in last month’s Forbes magazine predicted that telehealth will be a two billion dollar industry within five years, up from $240 million in 2013. The U.S. healthcare system’s quest for value—improved quality, delivered with greater efficiency—and developments including the shared savings programs of the Affordable Care Act will lead to increasing acceptance of telehealth’s ability to leverage individual physicians’ skills.
One important issue that has been keeping the brakes on the expansion of telemedicine is the lack of legal clarity regarding the types of healthcare services that may be delivered using tele-technologies. There currently are 50 separate sets of rules as to the care that can be provided. This often leaves both providers and patients in a state of uncertainty. Bipartisan legislation introduced in the House of Representatives in December, the Telehealth Modernization Act of 2013, would establish a federal definition of telehealth to provide guidance to states—13 of which have not adopted any legislation on the topic at all. The Telehealth Modernization Act, which is based on California legislation, is designed to incentivize more states to expeditiously adopt more favorable telehealth policies. It defines “telehealth” to mean:
with respect to health care that a health care professional is authorized to deliver to an individual in person under State law, such health care delivered by such health care professional to such individual not in person, from any location to any other location, and by means of real-time video, secure chat or secure email, or integrated telephony.
The proposed federal definition of telehealth would thus be broad enough to include both real-time and store-and-forward technology, such as communications systems that work like emails with attachments, and to cover home monitoring of patients.
Medicare enhanced coverage for telehealth services and increased facility fees for the originating site in the Final Rule on the Physician Fee Schedule for 2014. The Final Rule expands the geographic boundaries in which Medicare will cover telehealth services to include designated “health professional shortage areas” in rural portions of metropolitan areas that the Census Bureau defines as urban. It also updates the list of covered telehealth services (by CPT® code) to include the two Transitional Care Management codes (99495 and 99496) that were first covered last year. The Medicare-covered services are as follows:
- Initial inpatient consultations;
- Follow-up inpatient consultations;
- Office or other outpatient visits;
- Individual psychotherapy;
- Pharmacologic management;
- Psychiatric diagnostic interview examination;
- End-stage renal disease (ESRD) related services;
- Individual and group medical nutrition therapy (MNT);
- Neurobehavioral status exam;
- Individual and group health and behavior assessment and intervention (HBAI);
- Subsequent hospital care;
- Subsequent nursing facility care;
- Individual and group kidney disease education (KDE);
- Individual and group diabetes self-management training (DSMT);
- Smoking cessation services;
- Alcohol and/or substance abuse and brief intervention services;
- Screening and behavioral counseling interventions in primary care to reduce alcohol misuse;
- Screening for depression in adults;
- Screening for sexually transmitted infections (STIs) and high intensity behavioral counseling (HIBC) to prevent STIs;
- Intensive behavioral therapy for cardiovascular disease;
- Behavioral counseling for obesity; and
- Transitional care management.
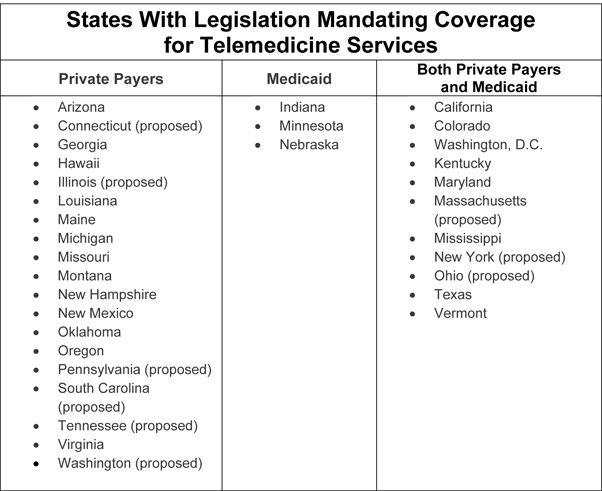
A major systemic obstacle to the dissemination of telemedicine has been the low level or lack of private or Medicaid payment for the service. The American Telemedicine Association reports that 23 states and the District of Columbia have adopted legislation mandating coverage for telemedicine services by both private payers and/or Medicaid. As of January 3, 2014, similar legislation is pending in nine other states. The table below groups the states by the payers targeted in their legislation.
A third legal impediment is the venerable prohibition on practicing medicine across state lines in a jurisdiction where the physician may not be licensed. The proposed bipartisan Telemedicine for Medicare Act, introduced in the House of Representatives last year, would permit licensed physicians and other practitioners to provide healthcare services to Medicare beneficiaries in other states and would explicitly invalidate any requirements that the out-of-state practitioner providing such services obtain a local license or other authorization.
Other telehealth-related federal legislation introduced in the last Congress includes the Health Savings Through Technology Act, which would create a 19-member commission to research best practices for using tele-technologies to lower healthcare costs and provide recommendations for how to incorporate them into federal healthcare programs, and the Telehealth Enhancement Act, which would adjust Medicare payments for home health services to account for the use of remote patient monitoring and provide coverage for home-based video services for homebound or hospice beneficiaries, among other reforms.
In some cases, the growth of telemedicine has been limited by lack of physician support, as well as by poor implementation. It appears that greater physician support may be developing. Indeed, at one rural hospital in Wisconsin, which implemented a tele-ICU program five years ago and reported ICU and hospital mortality rates and ventilator days 26 to 40 percent better than predicted, “Hospital officials also found the presence of the tele-ICU system made it easier to recruit physicians, as the program helped reduce night and weekend calls while maintaining high quality of care for patients.” (Gregg H. 3 Hospitals That Have Seen Positive Results From Tele-ICU Programs. Beckers Hospital Review, January 7, 2014)
The telemedicine consultations that were the subject of the 2004 Canadian study referenced in the first paragraph of this Alert involved an anesthesiologist who was:
present at the consultant site while a nurse accompanied the patient at the remote site during anesthesia consultation. The anesthesiologist took a history from the patient as in a conventional consultation. Examination of the airway and respiratory and cardiovascular systems was performed. Mouth opening and the Mallampati score were assessed using the airway camera. The patient was then turned, and a side-view visual assessment of the airway profile, thyromental distance, and neck movement was made using the room camera. The digital stethoscope was used to auscultate the heart and lung sounds. The nurse at the remote center was instructed on the positioning of the stethoscope on the patient’s chest and precordium. The rest of the consultation was conducted as per a conventional consultation.
The authors suggested that the high satisfaction scores given by the physicians in the study might have to do with the nature of the preanesthesia evaluation:
Because the physical examination by the anesthesiologist consists primarily of airway examination and heart and lung auscultation, the telemedicine format lends itself well to anesthesia consultations. The airway camera enables the anesthesiologist to assess the airway in a manner similar to that of a conventional consultation, but with better visualization of the posterior pharynx because of illumination. The digital stethoscope allows adequate examination of the cardiovascular and respiratory systems.
They also noted that:
There are several limitations to the telemedicine consultation process. First, there are privacy concerns for the patient because they are being asked to provide personal details and exposure of the chest for auscultation. Second, telemedicine consultation does not permit any physical contact between the physician and the patient. Third, the patient and the anesthesiologist cannot speak at the same time.
Those limitations are apt to give way in the face of the advantages of telemedicine. As stated by Galvez and Rehman in Telemedicine in anesthesia: an update (Curr Opin Anaesthesiol. 2011 Aug;24(4):459-62) in their Purpose of Review: “Advances in health information technology and broadband Internet connections provide novel opportunities for anesthesiologists to extend perioperative consultation services to remote geographic areas. Increasing economic pressures on healthcare delivery systems make initiatives such as telemedicine, which reduce costs while achieving excellent outcomes, an attractive option.” They also note the development of telemedicine programs in not just intraoperative consultation, postoperative management and critical care, but also in simulation and education.
Growth will also be driven by the shortage of physicians in rural areas and the increasing numbers of patients with chronic diseases—and by the continuing development of the technology as well as its users. A Stanford medical student recently wrote, in The Sacramento Bee, that “Students currently in the medical education pipeline started using smartphones and Skype in high school. The same can be said for many patients. Telemedicine can translate that familiarity with communications technology into a meaningful doctor-patient relationship."
TelePREOPTM is ABC’s latest clinical technology partner. It will be launching at the ASA Practice Management Conference in Dallas, TX on January 24. This service brings together telemedicine and preoperative software (ePREOP) to provide an economical solution to screen one hundred percent of surgical patients. We look forward to seeing you there.
With best wishes,
Tony Mira
President and CEO